Prolonged malnutrition can decrease the metabolic rate 20 percent to 30 percent, presumably because of the paucity of food substances in the cells. This condition resembles pellagra (because of the symptoms of diarrhea, dementia, and dermatitis) and may be misdiagnosed as a nutritional deficiency of niacin. Poor epithelial transport of neutral amino acids (such as tryptophan) leads to poor absorption of dietary amino acids, as well as excess amino acid excretion in the urine. Tryptophan is a precursor of niacin; it is an essential amino acid that must be included in the diet. Alkaptonuria, also called "black urine disease," is a genetic disorder of phenylalanine and tyrosine metabolism. Scurvy results from a deficiency of vitamin C, which is required for collagen synthesis. C) Mutations that produce a nonfunctional melanocortin-4 receptor cause extreme obesity and may account for as much as 5 percent to 6 percent of early onset, morbid obesity in children. All the other changes would tend to reduce food intake and/or increase energy expenditure and thus cause weight loss rather than obesity. A) One of the basic functions of vitamin A is in the formation of retinal pigments and therefore the prevention of night blindness. A) Cholecystokinin is released mainly in response to fats and proteins entering the duodenum and activates sensory receptors in the duodenum, sending messages to the brain stem via vagal afferents that contribute to satiation and meal cessation. Decreased utilization of these nutrients secondary to thiamine deficiency is responsible for many of the characteristics of beriberi, including peripheral vasodilation and edema, lesions of the central and peripheral nervous system, and gastrointestinal tract disturbances. D) Antagonists of melanocortin-4 receptors have been shown to markedly attenuate anorexia. All the others choices would tend to decrease appetite and/or increase energy expenditure, exacerbating the anorexia/cachexia of a patient with cancer. D) Triglycerides are hydrolyzed to glycerol and fatty acids, which, in turn, are oxidized to provide energy. Almost all cells, with the exception of some brain tissue, can use fatty acids almost interchangeably with glucose for energy. D) the rate of protein metabolism can be estimated by measuring the nitrogen in the urine, then adding 10 percent (about 90 percent of the nitrogen in proteins is excreted in the urine) and multiplying by 6. A) It is synthesized in the posterior pituitary gland B) It increases salt and water reabsorption in the collecting tubules and ducts C) It stimulates thirst D) It has opposite effects on urine and plasma osmolality 3. After menopause, hormone replacement therapy with estrogen-like compounds is effective in preventing the progression of osteoporosis. Of the following options, which outcome would be expected or which intervention would be suggested? Within minutes after a normal delivery, flow through the foramen ovale decreases dramatically. A young woman is given daily injections of a substance beginning on the sixteenth day of her normal menstrual cycle and continuing for 3 weeks. A) Conversion of cholesterol to 25-hydroxycholicalciferol B) Conversion of 25-hydroxycholicalciferol to 1,25dihydroxycholicalciferol C) Transport of calcium into the extracellular fluid D) Formation of calcium-binding protein E) Storage of vitamin D3 in the liver A Insulin D Muscle glucose uptake C Insulin the red lines in the above figure illustrate the normal relationships between plasma insulin concentration and glucose production in the liver and between plasma insulin concentration and glucose uptake in muscle. Which lines most likely illustrate these relationships in a patient with type 2 diabetes? Which lines most likely illustrate these relationships in a patient with acromegaly? Which of the following decreases the pressure in the pulmonary artery after birth? A) An increase in systemic arterial pressure B) Closure of ductus arteriosus C) An increase in left ventricular pressure D) A decrease in pulmonary vascular resistance 17. If a radioimmunoassay is properly conducted and the amount of radioactive hormone bound to antibody is low, what would this result indicate? A) Plasma levels of endogenous hormone are high B) Plasma levels of endogenous hormone are low C) More antibody is needed D) Less radioactive hormone is needed 19. When do progesterone levels rise to their highest point during the female hormonal cycle?
Cessation of breathing occurs for >20 seconds, at times accompanied by bradycardia and cyanosis. Generally, a problem of infancy, but may be seen later in childhood due to acquired brain injury. Idiopathic congenital central hypoventilation syndrome Unexplained by any of the listed possible causes. Seen with autonomic dysfunction-very low heart rate and respiratory rate variability, abrupt asystole, abnormal pupillary reactivity, temperature dysregulation, profuse sweating, swallowing difficulties, and/or oesophageal dysmotility. Late-onset central hypoventilation syndrome Presents following respiratory infection or anaesthesia, which may trigger the need for nocturnal ventilator support. Often preceded by chronic pulmonary hypertension, right heart failure, or respiratory infections with seizures or need for mechanical ventilation. Counsel parents Consider acetazolamide, non-invasive/long-term ventilation as appropriate. History and examination give diagnostic clues, but endoscopy is usually, and imaging may be required. Inspiratory stridor suggests a laryngeal obstruction, expiratory stridor implies tracheobronchial obstruction, and a biphasic stridor suggests a subglottic or glottic abnormality. Most neurological stridor is chronic; other causes include congenital or acquired stenosis or other compressive abnormalities, including webs, rings aberrant vessels, etc. Reduce numbers of unfamiliar bystanders to the minimum consistent with safety of personnel. Ensure any sensory impairments are minimized (find misplaced hearing aids, glasses, etc. Establish a rapport and attempt to reassure verbally and calm down: preferably consistently by the same member of staff. If medication is necessary, oral medication (haloperidol or risperidone) is preferable to parenteral administration. If parenteral administration is considered necessary, intramuscular administration is usually safer and more practicable than intravenous administration in an acute situation. Parenteral haloperidol can cause acute oculogyric crisis or dystonia (treat with procyclidine). Drug treatment Drug treatment of delirium should only be used when essential and then with care, especially in children. Antipsychotics and benzodiazepines can aggravate delirium, exacerbate underlying causes (for example, benzodiazepines worsening respiratory failure) and cause significant unwanted effects. In severe behavioural disturbance, haloperidol may be given intramuscularly or intravenously. Note resting pupil size and symmetry, and briskness and symmetry of the response to light. Do not mistake a dilated non-reactive pupil due an afferent pupillary defect (optic nerve involvement in fracture of the bony orbit) for a fixed dilated pupil due to third cranial nerve involvement in a herniation syndrome (the consensual response is present in the former, absent in the latter. The normal response is to maintain eye orientation in space (eyes move relative to the head and orbits). Intubation and ventilation of the unconscious child will be either for the purpose of securing a safe airway due to an inadequate cough and gag reflex, or for the management of raised intracranial pressure. Borderline cases should be discussed urgently with an intensivist or anaesthetist.
Syndromes
The probability of developing significant degenerative arterial disease is increased by certain vascular risk factors (Table 11. Age Family history of vascular disease Hypertension Diabetes mellitus Smoking Hypercholesterolaemia Alcohol Oral contraceptives Plasma fibrinogen M P A A M collateral blood supply. In the brain, this swelling may be sufficient to produce clinical deterioration in the days following a major stroke, as a result of a rise in intracranial pressure and compression of adjacent structures. The anterior (carotid) circulation consists of A + M, the posterior circulation is P plus the branches supplying the brainstem and cerebellum. Clinical features and classification Symptoms and signs of arterial infarcts depend on the vascular territory affected. Total anterior (carotid) circulation infarct hemiplegia (damage to the upper part of the corticospinal tract), hemianopia (damage to the optic radiation), cortical deficits. Multiple lacu82 Stroke Chapter 11 recurrent falls and fractures, spasticity, with pain, contractures and frozen shoulder, depression. Treatment the acute management of ischaemic stroke comprises: Admission to a stroke unit (Chapter 21), Aspirin 300 mg daily, modest benefit when given within 48 hours of onset, Thrombolysis. Up to 15% of patients will be eligible for thrombolysis with intravenous tissue plasminogen activator (alteplase). Patient assessment is urgent because this drug treatment must be started within 3 hours of stroke onset. Patients are ineligible for thrombolysis if there is uncertainty about the exact time of stroke onset and if they have risk factors for intracranial or systemic haemorrhage. For eligible patients, the benefits of preventing death or dependency outweigh the risk of alteplase causing symptomatic intracerebral haemorrhage. Some patients may benefit from newer techniques such as intra-arterial thrombolysis and clot retrieval, but these have not been the subjects of controlled clinical trials. Temporary removal of the skull vault on the side of the infarct (hemicraniectomy) may be life-saving. For the first 2 weeks after an ischaemic stroke, however, patients should not receive antihypertensive therapy beyond their pre-existing treatment unless there is evidence of malignant hypertension. This is because too rapid lowering of blood pressure may worsen ischaemia in a region where the cerebral circulation is already compromised (see below). Lifelong antiplatelet treatment is indicated, commencing as soon as possible after a cerebral infarct. The initial dose of aspirin (300 mg daily) can be reduced to 75 mg daily after 4 weeks. Anticoagulation with warfarin is effective prophylaxis in the presence of atrial fibrillation and other cardiac sources of embolism. If blood pressure falls below the autoregulatory range, as may occur in hypovolaemic shock, cerebral infarction may result as blood vessels are unable to dilate further in response to the drop in pressure, and blood flow falls. The regions most likely to be affected are the border zones or watersheds between vascular territories, as perfusion pressure here is usually at its lowest. Thus, for example, the patient may develop visual field defects or more complex visual disturbances. With severe (malignant) hypertension, the autoregulatory range may be exceeded and cerebral blood flow rises, with damage to vessel walls (fibrinoid necrosis) and consequent cerebral oedema. Rehabilitation Early management in stroke units is potentially life-saving (Chapter 21). Such an environment is best suited to the meticulous control of important variables which can affect outcome. Subsequent continued physiotherapy, occupational and speech therapy, and the involvement of social services may help survivors regain independence. In this process, intracerebral arteries alter their calibre in response to changes in cerebral perfusion pressure (the difference between blood pressure and intracranial pressure), a fall in pressure producing a widening of vessel lumen and hence constant flow. Treatment of intracranial venous sinus thrombosis is aimed at the underlying cause, in particular eradicating infection with appropriate antibiotics.
A different but equally promising approach to the design of cancer vaccines comes from observations made many years ago that tumor cells are immunogenic-animals injected with killed tumor cells do not grow tumors when challenged with live tissue. Genomics and proteomic methodologies provide novel tools for identifying tumor antigens. Additionally, there is a variety of approaches available to engage the immune system to respond to tumor antigens. Excise or tumor Use tumor cell line Isolate dendritic cells Mix killed tumor cells or proteins extracted from tumor cells with dendritic cells from patient Return dendritic cells and tumor antigens to patient Cancer vaccine design. Tumor cells are inactivated and mixed with dendritic cells from the patient and injected back into the patient as immunogens. An alternate approach is to prepare extracts or antigens from the tumor cells and inject these, in addition to dendritic cells, into the patient. Numerous observations indicate that activated macrophages also play a significant role in the immune response to tumors. For example, macrophages are often observed to cluster around tumors, and their presence is often correlated with tumor regression. The antitumor activity of activated macrophages is probably mediated by lytic enzymes and reactive oxygen and nitrogen intermediates. In spite of this, it is clear that an immune response can be generated to tumor cells, and therapeutic approaches aimed at increasing that response may serve as a defense against malignant cells. The immune surveillance theory was first conceptualized in the early 1900s by Paul Ehrlich. He suggested that cancer cells frequently arise in the body but are recognized as foreign and eliminated by the immune system. Some 50 years later, Lewis Thomas suggested that the cell-mediated branch of the immune system had evolved to patrol the body and eliminate cancer cells. According to these concepts, tumors arise only if cancer cells are able to escape immune surveillance, either by reducing their expression of tumor antigens or by an impairment in the immune response to these cells. Among the early observations that seemed to support the immune surveillance theory was the increased incidence of cancer in transplantation patients on immunosuppressive drugs. According to the immune surveillance theory, these mice should show an increase in cancer, instead, nude mice are no more susceptible to cancer than other mice. Furthermore, although individuals on immunosuppressive drugs do show an increased incidence of cancers of the immune system, other common cancers. One possible explanation for the selective increase in immunesystem cancers is that the immunosuppressive agents themselves may exert a direct carcinogenic effect on immune cells. Experimental data concerning the effect of tumor-cell dosage on the ability of the immune system to respond also are incompatible with the immune surveillance theory. For example, animals injected with very low or very high doses of tumor cells develop tumors, whereas those injected with intermediate doses do not. The mechanism by which a low dose of tumor cells "sneaks through" is difficult to reconcile with the immune surveillance theory. Finally, this theory assumes that cancer cells and normal cells exhibit qualitative antigen differences. In fact, as stated earlier, many types of tumors do not express tumor-specific antigens, and any immune response that develops must be induced by quantitative differences in antigen expression by normal cells and tumor cells. However, tumors induced by viruses would be expected to express some antigens encoded by the viral genome. These antigens are qualitatively different from those expressed by normal tissues and would be expected to attract the attention of the immune system. In fact, there are many examples of specific immune responses to virally induced tumors. Nevertheless, apart from tumors caused by viruses, the basic concept of the immune surveillance theory-that malignant tumors arise only if the immune system is somehow impaired or if the tumor cells lose their immunogenicity, enabling them to escape immune surveillance-at this time Tumor Evasion of the Immune System Although the immune system clearly can respond to tumor cells, the fact that so many individuals die each year from cancer suggests that the immune response to tumor cells is often ineffective. This section describes several mechanisms by which tumor cells appear to evade the immune system.

Effective immunity against a number of diseases, including cholera and gonorrhea, depends on increased production of secretory IgA at mucous membrane surfaces. Similar strategies using bacteria that are a normal part of oral flora are in development. The strategy would involve introduction of genes encoding antigens from pathogenic organisms into bacterial strains that inhabit the oral cavity or respiratory tract. Eliciting immunity at the mucosal surface could provide excellent protection at the portal used by the pathogen. For example, the encoded protein is expressed in the host in its natural form-there is no denaturation or modification. The immune response is therefore directed to the antigen exactly as it is expressed by the pathogen. Unlike vaccinia, the canarypox virus does not appear to be virulent even in individuals with severe immune suppression. This pathway stimulates B-cell immunity and generates antibodies and B-cell memory against the protein. However, they are not a universal solution to the problems of vaccination; for example, only protein antigens can be encoded-certain vaccines, such as those for pneumococcal and meningococcal infections, use protective polysaccharide antigens. Multivalent Subunit Vaccines One of the limitations of synthetic peptide vaccines and recombinant protein vaccines is that they tend to be poorly immunogenic; in addition, they tend to induce a humoral antibody response but are less likely to induce a cell-mediated response. What is needed is a method for constructing synthetic peptide vaccines that contain both immunodominant B-cell and T-cell epitopes. A number of innovative techniques are being applied to develop multivalent vaccines that can present multiple copies of a given peptide or a mixture of peptides to the immune system (Figure 18-7). In micelles and liposomes, the hydrophilic residues of the antigen molecules are oriented outward. By attaching different monoclonal antibodies to the solid matrix, it is possible to bind a mixture of peptides or proteins, composing immunodominant epitopes for both T cells and B cells, to the solid matrix (see Figure 18-7a). These multivalent complexes have been shown to induce vigorous humoral and cell-mediated responses. Their particulate nature contributes to their increased immunogenicity by facilitating phagocytosis by phagocytic cells. Another means of producing a multivalent vaccine is to use detergent to incorporate protein antigens into protein micelles, lipid vesicles (called liposomes), or immunostimulating complexes (see Figure 18-7b). The individual proteins orient themselves with their hydrophilic residues toward the aqueous environment and the hydrophobic residues at the center so as to exclude their interaction with the aqueous environment. Liposomes containing protein antigens are prepared by mixing the proteins with a suspension of phospholipids under conditions that form vesicles bounded by a bilayer. The proteins are incorporated into the bilayer with the hydrophilic residues exposed. Realizing the optimum benefit of vaccines will require cheaper manufacture and improved delivery methods for existing vaccines. Acellular pertussis vaccines containing genetically detoxified pertussis toxin induce long-lasting humoral and cellular responses in adults. Sucessful control of epidemic diphtheria in the states of the former Union of Soviet Socialist Republics: lessons learned. Poliovirus vaccines: progress toward global poliomyelitis eradication and changing routine immunization recommendations in the United States. Protein components of pathogens expressed in cell culture may be effective vaccines. Recombinant vectors, including viruses or bacteria, engineered to carry genes from infectious microorganisms, maximize cell-mediated immunity to the encoded antigens. If the girl receives no further treatment and steps on a rusty nail again 3 years later, will she be immune to tetanus? What are the advantages of the Sabin polio vaccine compared with the Salk vaccine? In an attempt to develop a synthetic peptide vaccine, you have analyzed the amino acid sequence of a protein antigen for (a) hydrophobic peptides and (b) strongly hydrophilic peptides. How might peptides of each type be used as a vaccine to induce different immune responses? You have identified a bacterial protein antigen that confers protective immunity to a pathogenic bacterium and have cloned the gene that encodes it. Explain the relationship between the incubation period of a pathogen and the approach needed to achieve effective active immunization.
Remarkably, these patients, although unable to identify others by their facial features, may be able to identify them by other features, such as their voice, dress, or characteristic gait (Damasio et al. Finally, and most remarkably, some patients are not able to recognize themselves when they look in the mirror (Damasio et al. As might be expected, such patients, in addition to being unable to recognize old acquaintances by their facial features, are also unable to utilize facial features to recognize new acquaintances (Malone et al. Topographagnosia At the outset, it should be noted that there is some debate regarding the definition of topographagnosia and, consequently, the reader, in perusing journal articles, should pay particular attention to the definition peculiar to the authors of the article. In this text, topographagnosia refers to a condition in which patients, despite adequate memory and vision, are unable to find their way in surroundings that had not previously caused any difficulty. In landmark agnosia, difficulty arises at the level of recognizing the Bank as a landmark. Although the patient may recognize the building, and even describe it, it is not recognized as a landmark and hence the patient is as likely to walk past it as to turn. In one case, a patient `had sudden difficulty finding her way out of a subway station she had used daily for years. The buildings in front of him were familiar to him, so he could recognize them right away. The basis for this, however, lies in an inability to commit to memory features of the new environment, and this stands in contrast with topographagnosia wherein memory is intact. Furthermore, patients with amnesia typically have no trouble finding their way in environments that they have travelled in before, provided, of course, that any retrograde amnesia has not obscured their recall. Patients with dementia or delirium often lose their way and although this may be on the basis of memory loss (or, in the case of delirium, confusion), it can also occur in patients with relatively preserved memory, and in these cases it is perhaps appropriate to consider the topographagnosia as but one indicator of widespread cortical damage or dysfunction. The existence of other cognitive deficits, however, indicates the correct syndromal diagnosis. An example was also reported as a sequela to herpes simplex encephalitis wherein there was damage to both temporal lobes, with the right side being much more severely involved (McCarthy et al. Topographical disorientation has also been reported with infarction of the bilateral fusiform, lingual, and parahippocampal gyri (Alsaadi et al. Interestingly, cases have also been reported secondary to infarction of the splenium (Alsaadi et al. Further, there are also case reports of topographagnosia occurring on a transient basis, with episodes lasting from 5 to 30 minutes (Stracciari et al. During these episodes, apart from the topographagnosia, patients are otherwise normal and recovery is complete. Most patients were women in their middle or later years and, although the etiology is unknown, it is speculated to be similar to that of transient global amnesia. In color agnosia, patients, despite normal color vision, are unable to recognize and name the color of objects (Kinsbourne and Warrington 1964; Meadows 1974a). Whereas patients with achromatopsia are unable to read the plates, patients with color agnosia are. The patient with achromatopsia exists in a world of grays; by contrast, the patient with color agnosia, although able to discern hues, cannot name them. Although hemiparesis is the deficit most commonly involved (and indeed anosognosia for hemiparesis is very common in the first few months after stroke [Hier 1983a,b]), other deficits, as noted below, may also go unrecognized. Even more remarkably, in some cases the patient may insist that the paralyzed limb, although motionless, is in fact moving (Feinberg et al. Other deficits that may go unrecognized include hemianopia, cortical blindness, chorea, and cognitive or behavioral deficits. Anosognosia for hemianopia after stroke was noted in over one-half of patients in one study (Celesia et al. Patients, although blind, may insist that their vision is perhaps only slightly impaired, that the light is too dim, or they may flatly insist that there is nothing wrong with their vision at all; attempting to walk, they predictably bump into things, trip, and fall. Cognitive and behavioral deficits may also be denied by patients with dementia, who may insist on keeping their own checkbooks or driving with disastrous results.
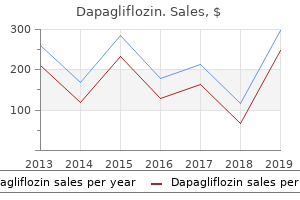
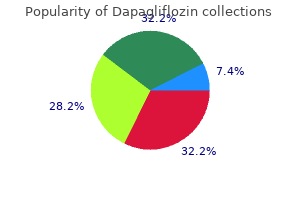
Hilberry (Wintergreen). Dapagliflozin.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96762

Laboratory abnormalities of specific immune function vary depending on the specific gene defect and can include alterations in immunoglobulin levels with impaired specific antibody responses, as well as defects of specific cellular immunity, as determined by using in vivo and in vitro assays. Therapy is often supportive and anti-infective with drugs and polyclonal human IgG. The principal clinical manifestations of humoral immunodeficiency are recurrent bacterial infections of the upper and lower respiratory tract. Both X-linked and autosomal forms of agammaglobulinemia are associated with extremely low numbers (absence) of B cells. The X-linked form (Bruton agammaglobulinemia) accounts for the majority (85%) of cases. In patients with common variable immunodeficiency, laboratory evaluation generally shows variable reduction in 2 or more major immunoglobulin classes, impairment of specific antibody responses, and, occasionally, reductions in B-cell numbers. For agammaglobulinemia or common variable immunodeficiency, therapy is either with antibiotic prophylaxis, IgG replacement, or both (Tables E6 and E7). The disorders of immune dysregulation (Fig E3) include the hemophagocytic syndromes, syndromes with autoimmunity and hypersensitivity, and lymphoproliferation. The hemophagocytic syndromes often have fulminant acute presentations triggered by viral infections. Other prominent disorders in this category are the autoimmune lymphoproliferative syndromes and immune deficiency, polyendocrinopathy, X-linked syndrome. Phagocytic cell defects (Fig E4) can present with severe pyogenic bacterial and fungal infections of the respiratory tract, skin, and viscera and gingivostomatitis. Laboratory evaluation might show neutropenia, normal neutrophil numbers, or marked neutrophilia (mainly in cellular adhesion defects). Functional studies show most often a defect in oxidative metabolism because chronic granulomatous disease is the most common phagocyte defect. In patients with other disorders, there might be simply severe neutropenia or variable impairment of chemotaxis (leukocyte adhesion defects), phagocytosis, or intracellular killing. The care of patients with other forms of phagocyte defects is primarily anti-infective and supportive. Also included in the category of phagocytic cell defects are the syndromes classified under Mendelian susceptibility to mycobacterial disease. These patients exhibit somewhat restricted susceptibility to mycobacteria and to severe salmonella infections. Disorders of innate immunity are rare and include defects of Toll-like receptor signaling, such as nuclear factor kB essential modulator syndrome, often exhibiting ectodermal dysplasia along with infection susceptibility with a narrow (eg, predominantly pyogenic bacteria or fungi) to a wide range of pathogens (Fig E5). These diseases are characterized by episodic fever often in association with other inflammatory manifestations that can affect the skin, joints, and gastrointestinal tract. Most early classical and alternative pathway complement defects tend to present either with systemic autoimmune disease resembling lupus erythematosus or recurrent respiratory tract bacterial infections similar to antibody deficiency. Deficiencies of terminal components can also be associated with recurrent neisserial meningitis. Some patients with low serum levels of mannosebinding lectin might be predisposed to bacterial respiratory tract infections, but there could be other host factors that interact to create such susceptibility in a patient. It is recommended that diagnosis and therapy are guided overall or performed in consultation with persons and centers with knowledge and experience diagnosing and treating a broad range of immunodeficiencies to improve consistency in evaluation and management and to have the best outcomes with respect to patient and family health, education, and planning. Primary immunodeficiency diseases: an update on the classification from the international union of immunological societies expert committee for primary immunodeficiency. Population prevalence of diagnosed primary immunodeficiency diseases in the United States. Newborn screening for severe combined immunodeficiency in 11 screening programs in the United States. Laboratory screening for the diagnosis of children with primary immunodeficiencies. Laboratory diagnosis of specific antibody deficiency to pneumococcal capsular polysaccharide antigens. Assessment of the antibody response to pneumococcal vaccine in high-risk populations. Estimating the protective concentration of anti-pneumococcal capsular polysaccharide antibodies.

An upright, well-supported posture is paramount during feeding, and an occupational therapist may help with this. The decision to insert a gastrostomy should be interdisciplinary, and made with the parents. Oral intake can still continue for pleasure, but there is no pressure to get calories in. Medical treatment includes reduction of acid production (ranitidine, omeprazole), prokinetics (domperidone, erythromycin, metoclopramide) and thickening agents (gaviscon, carobel). If gastrostomy is contemplated, and reflux is severe, the procedure can be combined with (laparoscopic) fundoplication. This is mainly due to poor bulbar function and is aggravated by problems with head control, lip closure, tongue control, dental malocclusion, chewing, sucking, swallowing, intraoral sensitivity and dysarthria. Other options include a palatal plate, botulinum toxin injections in the parotid glands, and surgical transplantation of salivary ducts posteriorly. The abdominal wall and stomach are perforated, and a gastrostomy is pulled through the resulting hole from the inside out. Benefits include increased weight, length, and skin-fold thickness, less time spent feeding, improved health (reduced admissions for chest infections), and improvement in quality of life, improvement in social functioning, mental health, energy, vitality and general health perception. Receptive communication (understanding) therefore requires adequate hearing (for verbal communication) or vision (for gestural or symbolic communication), and the cognitive ability to interpret this information. Expressive communication ultimately requires the ability to perform at least some movements voluntarily, with reasonable consistency. Speech production is, of course, a particular form of complex movement, but in some situations where speech is not possible, another voluntary movement can be recruited for purposes of communication. Total communication Speech and language therapy; peripatetic specialist teacher of the deaf, partially hearing unit in mainstream schooling or specialist school. Vision Some processes that cause general neurological disease will also cause primary ocular (particularly retinal) disease or refractive errors. Appropriate multidisciplinary assessment of these issues is likely to include specialist paediatric ophthalmology and neuropsychology or occupational therapy input. Consideration of which may be at work in an individual child is important in identifying potential interventions, realistic assessments of long-term respiratory prognosis and in informing the always difficult decisions about appropriateness of intensive care. Disturbed control of respiratory rate/rhythm Central hypoventilation Signs may be minimal when awake. Other indicators may include temperature instability, or disturbance of the hypothalamopituitary axis. This can increase tendency to infection through ineffective clearance of secretions and atelectasis. Acute disseminated encephalomyelitis cohort study: prognostic factors for relapse. They include presence of lesions perpendicular to the corpus callosum or presence of well-defined lesions.

These patients presented very early in life with recurrent fever and systemic inflammation, as well as hepatosplenomegaly and lymphadenopathy, without other signs of mucosal inflammation. In addition, they were affected by recurrent infection, although not until steroid therapy was initiated for the autoinflammatory episodes. Prophylactic antibiotics, hyperimmunization, and immunoglobulin replacement have been used to attempt to reduce infection rates. Vaccination against N meningitidis, H influenzae, and S pneumoniae should be performed, with serologic confirmation of response. If poor response to vaccination is noted, immunoglobulin replacement should be strongly considered. Of note, for 7 patients older than 14 years who were not receiving prophylaxis, no further invasive infections were described. Thus reducing or discontinuing prophylaxis might be considered in well patients during this age period. Signs of inflammation might be lacking in early infection, particularly in neonates. Nearly all neonates and roughly half of infants and children will lack fever (>388C) in the setting of invasive bacterial infections. Antibiotic treatment should not be withheld based on lack of inflammatory features. Because the majority of patients seem to have an initial encephalopathic period followed by neurological deterioration during a limited period of a few months with subsequent stabilization, early diagnosis and symptom control might be critical to minimizing clinical decline during this critical progressive stage. There is also significant variability in the disease between patients and even within families. Therapy of type 1 interferonopathies should be directed toward infectious and autoimmune complications. Condyloma accuminata can occur, as can dysplastic lesions with risk of malignant transformation. Recurrent pneumonias are common, which in some cases might contribute to the development of bronchiectasis. Other infections include sinusitis, cellulitis, urinary tract infection, thrombophlebitis, osteomyelitis, and deep tissue abscesses. Common pathogens include H influenzae, S pneumoniae, Klebsiella pneumoniae, S aureus, and Proteus mirabilis. Aside from human papillomaviruses, other viruses are rarely implicated in patients with severe infections. Levels of IgG, IgA, or both are often less than normal levels; IgM levels are more often normal. Humoral responses to vaccination are present but often transient, with rapid waning of protection over time. Skin lesions present as disseminated macules or flat warts that are concentrated in areas of sun exposure and often change slowly over time. Immunologic studies in these siblings showed decreased T-cell proliferation in vitro, as well as markedly decreased numbers of naive T cells. Monitoring for premalignant lesions through regular dermatologic screening is recommended. There are insufficient data to determine the safety of these vaccines for these patients. Patients presenting with a family history of asplenia or sepsis caused by encapsulated bacteria, most frequently S pneumoniae, should be evaluated for congenital asplenia. It is often a silent disease until presentation with sudden invasive disease, most frequently as pneumococcal sepsis. This contrasts with asplenia syndrome (Ivemark syndrome), which presents primarily with symptomatic congenital heart disease in early infancy. Diagnosis is made by means of ultrasound of the abdomen and examination for Howell-Jolly bodies on peripheral blood smear. Prophylaxis should be continued at least until the age of 5 years in fully vaccinated children.
Langerhans cells (dendritic cells found throughout the epithelial layers of the skin and the respiratory, gastrointestinal, urinary, and genital tracts) can capture antigens from invading pathogens and migrate into a nearby lymphatic vessel, where the flow of lymph carries them to nearby lymph nodes. Once in the lymph, the newly released activated lymphocytes can enter the bloodstream via the subclavian vein. Eventually, the circulation carries them to blood vessels near the site of the infection, where the inflammatory process makes the vascular endothelium of the nearby blood vessels more adherent for activated T cells and other leukocytes (see Chapter 15). Chemotactic factors that attract lymphocytes, macrophages, and neutrophils are also generated during the inflammatory process, promoting leukocyte adherence to nearby vascular epithelium and leading leukocytes to the site of the infection. Later in the course of the response, pathogen-specific antibodies produced in the node are also carried to the bloodstream. Inflammation aids the delivery of the anti-pathogen antibody by promoting increased vascular permeability, which increases the flow of antibody-containing plasma from the blood circulation to inflamed tissue. The result of this network of interactions among diffusible molecules, cells, organs, the lymphatic system, and the circulatory system is an effective and focused immune response to an infection. Consequently, adaptive immunity, which is mediated by antibodies and T cells, is only seen in this phylum. However, as shown in Figure 2-23, the kinds of lymphoid tissues seen in different orders of vertebrates differ. The presence and location of lymphoid tissues in several major orders of vertebrates are shown. Whether bone marrow is involved in the generation of lymphocytes in reptiles is under investigation. The differences seen at the level of organs and tissues are also reflected at the cellular level. Lymphocytes that express antigen-specific receptors on their surfaces are necessary to mount an adaptive immune response. So far, it has not been possible to demonstrate the presence of T or B lymphocytes in the jawless fishes, and attempts to demonstrate an adaptive immune response in lampreys and hagfish, members of the order Agnatha, have failed. In fact, only jawed vertebrates (Gnathosomata), of which the cartilaginous fish (sharks, rays) are the earliest example, have B and T lymphocytes and support adaptive immune responses. The lymphocyte is the only cell to possess the immunologic attributes of specificity, diversity, memory, and self/nonself recognition. The division of a stem cell can result in the production of another stem cell and a differentiated cell of a specific type or group. All leukocytes develop from a common multipotent hematopoietic stem cell during hematopoiesis. Various hematopoietic growth factors (cytokines) induce proliferation and differentiation of the different blood cells. The differentiation of stem cells into different cell types requires the expression of different lineage-determining genes. Hematopoiesis is closely regulated to assure steady-state levels of each of the different types of blood cell. Cell division and differentiation of each of the lineages is balanced by programmed cell death. The three types of lymphoid cells are best distinguished on the basis of function and the presence of various membrane molecules. Naive B and T lymphocytes (those that have not encountered antigen) are small resting cells in the G0 phase of the cell cycle. After interacting with antigen, these cells enlarge into lymphoblasts that proliferate and eventually differentiate into effector cells and memory cells. Macrophages and neutrophils are specialized for the phagocytosis and degradation of antigens (see Figure 2-9). I I I I I I Phagocytosis is facilitated by opsonins such as antibody, which increase the attachment of antigen to the membrane of the phagocyte. Activated macrophages secrete various factors that regulate the development of the adaptive immune response and mediate inflammation (see Table 2-7). Basophils and mast cells are nonphagocytic cells that release a variety of pharmacologically active substances and play important roles in allergic reactions. Follicular dendritic cells, unlike the others, facilitate B-cell activation but play no role in T-cell activation.
References:




