The photomicrograph below shows an esophageal biopsy taken 10 cm above the lower esophageal sphincter. A 71-year-old male presents with dysphagia and is found to have a 5-cm mass that is located in the middle third of the esophagus and extends into adjacent lung tissue. A mass composed of benign cartilage A mass composed of benign smooth-muscle cells Infiltrating groups of cells forming glandular structures Infiltrating sheets of cells forming keratin Infiltrating single cells having intracellular mucin 275. A 2-week-old neonate presents with regurgitation and persistent, severe projectile vomiting. Oral medication with omeprazole and clarithromycin Oral medication with vancomycin or metronidazole Surgery to cut a hypertrophied stenotic band at the pylorus Surgery to remove a mass of the adrenal gland Surgery to resect an aganglionic section of the intestines 276. A 49-year-old female taking ibuprofen for increasing joint pain in her hands presents with increasing pain in her midsternal area. Gastroscopy reveals multiple, scattered, punctate hemorrhagic areas in her gastric mucosa. Biopsies from one of these hemorrhagic lesions reveal mucosal erosions with edema and hemorrhage. Active chronic gastritis Acute gastritis Autoimmune gastritis Chronic gastritis Peptic ulcer disease 304 Pathology 277. A biopsy of the antrum of the stomach of an adult who presents with epigastric pain reveals numerous lymphocytes and plasma cells within the lamina propria, which is of normal thickness. A Steiner silver stain from this specimen is positive for a small, curved organism, which is consistent with a. A 51-year-old male presents with epigastric pain that is lessened whenever he eats. A gastroscopy is performed to evaluate these gastric symptoms and a solitary gastric ulcer is seen. The margins of the ulcer are slightly elevated, and gastric rugae radiate outward from the ulcer. Based on these findings, in order to relieve the epigastric pain this patient should a. Take indomethacin twice a day Abstain from smoking Eat only two meals per day Drink alcohol with his evening meal Have surgery to resect the ulcer Gastrointestinal System 305 279. Gastric tumors with the histologic appearance illustrated in the photomicrograph below are likely to have a gross appearance described best by which one of the listed terms The overall incidence of malignancies of the stomach in the United States is decreasing primarily due to a decreased incidence of a. Is present in approximately 20% of normal persons Is lined by heterotopic gastric mucosa in less than 2% of cases Often shows mucosal ulceration Is related to persistence of the vitellointestinal duct Usually arises from the mesenteric border of the ileum 282. The signs and symptoms in which one of the listed individuals are most likely to be due to intussusception of the bowel An 18-year-old male with fever, leukocytosis, and right lower quadrant abdominal pain b. A 3-year-old child with the abrupt onset of colicky abdominal pain and bloody, "currant jelly" stools c. A 67-year-old female with fever, leukocytosis, and left lower quadrant abdominal pain. A newborn infant with projectile vomiting and midepigastric mass Gastrointestinal System 307 283. A 10-month-old, previously healthy male infant develops a severe, watery diarrhea 2 days after visiting the pediatrician for a routine checkup. The appearance of the small intestinal mucosa illustrated in the photomicrograph below indicates a. He is found to have multiple pain and swelling of his joints (migratory polyarthritis) and generalized lymphadenopathy. Fibrosis may produce a "lead pipe" appearance with "creeping fat" around the outside of the gut b. Sudden abdominal pain may result from intestinal obstruction due to pericolonic abscess. A biopsy from the terminal ileum reveals numerous acute and chronic inflammatory cells within the lamina propria. Gross examination of this resected bowel reveals deep, long mucosal fissures extending deep into the muscle wall.
It modulates intracellular levels of Ca2+ through the activation of protein kinases; these enzymes phosphorylate various transport proteins in the sarcolemma and sarcoplasmic reticulum and also in the troponin-tropomyosin regulatory complex, affecting intracellular levels of Ca2+ or responses to it. There is a rough correlation between the phosphorylation of TpI and the increased contraction of cardiac muscle induced by catecholamines. This may account for the inotropic effects (increased contractility) of -adrenergic compounds on the heart. We shall briefly consider three transmembrane proteins that play roles in this process. Ca2+ Channels Ca2+ enters myocytes via these channels, which allow entry only of Ca2+ ions. The major portal of entry is the L-type (long-duration current, large conductance) or slow Ca2+ channel, which is voltage-gated, opening during depolarization induced by spread of the cardiac action potential and closing when the action potential declines. Fast (or T, transient) Ca2+ channels are also present in the plasmalemma, though in much lower numbers; they probably contribute to the early phase of increase of myoplasmic Ca2+. It is estimated that approximately 10% of the Ca2+ involved in contraction enters the cytosol from the extracellular fluid and 90% from the sarcoplasmic reticulum. However, the former 10% is important, as the rate of increase of Ca2+ in the myoplasm is important, and entry via the Ca2+ channels contributes appreciably to this. In resting myocytes, it helps to maintain a low level of free intracellular Ca2+ by exchanging one Ca2+ for three Na+. The energy for the uphill movement of Ca2+ out of the cell comes from the downhill movement of Na+ into the cell from the plasma. This exchange contributes to relaxation, but may run in the reverse direction during excitation. Because of the Ca2+-Na+ exchanger, anything that causes intracellular Na+ (Na+i) to rise will secondarily cause Ca2+i to rise, causing more forceful contraction. This results in less Na+ being pumped out of the cardiac myocyte and leads to an increase of the intracellular concentration of Na+. In turn, this stimulates the Na+-Ca 2+ exchanger so that more Na+ is exchanged outward, and more Ca2+ enters the myocyte. The resulting increased intracellular concentration of Ca2+ increases the force of muscular contraction. Cardiac muscle is rich in ion channels, and they are also important in skeletal muscle. Mutations in genes encoding ion channels have been shown to be responsible for a number of relatively rare conditions affecting muscle. It should be noted that there are a variety of ion channels (Chapter 40) in most cells, for Na+, K+, Ca2+, etc. Open or close in response to a specific intracellular molecule, eg, a cyclic nucleotide. Open in response to a change in membrane potential, eg, Na+, K+, and Ca2+ channels in heart. Some conditions are mild, whereas others are severe and may be part of a syndrome affecting other tissues. Mutations in the genes encoding these latter proteins cause familial hypertrophic cardiomyopathy, which will now be discussed. Mutations in the Cardiac -Myosin Heavy Chain Gene Are One Cause of Familial Hypertrophic Cardiomyopathy Familial hypertrophic cardiomyopathy is one of the most frequent hereditary cardiac diseases. Patients exhibit hypertrophy-often massive-of one or both ventricles, starting early in life, and not related to any extrinsic cause such as hypertension.
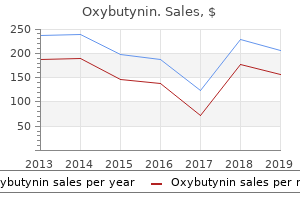
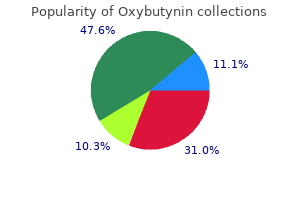
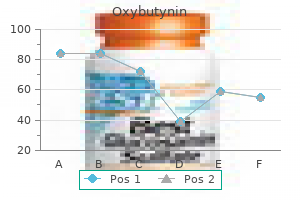
| Comparative prices of Oxybutynin | ||
| # | Retailer | Average price |
| 1 | Menard | 581 |
| 2 | ShopKo Stores | 670 |
| 3 | GameStop | 573 |
| 4 | Darden Restaurants | 121 |
| 5 | Costco | 918 |
| 6 | Office Depot | 162 |
| 7 | Ingles Markets | 630 |
| 8 | Rite Aid | 276 |
| 9 | Giant Eagle | 169 |
A given amino acid can be coded for by more than one codon (degenerate code), but a given codon codes for just one particular amino acid (unambiguous code). Phosphorylation at carbon 6 of terminal mannose residues in glycoproteins targets these proteins (acid hydrolases) to lysosomes. Each of these steps can be regulated to provide additional control over the kinds and amounts of functional products that are produced. For example, genes described as constitutive encode products required for basic cellular functions, and so are continually expressed; they are also known as "housekeeping" genes. The ability to regulate gene expression, that is, to determine if, how much, and when particular gene products will be made, gives the cell control over structure and function. A trans-acting Proteins Modified or degraded proteins In eukaryotes gene expression also involves posttranscriptional and posttranslational processes Figure 32. For example, a protein transcription factor (a trans-acting molecule) which regulates a gene on chromosome 6 might itself have been transcribed from a gene on chromosome 11. However, when an inducer molecule is present, it binds to the repressor, causing the repressor to change shape so that it no longer binds the operator. The lactose (lac) operon contains the genes that code for three proteins involved in the catabolism of the disaccharide, lactose: the lacZ gene codes for -galactosidase, which hydrolyzes lactose to galactose and glucose; the lacY gene, which codes for a permease that facilitates the movement of lactose into the cell; and the lacA gene that codes for thiogalactoside transacetylase whose exact physiologic function is unknown. Allolactose binds to repressor protein, causing a conformation change that prevents its binding to the operator. Operator l Z lacZ gene l Y gene lacY l A gene lacA Promoter Even though the operon is off, the synthesis of a few molecules of permease results in the uptake and conversion of a small amount of lactose to allolactose, and the inactivation of some repressor molecules. The synthesis of a few molecules of permease (and -galactosidase) allows the organism to respond rapidly should glucose become unavailable. Regulation of Gene Expression when lactose is available to the cell but glucose is not. A regulatory gene, the lacI gene, codes for the repressor protein (a trans-acting factor) that binds to the operator site. When glucose is the only sugar available: In this case, the lac Amino acid sequence forms a turn -Helix operon is repressed (turned off). Repression is mediated by the repressor protein binding via a helix-turn-helix motif (Figure 32. When both glucose and lactose are available: In this case, tran- scription of the lac operon is negligible, even if lactose is present at a high concentration. The tryptophan operon the tryptophan (trp) operon codes for five proteins that are required for the synthesis of the amino acid, tryptophan. Negative control includes trp itself binding to the repressor protein and facilitating the binding of the repressor to the operator. Repression by trp is not always complete, however, and so unlike the lac operon, the trp operon is also regulated by a process known as attenuation. With attenuation, transcription is initiated but is terminated well before completion (Figure 32. In eukaryotes this does not occur because, as a result of having a membrane-bound nucleus, transcription and translation are spatially and temporally separate processes. Thus, transcriptional control by the stringent response ultimately results in down-regulation of protein synthesis until amino acids are again available. The higher degree of complexity of eukaryotic genomes, as well as the presence of a nuclear membrane, necessitates a wider range of regulatory processes. As with the prokaryotes, the primary site of regulation is at the level of transcription. Again, the theme of trans-acting molecules binding to cis-acting elements is seen. Operons, however, are not found in eukaryotes, which must use alternative strategies to solve the problem of how to coordinately regulate all the genes required for a specific response. In eukaryotes, gene expression is also regulated at multiple levels other than transcription. Cis-acting regulatory elements the need to coordinately regulate a group of genes to effect a particular response is of key importance in multicellular organisms including humans. An underlying theme occurs repeatedly: A protein binds to a regulatory element for each of the genes in the group and coordinately affects the expression of those genes, even if they are on different chromosomes. In general, hormones bind either to intracellular receptors (steroid hormones are an example, see p.
It has been estimated that some 1% of the human genome may be involved with glycosylation events. Multiple species of the other glycosyltransferases (eg, sialyltransferases) also exist. Controlling factors of the first stage of N-linked glycoprotein biosynthesis (ie, oligosaccharide assembly and transfer) include (1) the presence of suitable acceptor sites in proteins, (2) the tissue level of Dol-P, and (3) the activity of the oligosaccharide: protein transferase. Certain glycosyltransferases act only on an oligosaccharide chain if it has already been acted upon by another processing enzyme. Differences in conformation of different proteins may facilitate or hinder access of processing enzymes to identical oligosaccharide chains. Same cells (eg, fibroblasts) from different species may exhibit different patterns of processing enzymes. Cancer cells may exhibit processing enzymes different from those of corresponding normal cells. In turn, the oligosaccharide chain is linked via phosphorylethanolamine in an amide linkage to the carboxyl terminal amino acid of the attached protein. The genes encoding many glycosyltransferases have already been cloned, and others are under study. The latter should also cast light on the mechanisms involved in their transcriptional control, and gene knockout studies are being used to evaluate the biologic importance of various glycosyltransferases. Tunicamycin Inhibits N- But Not O-Glycosylation A number of compounds are known to inhibit various reactions involved in glycoprotein processing. These agents can be used experimentally to inhibit various stages of glycoprotein biosynthesis and to study the effects of specific alterations upon the process. For instance, if cells are grown in the presence of tunicamycin, no glycosylation of their normally N-linked glycoproteins will occur. In certain cases, lack of glycosylation has been shown to increase the susceptibility of these proteins to proteolysis. The functional significance of these variations among structures is not understood. Increased mobility may be important in facilitating rapid responses to appropriate stimuli. Glycation is distinguished from glycosylation because the latter involves enzyme-catalyzed attachment of sugars. When glucose attaches to a protein, in- termediate products formed include Schiff bases. These reactions are involved in the browning of certain foodstuffs that occurs on storage or processing (eg, heating). At constant time intervals, the extent of glycation is more or less proportional to the blood glucose level. Non-enzymic attachment of glucose to hemoglobin A present in red blood cells (ie, formation of HbA1c) occurs in normal individuals and is increased in patients with diabetes mellitus whose blood sugar levels are elevated. As discussed in Chapter 6, measurement of HbA1c has become a very important part of the management of patients with diabetes mellitus. Glucose is shown interacting with the amino group of hemoglobin (Hb) forming a Schiff base. Thickening of basement membranes can also occur by binding of glycated proteinstothem. Damage to renal basement membranes, thickening of these membranes in capillaries and endothelial dysfunction are found in ongoing uncontrolled diabetes mellitus. Here, their involvement in two specific processes-fertilization and inflammation-will be briefly described. In addition, the bases of a number of diseases that are due to abnormalities in the synthesis and degradation of glycoproteins will be summarized. Selectins Play Key Roles in Inflammation & in Lymphocyte Homing Leukocytes play important roles in many inflammatory and immunologic phenomena.

Foodborne transmission, particularly involving unpasteurized apple cider, raw milk, and ill food handlers, has been documented. International travelers who drink the water in countries with less stringent drinking water treatment standards than the United States may might be at risk for Cryptosporidium infection. Across all time periods, the highest rates were in children from birth to age 14 years, and cases were most frequently reported in children aged 1 to 4 years. Infected patients can be asymptomatic, those with symptoms might not seek health care, health care providers might not request laboratory diagnostics when evaluating non-bloody diarrhea, requested ova and parasite testing might not include Cryptosporidium testing, and positive laboratory results are not always reported to public health officials. Diarrheawhich can be profuse, usually non-bloody, and watery-and weight loss, abdominal pain, anorexia, fatigue, joint pain, headache, fever, and vomiting have been reported in immunocompetent children and adults with Cryptosporidium infection. Cryptosporidium infection in children can have a significant impact on nutritional status and growth. Diagnostic studies show dilatation of the common bile duct, thickening of the gall bladder wall, and pericholecystic fluid collection. When compared with microscopy, the sensitivity for detection of parasitic pathogens was 91. Molecular characterization tools are being increasingly used to differentiate Cryptosporidium species in outbreak investigations and infection/contamination source tracking. Maternal infection with Cryptosporidium has been associated with infection in young infants demonstrating the importance of caregiver hygiene. Some outbreaks of cryptosporidiosis have been linked to ingestion of water from contaminated municipal water supplies; the incidence of these outbreaks has dramatically decreased since the mid-1990s because of improved water treatment targeting the inactivation and removal of Cryptosporidium. To decrease the risk of cryptosporidiosis during outbreaks or when otherwise advised by local public health officials to boil water, heat water used for preparing infant formula, drinking, making ice, etc. After the boiled water cools, put it in a clean bottle or pitcher with a lid and store it in the refrigerator. Water bottles and ice trays should be cleaned with soap and water before each use. Nationally distributed brands of bottled or canned carbonated soft drinks are generally safe to drink. Commercially packaged, non-carbonated soft drinks and fruit juices that do not require refrigeration until after they are opened. Nationally distributed brands of frozen fruit juice concentrate are safe if they are reconstituted by the user with water from a safe water source. Fruit juices that must be refrigerated from the time they are processed to the time of consumption are either fresh. If extra steps are required to make water safe, this safe water should be used to wash fruits and vegetables. Because cooking food kills Cryptosporidium, cooked food and heat-processed foods are generally safe if, after cooking or processing, they are not handled by someone infected with the parasite or exposed to contaminated water. Ingesting ice made from tap water, raw fruits, and raw vegetables should also be avoided. Steaming-hot foods, self-peeled fruits, bottled and canned processed drinks, and hot coffee or hot tea are generally safe. However, if the patient is diapered or incontinent, contact precautions should be used for the duration of illness. In addition, contact precautions may be used to control institutional outbreaks of cryptosporidiosis. To reduce the risk of exposure to feces, adolescents should use dental dams or similar barrier methods for oral-anal and oral-genital contact, wear latex gloves during digital-anal contact, and change condoms after anal intercourse. Frequent washing of hands and genitals with warm, soapy water during and after sexual activities that could bring these body parts in contact with feces might further reduce the risk of Cryptosporidium infection. Supportive care with hydration, correction of electrolyte abnormalities, and nutritional supplementation should be provided. Antimotility agents to combat malabsorption of nutrients and drugs should be used with caution. No severe adverse events were reported, and adverse events that were reported were similar in the treatment and placebo groups in this study.
Syndromes
There is some evidence that butyrate also has antiproliferative activity, and so provides protection against colorectal cancer. Congenital deficiency of lactase occurs rarely in infants, leading to lactose intolerance and failure to thrive when fed on breast milk or normal infant formula. Congenital deficiency of sucraseisomaltase occurs among the Inuit, leading to sucrose intolerance, with persistent diarrhea and failure to thrive when the diet contains sucrose. In most mammals, and most human beings, lactase activity begins to fall after weaning, and is almost completely lost by late adolescence, leading to lactose intolerance. Lactose remains in the intestinal lumen, where it is a substrate for bacterial fermentation to lactate, resulting in abdominal discomfort and diarrhea after consumption of relatively large amounts. In two population groups, people of north European origin and nomadic tribes of sub-Saharan Africa and Arabia, lactase persists after weaning and into adult life. Marine mammals secrete a high-fat milk that contains no carbohydrate, and their pups lack lactase. Because they are not actively transported, fructose and sugar alcohols are only absorbed down their concentration gradient, and after a moderately high intake, some may remain in the intestinal lumen, acting as a substrate for bacterial fermentation. It is specific for the primary ester links-ie, positions 1 and 3 in triacylglycerols-resulting in 2-monoacylglycerols and free fatty acids as the major end products of luminal triacylglycerol digestion. Bile salts, formed in the liver and secreted in the bile, permit emulsification of the products of lipid digestion into micelles together with phospholipids and cholesterol from the bile. Because the micelles are soluble, they allow the products of digestion, including the fat-soluble vitamins, to be transported through the aqueous environment of the intestinal lumen and permit close contact with the brush border of the mucosal cells, allowing uptake into the epithelium. The bile salts pass on to the ileum, where most are absorbed into the enterohepatic circulation (Chapter 26). Within the intestinal epithelium, 1-monoacyglycerols are hydrolyzed to fatty acids and glycerol and 2-monoacylglycerols are reacylated to triacylglycerols via the monoacylglycerol pathway. Glycerol released in the intestinal lumen is not reutilized but passes into the portal vein; glycerol released within the epithelium is reutilized for triacylglycerol synthesis via the normal phosphatidic acid pathway (Chapter 24). These are hydrophobic molecules, and have to be hydrolyzed and emulsified to very small droplets (micelles) before they can be absorbed. The fat-soluble vitamins, A, D, E, and K, and a variety of other lipids (including cholesterol) are absorbed dissolved in the lipid micelles. Hydrolysis of triacylglycerols is initiated by lingual and gastric lipases, which attack the sn-3 ester bond forming 1,2-diacylglycerols and free fatty acids, aiding emulsification. The values given for percentage uptake may vary widely but indicate the relative importance of the three routes shown. Short- and medium-chain fatty acids are mainly absorbed into the hepatic portal vein as free fatty acids. Cholesterol is absorbed dissolved in lipid micelles, and is mainly esterified in the intestinal mucosa before being incorporated into chylomicrons. Unesterified cholesterol and other sterols are actively transported out of the mucosal cells into the intestinal lumen. Plant sterols and stanols (in which the B ring is saturated) compete with cholesterol for esterification, but are poor substrates. They therefore reduce the absorption of cholesterol, and act to lower serum cholesterol. Free Amino Acids & Small Peptides Are Absorbed by Different Mechanisms the end product of the action of endopeptidases and exopeptidases is a mixture of free amino acids, di- and tripeptides, and oligopeptides, all of which are absorbed. Free amino acids are absorbed across the intestinal mucosa by sodium-dependent active transport. There are several different amino acid transporters, with specificity for the nature of the amino acid side-chain (large or small, neutral, acidic or basic). The various amino acids carried by any one transporter compete with each other for absorption and tissue uptake.
On per vaginum and speculum examination, the cervix is ulcerated and bleeds on touch. On physical examination, there is fissuring and ulceration of the areola and nipple. Deep palpation of the breast shows a hard lump 5 cm in diameter, with irregular margins underneath the nipple. There is a history of presence of small waxy nodule initially for about one year which slowly increased in size followed by its ulceration. On examination, there is a single nodule with central ulceration, 4 mm in diameter, having pearly white rolled up margins. She also complains of irregular and heavy periods, weight loss, intermittent headache, nervousness, palpitation, excessive sweating and tremors in both hands. On physical examination, the thyroid gland is diffusely enlarged, nontender and prominent but there is no nodularity. He is a known case of diabetes for 7 years and hypertension for the last 10 years and has been on irregular treatment and intermittent follow up. An X-ray of the right knee shows an expanded and osteolytic mass in the right lower femur in the region of metaphysis. It has been growing rapidly and lately he has noticed that he has started having tightness of shirt on this side due to increase in size of swelling. On examination, the swelling is 6 x 4 cm size, firm to hard subcutaneous mass which is fixed to underlying soft tissues. He gives history of hypertension for 12 years, diabetes mellitus for 10 years and has been a smoker for 30 years before he quit smoking 10 years back. He has been well with treatment for hypertension and diabetes mellitus except for occasional episodes of angina which were relieved by rest. September 2015 Patient Adoption of mHealth Use, Evidence and Remaining Barriers to Mainstream Acceptance Introduction the availability of consumer apps continues to grow, particularly in the area of healthcare apps. Commonly referred to as mHealth apps, these apps assist consumers in self-management of overall wellness, disease prevention and disease management. Recognition of the importance of patients taking an active and informed role in their own healthcare has fueled this growth. The proliferation of smart phones and consumer interest in taking a more active role in their health, presents a significant opportunity to leverage mHealth apps in innovative ways. This is especially true as improvements are made in the connectivity aspects of mHealth apps both in how data is compiled and how it is connected back to healthcare providers. The primary focus of this report is on the consumer or patient use of mHealth apps. The mHealth app availability and usage information is focused on apps available to the general public that support everyday healthcare management in conjunction with their healthcare provider. While the information is agnostic to geographic boundaries, this report is primarily focused on the U. Throughout this report, the term "prescribe" is used in a manner to differentiate between an informal recommendation of mHealth apps by healthcare providers and a "prescriptive" specific recommendation to patients for use of an mHealth app as part of treatment protocols. The individuals below have participated in interviews, roundtable discussions and chapter reviews. Executive summary the number of mHealth apps available to consumers now exceeds 165,000 and since 2013 there has been progress in understanding and addressing the barriers to more mainstream adoption of mHealth. Apple iTunes store and Google Play (Android) provides an assessment of the current availability and use of mHealth apps. Similar to the study performed in 2013, the majority of available mHealth apps continue to be concentrated in the areas of wellness, diet and exercise. Nearly a quarter of mHealth apps focus on disease and treatment management reflecting the growing interest in the use of mHealth apps for chronic disease management. When looking at overall functionality and scope of the features, over 50% of mHealth apps continue to have limited functionality, most simply providing information. One in ten mHealth apps have the capability to connect to a device or sensor which greatly improves the accuracy and convenience of data collection for mHealth apps.
Genetic deficiencies of each of the five enzymes of the urea cycle, as well as deficiencies in N-acetyglutamate synthase, have been described. The accumulation of citrulline (but not argininosuccinate) in the plasma of this patient means that the enzyme required for the conversion of citrulline to argininosuccinate (argininosucinate synthetase) is defective, whereas the enzyme that cleaves argininosuccinate (argininosuccinate lyase) is functional. Deficiencies of the enzymes of the urea cycle result in the failure to synthesize urea and lead to hyperammonemia in the first few weeks after birth. Glutamine will also be elevated because it acts as a nontoxic storage and transport form of ammonia. Ornithine will be combined with carbamoyl phosphate by ornithine transcarbamoylase to form citrulline. These pathways converge to form seven intermediate products: oxaloacetate, pyruvate, -ketoglutarate, fumarate, succinyl coenzyme A (CoA), acetyl CoA, and acetoacetate. In contrast, the essential amino acids cannot be synthesized (or produced in sufficient amounts) by the body and, therefore, must be obtained from the diet in order for normal protein synthesis to occur. Genetic defects in the pathways of amino acid metabolism can cause serious disease. Ketogenic amino acids Amino acids whose catabolism yields either acetoacetate or one of its precursors (acetyl CoA or acetoacetyl CoA) are termed ketogenic (see Figure 20. Acetoacetate is one of the ketone bodies, which also include 3-hydroxybutyrate and acetone (see p. Leucine and lysine are the only exclusively ketogenic amino acids found in proteins. Their carbon skeletons are not substrates for gluconeogenesis and, therefore, cannot give rise to the net synthesis of glucose. Aspartate loses its amino group by transamination to form oxaloacetate (see Figure 20. This makes asparagine an essential amino acid for these cells, which, therefore, require asparagine from the blood. Asparaginase, which hydrolyzes asparagine to aspartate, can be administered systemically to treat leukemic patients. Asparaginase lowers the level of asparagine in the plasma, thereby depriving cancer cells of a required nutrient. For example, supplementation with glutamine and arginine has been shown to improve outcomes in patients with trauma, postoperative infections, and immunosuppression. Glutamine: this amino acid is hydrolyzed to glutamate and ammonium by the enzyme glutaminase (see p. Glutamate is converted to -ketoglutarate by transamination or through oxidative deamination by glutamate dehydrogenase (see p. Arginine: this amino acid is hydrolyzed by arginase to produce ornithine (and urea). Alanine: this amino acid loses its amino group by transamination to form pyruvate (Figure 20. Serine: this amino acid can be converted to glycine and N5,N10methylenetetrahydrofolate (Figure 20. Glycine: this amino acid can be converted to serine by the reversible addition of a methylene group from N5,N10-methylenetetrahydrofolic acid (see Figure 20. Deficiency of the transaminase in liver peroxisomes causes overproduction of oxalate, the formation of oxalate stones, and kidney damage (primary oxaluria type 1). Threonine: this amino acid is converted to pyruvate in most organisms but is a minor pathway (at best) in humans. Phenylalanine and tyrosine: Hydroxylation of phenylalanine produces tyrosine (Figure 20. This reaction, catalyzed by tetrahydrobiopterin-requiring phenylalanine hydroxylase, initiates the catabolism of phenylalanine. Thus, the metabolism of phenylalanine and tyrosine merge, leading ultimately to the formation of fumarate and acetoacetate. Inherited deficiencies: Inherited deficiencies in the enzymes of phenylalanine and tyrosine metabolism lead to the diseases phenylketonuria (see p. Amino acids that form succinyl coenzyme A: methionine Methionine is one of four amino acids that form succinyl CoA. Methionine is also the source of homocysteine, a metabolite associated with atherosclerotic vascular disease and thrombosis (see p. The methyl group is usually transferred to nitrogen (as with epinephrine) or oxygen atoms (as with the catechols; see p.
Their synthesis is increased or decreased by estrogen deficiency, with the overall effect of extending the life span of osteoclasts (by inhibiting apoptosis). In osteoporosis, bone mass decreases due to decreased bone formation and increased resorption, but a normal ratio of bone mineral (hydroxyapatite) to bone matrix (mostly collagen type 1) is preserved. Osteomalacia is also an example of osteopenia, but in it there is decreased mineralization; its commonest cause is deficiency of vitamin D. Primary osteoporosis can be divided into 3 types: idiopathic (uncommon, and occurs in children and young adults), postmenopausal, and involutional (elderly) types. This case is an example of postmenopausal osteoporosis, and decline in estrogen levels is a major factor in its causation. This type can also occur in males due to a decline of serum testosterone, which acts to increase osteoclastic activity. Involutional osteoporosis occurs in older individuals and is due to the decline of the number of osteoblasts with age. Secondary osteoporosis is relatively uncommon, and may be due to a variety of conditions (eg, chronic renal disease, various drugs [especially corticosteroids], a number of endocrine disorders, malabsorption syndrome, etc). An in-depth understanding of them requires a knowledge of bone modeling, of a variety of cytokines, of the actions of a number of hormones, and of various nutritional and genetic factors, among other considerations. In regards to post-menopausal osteoporosis in particular, one important consideration is that estrogen loss appears to increase the secretion of a number of cytokines that lead to recruitment of osteoclasts. Also, estrogen loss diminishes the secretion of certain other cytokines that promote osteoblastic activity. The overall effect is thus an imbalance between osteoclasts and osteoblasts, in favor of the former. Alterations of the levels of various factors (hormones, cytokines, nutritional) result in an increase of osteoclastic activity over osteoblastic activity. Resorption of bone with loss of matrix (mainly collagen type I, but also other proteins such as osteocalcin) with preservation of the ratio of matrix: mineral (hydroxyapatite). Fragility of bones, often resulting in fractures (hip fractures are among the most serious). History and Physical Examination An 8-year-old boy, an only child, presented at a dermatology clinic with a skin tumor on his right cheek. He had always avoided exposure to sunlight because it made his skin Simplified scheme of some major factors in the causation of osteoporosis. His skin had scattered areas of hyperpigmentation and other areas where it looked mildly atrophied. Laboratory Findings Histologic examination of the excised tumor showed that it was a squamous cell carcinoma (a common type of tumor skin cancer in older people, but very unusual in a boy of this age). A small piece of skin was removed for preparing fibroblasts to be grown in tissue culture. In E coli, an endonucleolytic cleavage, catalyzed by a specific endonuclease (also called an excinuclease), occurs on either side of the damage, releasing a 12- to 13-base-pair oligonucleotide. The most noticeable difference is that a much larger oligonucleotide (about 30 bases) is excised in humans. In the boy whose situation is discussed here, the specific gene involved was not determined. This indicated that one set of cells was providing a normal gene product to the other, thus correcting the defect. In this manner, at least seven complementation groups, corresponding to the seven genes and their products mentioned above, have been recognized. The parents of the boy in the present case were told that he would have to be watched closely throughout life for the development of new skin cancers. In addition, he was advised to avoid sunlight and to use an appropriate sunscreen ointment.
Regional lymph node metastases may occur but distant organ metastases are infrequent. The tumour is predominantly found in old age (7th-8th decades) and is slightly more common in females than in males (female-male ratio 1. G/A the tumour is generally large and irregular, often invading the adjacent strap muscles of the neck and other structures in the vicinity of the thyroid. Cut surface of the tumour is white and firm with areas of necrosis and haemorrhages. Small cell carcinoma this type of tumour is composed of closely packed small cells having hyperchromatic nuclei and numerous mitoses. Spindle cell carcinoma these tumours are composed of spindle cells resembling sarcoma. Some tumours may contain obvious sarcomatous component such as areas of osteosarcoma, chondrosarcoma or rhabdomyosarcoma. Giant cell carcinoma this type is composed of highly anaplastic giant cells showing numerous atypical mitoses, bizarre and lobed nuclei and some assuming spindle shapes. In the adults, each gland is an oval, yellowish-brown, flattened body, weighing 35-45 mg. M/E Parathyroid glands are composed of solid sheets and cords of parenchymal cells and variable amount of stromal fat. The parenchymal cells are of 3 types: chief cells, oxyphil cells and water-clear cells. The major function of the parathyroid hormone, in conjunction with calcitonin and vitamin D, is to regulate serum calcium levels and metabolism of bone. The role of parathyroid hormone in regulating calcium metabolism in the body is at the following 3 levels: 1. Parathyroid hormone stimulates osteoclastic activity and results in resorption of bone and release of calcium. Calcitonin released by C-cells, on the other hand, opposes parathyroid hormone by preventing resorption of bone and lowering serum calcium level. Parathyroid hormone acts directly on renal tubular epithelial cells and increases renal reabsorption of calcium and inhibits reabsorption of phosphate; calcitonin enhances renal excretion of phosphate. Parathyroid hormone increases renal production of the most active metabolite of vitamin D, i. Metastatic calcification, especially in the blood vessels, kidneys, lungs, stomach, eyes and other tissues. Generalised osteitis fibrosa cystica due to osteoclastic resorption of bone and its replacement by connective tissue. Hypocalcaemia stimulates compensatory hyperplasia of the parathyroid glands and causes secondary hyperparathyroidism. Chronic renal insufficiency resulting in retention of phosphate and impaired intestinal absorption of calcium. Vitamin D deficiency and consequent rickets and osteomalacia may cause parathyroid hyperfunction. The patients with secondary hyperparathyroidism have signs and symptoms of the disease which caused it. Possibly, a hyperplastic nodule in the parathyroid gland develops which becomes partially autonomous and continues to secrete large quantities of parathyroid hormone without regard to the needs of the body. Most common causes of primary hypoparathyroidism are: surgical procedures involving thyroid, parathyroid, or radical neck dissection for cancer. The patients are generally females and are characterised by signs and symptoms of hypoparathyroidism and other clinical features like short stature, short metacarpals and metatarsals, flat nose, round face and multiple exostoses. It may occur at any age and in either sex but is found more frequently in adult life. Most adenomas are first brought to attention because of excessive secretion of parathyroid hormone causing features of hyperparathyroidism as described above. G/A A parathyroid adenoma is small (less than 5 cm diameter) encapsulated, yellowish-brown, ovoid nodule and weighing up to 5 gm or more. M/E Majority of adenomas are predominantly composed of chief cells arranged in sheets or cords. Oxyphil cells and water-clear cells may be found intermingled in varying proportions. The discussion here is focused on the endocrine pancreas and its two main disorders: diabetes mellitus and islet cell tumours.
References:




