Fluid motions, steatorrhoea, abdominal pain, nausea, flatulence and vitamin deficiency are the side effects. Olestra is a sucrose polyester which can be used as a cooking medium in place of fat but is neither digested nor absorbed. Leptin (the endogenous slimming peptide) analogues, neuropeptide Y antagonists and 3 adrenergic agonists are under investigation as antiobesity drugs. Nocturnal enuresis in children and urinary incontinence Amphetamine affords benefit both by its central action as well as by increasing tone of vesical sphincter. Uterine relaxant Isoxsuprine has been used in threatened abortion and dysmenorrhoea, but efficacy is doubtful. Insulin hypoglycaemia Adr may be used as an expedient measure, but glucose should be given as soon as possible. Nasal stuffiness and miosis result from blockade of receptors in nasal blood vessels and in radial muscles of iris respectively. Intestinal motility is increased due to partial inhibition of relaxant sympathetic influences- loose motion may occur. This is accentuated by reflex increase in renin release mediated through 1 receptors. Contractions of vas deferens and related organs which result in ejaculation are coordinated through receptors- blockers can inhibit ejaculation; this may manifest as impotence. The blockers have no effect on adrenergic cardiac stimulation, bronchodilatation, vasodilatation and most of the metabolic changes, because these are mediated predominantly through receptors. These are drugs which antagonize the receptor action of adrenaline and related drugs. They are competitive antagonists at or or both and adrenergic receptors and differ in important ways from the "adrenergic neurone blocking agents", which act by interfering with the release of adrenergic transmitter on nerve stimulation. The pharmacological profile of an blocker is mainly governed by its central effects and by the relative activity on 1 and 2 receptor subtypes. Phenoxybenzamine It cyclizes spontaneously in the body giving rise to a highly reactive ethyleniminium intermediate which reacts with adrenoceptors and other biomolecules by forming strong covalent bonds. The blockade is of nonequilibrium (irreversible) type and develops gradually (even after i. In recumbent subjects cardiac output and blood flow to many organs is increased due to reduction in peripheral resistance and increased venous return. It tends to shift blood from pulmonary to systemic circuit because of differential action on the two vascular beds. Major side effects are postural hypotension, palpitation, nasal blockage, miosis, inhibition of ejaculation. Pharmacokinetics Oral absorption of phenoxybenzamine is erratic and incomplete; i. Though most of the administered dose is excreted in urine in 24 hours, small amounts that have covalently reacted remain in tissues for long periods. The amino acid alkaloids ergotamine and ergotoxine are partial agonists and antagonists at adrenergic, serotonergic and dopaminergic receptors. The natural ergot alkaloids produce long lasting vasoconstriction which predominates over their blocking action-peripheral vascular insufficiency and gangrene of toes and fingers occurs in ergotism. Ergotoxine is a more potent blocker and less potent vasoconstrictor than ergotamine. Phentolamine this is a rapidly acting blocker with short duration of action (in minutes). This is unrelated to 1 receptor blockade, but may retard the progression of prostatic hypertrophy. Prazosin It is first of the highly selective 1 blockers having 1: 2 selectivity ratio 1000:1. Other blocking side effects (miosis, nasal stuffiness, inhibition of ejaculation) are also milder. For the above reasons, prazosin (also other 1 blockers) has largely replaced phenoxybenzamine. Prazosin is effective orally (bioavailability ~60%), highly bound to plasma proteins (mainly to 1 acid glycoprotein), metabolized in liver and excreted primarily in bile. Prazosin blocks 1 receptors in bladder trigone and prostatic smooth muscle, thereby improves urine flow, reduces residual urine in bladder.
Gastric lavage to remove unabsorbed drug; alkaline diuresis or haemodialysis to remove absorbed drug is indicated in severe cases. Precautions and contraindications · Aspirin is contraindicated in patients who are sensitive to it and in peptic ulcer, bleeding tendencies, in children suffering from chicken pox or influenza. Aspirin displaces warfarin, naproxen, sulfonylureas, phenytoin and methotrexate from binding sites on plasma proteins: toxicity of these drugs may occur. Its antiplatelet action increases the risk of bleeding in patients on oral anticoagulants. Aspirin at analgesic doses inhibits tubular secretion of uric acid and antagonizes uricosuric action of probenecid. Aspirin blunts diuretic action of furosemide and thiazides and reduces K+ conserving action of spironolactone. Competition between canrenone (active metabolite of spironolactone) and aspirin for active transport in proximal tubules has been demonstrated. Aspirin reduces protein bound iodine levels by displacement of thyroxine; but hypothyroidism does not occur. As analgesic For headache (including mild migraine), backache, myalgia, joint pain, pulled muscle, toothache, neuralgias and dysmenorrhoea; it is effective in low doses (0. As antipyretic Aspirin is effective in fever of any origin; dose is same as for analgesia. Antipyretics are not useful in fever due to heat stroke; only external cooling lowers body temperature. Acute rheumatic fever Aspirin is the first drug to be used in all cases; other drugs are added or substituted only when it fails or in severe cases (corticosteroids act faster). In a dose of 45 g or 75100 mg/kg/day (in divided portions producing steady state serum salicylate concentration 1530 mg/dl) it brings about marked symptomatic relief in 13 days. Granulomatous lesions, nodules, cardiac complications, valvular defects, chorea and duration of disease are not altered by salicylate therapy. Rheumatoid arthritis Aspirin in a dose of 35 g/day is effective in most cases; produces relief of pain, swelling and morning stiffness, but progress of the disease process is not affected. Postmyocardial infarction and poststroke patients By inhibiting platelet aggregation aspirin lowers the incidence of reinfarction. Some authorities recommend it for primary prophylaxis as well, but the risk of bleeding has to be weighed against the possible benefit. All have similar pharmacodynamic properties but differ considerably in potency and to some extent in duration of action (Table 14. Inhibition of platelet aggregation is short-lasting with ibuprofen, but longer lasting with naproxen. Adverse effects Ibuprofen and all its congeners are better tolerated than aspirin. Gastric discomfort, nausea and vomiting, though less than aspirin or indomethacin, are still the most common side effects. They are not to be prescribed to pregnant women and should be avoided in peptic ulcer patient. Pharmacokinetics and interactions All are well absorbed orally, highly bound to plasma proteins (9099%), but displacement interactions are not clinically significant-dose of oral anticoagulants and oral hypoglycaemics need not be altered. Because they inhibit platelet function, use with anticoagulants should, nevertheless, be avoided. They are largely metabolized in liver by hydroxylation and glucuronide conjugation and excreted in urine as well as bile. Ibuprofen is used as a simple analgesic and antipyretic in the same way as low dose of aspirin. Ibuprofen and its congeners are widely used in rheumatoid arthritis, osteoarthritis and other musculoskeletal disorders, especially where pain is more prominent than inflammation. They are indicated in soft tissue injuries, fractures, vasectomy, tooth extraction, postpartum and postoperatively: suppress swelling and inflammation. Ibuprofen (400 mg) has been found equally or more efficacious than a combination of aspirin (650 mg) + codeine (60 mg) in relieving dental surgery pain, but is a weaker antiinflammatory; not suitable for acute gout and other similar conditions. Naproxen is marketed as active single S() enantiomer preparation, which poses less renal burden. It is highly bound to plasma proteins-displacement interactions can occur; partly metabolized and excreted in urine as well as bile.
In the end it should be ensured that the instructions have been properly understood by the patient. Under specified storage conditions, the product is expected to remain stable (retain >95% potency) during this period. In India, the schedule P (Rule 96) of Drugs and Cosmetics Act (1940) specifies the life period (mostly 15 years) of drugs and the conditions of storage. The expiry of other medicines has to be specified by the manufacturer, but cannot exceed 5 years, unless permitted by the licencing authority on the basis of satisfactory stability proof. The shelf-life of a medicine is determined by real time stability studies or by extrapolation from accelerated degradation studies. The expiry date does not mean that the medicine has actually been found to lose potency or become toxic after it, but simply that quality of the medicine is not assured beyond the expiry date, and the manufacturer is not liable if any harm arises from the use of the product. Infact, studies have shown that majority of solid oral dosage forms (tablets/capsules, etc. Injectable solutions may develop precipitates, become cloudy or discoloured by prolonged storage. Adrenaline injection (in ampoules) has been found to lose potency few months after the expiry date of 1 year (it gets oxidized). The degradation product of only one drug (tetracycline) has caused toxicity in man. Outdated tetracycline capsules produced renal tubular damage resembling Fanconi syndrome in the early 1960s. Though, majority of medicines, especially solid oral dosage forms, remain safe and active years after the stated expiry date, their use cannot be legally allowed beyond this date. Evidence-based medicine is the process of systematically finding, evaluating and using contemporary research findings as the basis of clinical decisions. Results of well designed multicentric interventional trials are forming the basis of constantly evolving guidelines for disease management. Therapeutic evaluation of a drug includes: · Quantitation of benefit afforded by it. Case control studies Clinical trial It is a prospective ethically designed investigation in human subjects to objectively discover/verify/ compare the results of two or more therapeutic measures (drugs). Clinical trials are designed to answer one or more precisely framed questions about the value of treating equivalent groups of patients by two or more modalities (drugs, dosage regimens, other interventions). Depending on the objective of the study, clinical trial may be conducted in healthy volunteers or in volunteer patients. Healthy volunteers may be used to determine pharmacokinetic characteristics, tolerability, safety and for certain type of drugs. The ethics committee has to ensure that the study does not breach the ethical principles of: Autonomy: Freedom, dignity and confidentiality of the subject; right to choose whether or not to participate in the trial or to continue with it. Non-maleficence: Not to do harm or put the participant at undue risk/disadvantage. Justice: Observence of fairness, honesty and impartiality in obtaining, analysing and communicating the data. Controlled trial the inclusion of a proper comparator (control) group in clinical trials is crucial. The control group, which should be as similar to the test group as possible, receives either a placebo (if ethically permissible) or the existing standard treatment (active control). Separate test and control groups may run simultaneously (parallel group design), or all the subjects may be treated by the two options one after the other (cross over design) so that the same subjects serve as their own controls. This design is applicable only to certain chronic diseases which remain stable over long periods. When one drug is compared to another drug or to a placebo, the dosage regimen (dose, frequency, duration) of the drug is decided in advance. To determine the most appropriate dose, separate dose-ranging studies (trials) have to be performed. It is well known that both the participants and the investigators of the trial are susceptible to conscious as well as unconscious bias in favour of or against the test drug. The greatest challenge in the conduct of clinical trial is the elimination of bias.
Ehrlich produced organic arsenicals for cure of syphilis, and some organic arsenicals were used in amoebiasis till 1960s. Adverse effects of arsenic are nausea, dizziness, malaise, fatigue, sensory disturbances, effusions, breathlessness, hyperglycaemia, Q-T prolongation, A-V block. Designing and development of drugs to attack these targets is an active area of current research. These drugs are primarily of two types: · Specific monoclonal antibodies that need to be given parenterally, and attack cell surface targets or tumour antigens. Only a sample of these drugs, especially those available in India, are presented here. Tyrosine-protein kinase inhibitors Imatinib It is the first selectively targeted drug to be introduced for treatment of a malignancy. Resistance to imatinib develops by point mutations in Bcr-Abl tyrosine kinase affecting its affinity for imatinib. Gefitinib monotherapy has been used for locally advanced or metastatic lung cancers after cisplatin and docetaxal have failed. Erlotinib It is similar to gefitinib in action, pharmacokinetics, adverse effects and efficacy in a subtype of non-small cell lung cancer. It has been combined with gemcitabine for advanced/ metastatic pancreatic cancer as well. Few cases of serious hepatic dysfunction have occured in patients with preexisting liver disease. Binding to the receptor, it prevents transmembrane signalling resulting in blockade of cell growth, proliferation and metastasis. Angiogenesis inhibitors Angiogenesis (proliferation of new blood vessels) is essential for growth and metastasis of cancers. Added to conventional chemotherapy, it improves survival in metastatic non-small cell lung cancer, breast cancer, clear cell renal carcinoma and glioblastoma. Deafness due to neurofibromatosis can be reversed by growth inhibitory effect of bevacizumab. The prime indication of bortezomib is multiple myeloma, both for first line combined therapy (along with cytotoxic drugs), as well as for relapsed disease. Others are diarrhoea, fatigue, bone marrow depression, especially thrombocytopenia. This hybridoma is then cloned so that the single species antibody is obtained in large quantity. Proteasome inhibitor Proteasomes are packaged complexes of proteolytic enzymes which degrade several intracellular signalling proteins that control cell cycle, apoptosis and survival response. Bortezomib It is a unique boron containing compound that covalently binds to proteasome and inhibits its proteolytic activity disrupting many intracellular signalling pathways. They could also be used as missiles to carry biological bombs (toxins) and are called immunotoxins, or a radioactive isotope as radiopharmaceuticals. It is indicated in B-cell lymphoma, non-Hodgkin lymphoma and chronic lymphocytic leukaemia, both as single agent as well as in combination with cytotoxic chemotherapy. Survival benefits have been obtained both when it is used as initial therapy as well as in relapsed cases. Adverse effects are infusion reactions consisting of chills, fever, urticarial rashes, pruritus, dyspnoea and hypotension. Moreover, they afford symptomatic relief by antipyretic and mood elevating action and potentiate the antiemetic action of ondansetron/metoclopramide. Prednisolone/dexamethasone are most commonly used; doses are high-hypercorticism may occur (see Ch. Fosfestrol It is the phosphate derivative of stilbestrol; has been specifically used in carcinoma prostate. The above three classes of drugs are the sheet anchor of adjuvant and palliative therapy of carcinoma breast, as well as for primary and secondary prevention of breast cancer (see Ch.
Cardiovascular system: A high dose of caffeine has positive inotropic and chronotropic effects on the heart. In others, an accelerated heart rate can trigger premature ventricular contractions. Diuretic action: Caffeine has a mild diuretic action that increases urinary output of sodium, chloride, and potassium. Gastric mucosa: Because all methylxanthines stimulate secretion of hydrochloric acid from the gastric mucosa, individuals with peptic ulcers should avoid beverages containing methylxanthines. Therapeutic uses: Caffeine and its derivatives relax the smooth muscles of the bronchioles. Adverse effects: Moderate doses of caffeine cause insomnia, anxiety, and agitation. A high dosage is required for toxicity, which is manifested by emesis and convulsions. The lethal dose is about 10 g of caffeine (about 100 cups of coffee), which induces cardiac arrhythmias; death from caffeine is thus highly unlikely. Lethargy, irritability, and headache occur in users who have routinely consumed more than 600 mg of caffeine per day (roughly six cups of coffee per day) and then suddenly stop. Although this drug is not currently used therapeutically (except in smoking cessation therapy, see p. In combination with the tars and carbon monoxide found in cigarette smoke, nicotine represents a serious risk factor for lung and cardiovascular disease, various cancers, as well as other illnesses. Mechanism of action: In low doses, nicotine causes ganglionic stimulation by depolarization. Cigarette smoking or administration of low doses of nicotine produces some degree of euphoria and arousal as well as relaxation. High doses of nicotine result in central respiratory paralysis and severe hypotension caused by medullary paralysis (Figure 10. Stimulation of sympathetic ganglia as well as the adrenal medulla increases blood pressure and heart rate. Many patients with peripheral vascular disease experience an exacerbation of symptoms with smoking. For example, nicotine-induced vasoconstriction can decrease coronary blood flow, adversely affecting a patient with angina. Stimulation of parasympathetic ganglia also increases motor activity of the bowel. At higher doses, blood pressure falls, and activity ceases in both the gastrointestinal tract and bladder musculature as a result of a nicotine-induced block of parasympathetic ganglia. Pharmacokinetics: Because nicotine is highly lipid soluble, absorption readily occurs via the oral mucosa, lungs, gastrointestinal mucosa, and skin. Nicotine crosses the placental membrane and is secreted in the milk of lactating women. By inhaling tobacco smoke, the average smoker takes in 1 to 2 mg of nicotine per cigarette (most cigarettes contain 6 to 8 mg of nicotine). Clearance of nicotine involves metabolism in the lung and the liver and urinary excretion. Tolerance to the toxic effects of nicotine develops rapidly, often within days after beginning usage. Nicotine may also cause intestinal cramps, diarrhea, and increased heart rate and blood pressure. In addition, cigarette smoking increases the rate of metabolism for a number of drugs. Withdrawal syndrome: As with the other drugs in this class, nicotine is an addictive substance, and physical dependence on nicotine develops rapidly and can be severe (Figure 10. Withdrawal is characterized by irritability, anxiety, restlessness, difficulty concentrating, headaches, and insomnia. For example, the blood concentration of nicotine obtained from nicotine chewing gum is typically about one-half the peak level observed with smoking (Figure 10. Because it is only a partial agonist at these receptors, it produces less euphoric effects than those produced by nicotine itself (nicotine is a full agonist at these receptors).
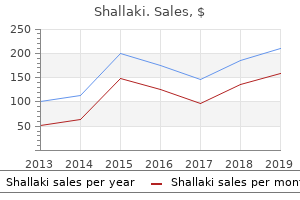
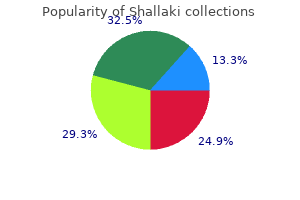
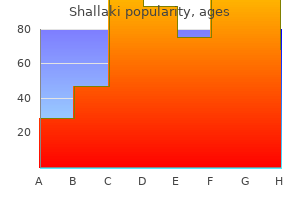
Niauli Oil. Shallaki.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96576
Etiologic classification 1) Ischemic -stroke accounts for 80 90% of all stroke in developed countries a) Embolic b) Thrombotic i) Large vessel disease: resulting from narrowing of cerebral arteries doe to atherosclerosis. Vasculitis resulting thrombus formation 2) Hemorrhagic Stroke: accounts for 10-20 % of cerebrovascualr accidents in developed nations. It is third commonest cause of death in developed world following Coronary heart diseases and cancer. The prevalence and incidence of stroke is also on the rise in developing countries. Major risk factors associated with stroke include · · · · · · · · · Incidence is higher in men and old age Hypertension Smoking Diabetic mellitus Hyperlipidemia Atrial fibrillation Myocardial infarction Congestive heart failure Acute alcohol abuse Approach to a patient with stroke: Goals /Steps 1. Initial Assessment and maintenance of vital functions/stabilizing the patient Stroke should be considered as medical emergency, as it affects vital functions of an individual. For this reason the initial step in management of patients with acute stroke should be rapid assessment and maintenance of vital functions. This includes: 508 Internal Medicine a) Maintenance of air way and ventilation b) Control of blood pressure Acute stroke alters autoregulation of cerebral blood flow, compromising the blood supply to an already damaged brain. Close monitoring of blood pressure and correction of both hypotension and hypertension reduces this risk. If the patient is hypotensive, it should be corrected by fluid administration and treatment of the underlying cause for the hypotension. Because fever worsens the prognosis of stroke body temperature should be controlled appropriately. Glucose is said to be neurotoxic and it is better avoided in patients with stroke. B Exclude causes of brain dysfunction, which mimic stroke like states like syncope, migraine, hysteria and trauma. Determine Presumptive Diagnosis of Stroke Subtype Numbers of clinical features are useful in determining the type of stroke. A good history taking, and proper physical examination may suggest the possible cause of the stroke. Important historical information includes: · Mode of onset and pattern of progression o Embolisms usually occur suddenly when the patient is awake, most often early in the morning, giving maximum deficit at onset. Very severe headache with altered consciousness without major neurologic deficit may suggest subarachnoid hemorrhage. Physical Examination · · · · · · Physical Findings may give clue to the type of stroke the patient is suffering from. Absent/reduced peripheral pulses suggest atherosclerosis or embolism Presence of neck bruit suggests extra cranial occlusion of carotid arteries Cardiac abnormalities: such as atrial fibrillation, murmurs or cardiac enlargement may suggest embolic stroke, the embolus originating from the heart. Fever raises concern for infectious etiologies Ophthalmoscopic examination: papilledma or retinal hemorrhage may suggest subarachnoid hemorrhage or increased intracranial pressure. Confirmation of Diagnosis: different investigations are needed to confirm the diagnosis. Management of specific stroke Goal of Treatment · · · · Interruption of further brain damage Prevention and management of complication A. General Measures Admit the patients where close follow up can be given Continue follow up and maintenance of vital functions. Anticoagulation with heparin should be initiated when the acute phase of stroke is over. Impairment of consciousness and Coma Learning objectives: at the end of this lesson the student will be able to: 1. Introduction Maintenance of conscious state requires proper functioning of the cerebral hemispheres, reticular activating system found in brain stem and corticothalmic connections. Stupor is a sleep like unarousability, from which the patient can be awakened by vigorous stimuli. Drowsiness: is a state of reduced consciousness characterized by easy arousal that can be maintained only for brief period of time. Autonomic functions are relatively well maintained, and a sleep-wake cycle exists. If there is structural, metabolic or toxic insult of diffuse nature to these structures results in alteration of Etiologies 1. The loss of consciousness in such patients is diffuse bilateral hemispheric impairment, and such patients have normal brainstem function. Some of the causes include:- 515 Internal Medicine · Metabolic disturbances such as: hepatic encephalopathy,uremic encephalopathy,hypoglycemia, diabetic ketoacidosis.
Syndromes
More commonly, multiple drugs are used to treat a patient who is suffering from two or more diseases at the same time. The chances of unintended/adverse drug interactions are greater in this later situation, because an assortment of different drugs may be administered to a patient depending on his/her diseases/symptoms. Several drug interactions are desirable and deliberately employed in therapeutics. These are well-recognized interactions and do not pose any undue risk to the patient. The focus of attention in this chapter are drug interactions which may interfere with the therapeutic outcome or be responsible for adverse effects, or may even be fatal (bleeding due to excessive anticoagulant action). More importantly, a large section of patients may be receiving one or several drugs for their chronic medical conditions like hypertension, diabetes, arthritis, etc. The physician may prescribe certain drugs which may interact with those already being taken by the patient and result in adverse consequences. It is, therefore, imperative for the doctor to elicit a detailed drug history of the patient and record all the medication that he/she is currently on. The list of potential adverse drug interactions is already quite long and constantly growing. It is practically impossible for anyone to know/remember all possible drug interactions. Fortunately, the clinically important and common drug interactions that may be encountered in routine practice are relatively few. More exhaustive Regular medication drugs (Likely to be involved in drug interactions) 1. Certain types of drugs (see box) can be identified that are most likely to be involved in clinically important drug interactions. The physician may take special care and pay attention to the possibility of drug interactions when the patient is receiving one or more of such medications, or when the doctor intends to prescribe any of such drugs. Types of drugs most likely to be involved in clinically important drug interactions · Drugs with narrow safety margin. In certain cases, however, the mechanisms are complex and may not be well understood. Few interactions take place even outside the body when drug solutions are mixed before administration. Pharmacokinetic interactions these interactions alter the concentration of the object drug at its site of action (and consequently the intensity of response) by affecting its absorption, distribution, metabolism or excretion. Absorption Absorption of an orally administered drug can be affected by other concurrently ingested drugs. This is mostly due to formation of insoluble and poorly absorbed complexes in the gut lumen, as occurs between tetracyclines and calcium/iron salts, antacids or sucralfate. Such interactions can be minimized by administering the two drugs with a gap of 23 hours so that they do not come in contact with each other in the g. Ketoconazole absorption is reduced by H2 blockers and proton pump inhibitors because they decrease gastric acidity which promotes dissolution and absorption of ketoconazole. Antibiotics like ampicillin, tetracyclines, cotrimoxazole markedly reduce gut flora that normally deconjugates oral contraceptive steroids secreted in the bile as glucuronides and permits their enterohepatic circulation. Several instances of contraceptive failure have been reported with concurrent use of these antibiotics due to lowering of the contraceptive blood levels. Alteration of gut motility by atropinic drugs, tricyclic antidepressants, opioids and prokinetic drugs like metoclopramide or cisapride can also affect drug absorption. Distribution Interactions involving drug distribution are primarily due to displacement of one drug from its binding sites on plasma proteins by another drug. Another requirement is that the displacing drug should bind to the same sites on the plasma proteins with higher affinity. Displacement of bound drug will initially raise the concentration of the free and active form of the drug in plasma that may result in toxicity. However, such effects are usually brief, because the free form rapidly gets distributed, metabolized and excreted, so that steady-state levels are only marginally elevated. Quinidine has been shown to reduce the binding of digoxin to tissue proteins as well as its renal and biliary clearance by inhibing the efflux transporter P-glycoprotein, resulting in nearly doubling of digoxin blood levels and toxicity. They may thus affect the bioavailability (if the drug undergoes extensive first pass metabolism in liver) and the plasma half-life of the drug (if the drug is primarily eliminated by metabolism).
It is nearly equipotent antitussive as codeine, especially useful in spasmodic cough. Dextromethorphan does not depress mucociliary function of the airway mucosa and is practically devoid of constipating action. The antitussive action of Bronchodilators Bronchospasm can induce or aggravate cough. Bronchodilators relieve cough in such individuals and improve the effectiveness of cough in clearing secretions by increasing surface velocity of airflow during the act of coughing. They should be used only when an element of bronchoconstriction is present and not routinely. Their fixed dose combinations with antitussives are not satisfactory because of differences in time course of action of the components and liability for indiscriminate use. Fixed dose combinations of a centrally acting antitussive with a bronchodilator or with an antihistaminic having high atropinic activity have been banned in India, but many are still marketed. Though it has been shown to reduce experimentally induced cough in healthy volunteers, there is no evidence of benefit in pathological cough. Asthma is now recognized to be a primarily inflammatory condition: inflammation underlying hyperreactivity. An allergic basis can be demonstrated in many adult, and higher percentage of pediatric patients. In others, a variety of trigger factors (infection, irritants, pollution, exercise, exposure to cold air, psychogenic) may be involved: Extrinsic asthma: It is mostly episodic, less prone to status asthmaticus. These mediators together constrict bronchial smooth muscle, cause mucosal edema, hyperemia and produce viscid secretions, all resulting in reversible airway obstruction. The inflammation perpetuates itself by cell-to-cell communication and recruitment of more and more inflammatory cells. Bronchial smooth muscle hypertrophy, increase in the population of mucus secreting cells and blood vessels occurs over time and damage to bronchial epithelium accentuates the hyperreactivity. Loss of bronchiolar elasticity leads to closure of smaller air tubes during expiration. The airway obstruction is accentuated during exercise causing shortness of breath. The expiratory airflow limitation does not fluctuate markedly over long periods of time, but there are exacerbations precipitated by respiratory infections, pollutants, etc. It is clearly related to smoking and characteristically starts after the age of 40. Methylxanthines: Theophylline (anhydrous), Aminophylline, Choline theophyllinate, Hydroxyethyl theophylline, Theophylline ethanolate of piperazine, Doxophylline. Inhalational: Beclomethasone dipropionate, Budesonide, Fluticasone propionate, Flunisolide, Ciclesonide. Since 2 receptors on inflammatory cells desensitize quickly, the contribution of this action to the beneficial effect of 2 agonists in asthma where airway inflammmation is chronic, is uncertain, and at best minimal. Though adrenaline (1+2+ receptor agonist) and isoprenaline (1+2 agonist) are effective bronchodilators, it is the selective 2 agonists that are now used in asthma to minimize cardiac side effects. Salbutamol (Albuterol) A highly selective 2 agonist; cardiac side effects are less prominent. It is, therefore, used to abort and terminate attacks of asthma, but is not suitable for round-the-clock prophylaxis. Palpitation, restlessness, nervousness, throat irritation and ankle edema can also occur. Salbutamol undergoes presystemic metabolism in the gut wall, oral bioavailability is 50%. Oral salbutamol acts for 46 hours, is longer acting and safer than isoprenaline, but not superior in bronchodilator efficacy. Because of more frequent side effects, oral 2 agonist therapy is reserved for patients who cannot correctly use inhalers or as alternative/ adjuvant drugs in severe asthma. Single enantiomer preparation of R() salbutamol has also been marketed, because it is the active 2 agonist and more potent bronchodilator which may produce fewer side effects than the racemate.
It is a strong irritant, higher concentrations damage the epithelium and cause vesication-has been used to remove warts, etc. It is added to hair tonics-claimed to increase vascularity of scalp and promote hair growth. Methyl salicylate (oil of wintergreen) In contrast to other salicylates, it is not used internally (induces vomiting, gastritis and systemic toxicity). It is combined with other irritants in liniments and ointments for muscle and joint pain. Trichloroacetic acid As crystals or 1020% solution to cauterise adenoids; dilute solution is used to promote peeling of frackled skin. These drugs are used on hyperkeratotic lesions like corns, warts, psoriasis, chronic dermatitis, ringworm, athletes foot, etc. Salicylic acid As 1020% solution in alcohol or propylene glycol for dissolving corns. Applied under polyethylene occlusive dressing, it causes maceration of skin and acts as a keratolytic, supplementing the action of salicylic acid. An escharotic, in addition, precipitates proteins that exude to form a scab-gets fibrosed to form a tough scar. They are used to remove moles, warts (including genital warts) condylomata, papillomas and on keratotic lesions. Resorcinol Has antiseptic, antifungal, local irritant and keratolytic properties; 310% is used in eczema, seborrheic dermatitis, ringworm, etc. Urea Applied at a concentration of 520% in cream/ointment base, urea acts as a humectant by its hygroscopic and water retaining property. It causes softening and solubilization of keratin, facilitating its removal from hyperkeratinized lesions like ichthyosis, lichen planus. A causal role of the yeast Pityrosporum ovale has been shown, but various trigger factors like change in quantity and composition of sebum, increase in alkalinity of skin (due to increased sweating), external local factors, emotional stress, genetic predisposition appear to be needed to transform the yeast from a commensal to a noninvasive pathogenic organism. Dryness, folliculitis and dandruff are benefited, but > 50% patients relapse on discontinuation. Systemic absorption and toxicity can occur if it is applied to inflamed or damaged skin. Good to excellent results have been obtained with these preparations without skin irritation, contact sensitivity, phototoxicity or systemic adverse effects. They have minimal antiyeast action: may benefit seborrhoea by keratolytic and antiseptic properties. Salicylic acid It is keratolytic, has mild effect in seborrhoea, probably by removing the scales and by improving penetration of other drugs. Psoralens are furocoumarins which on photoactivation stimulate melanocytes and induce their proliferation. Methoxsalen Corticosteroids Massaged in the scalp as a lotion, topical steroids are highly effective in relieving symptoms of seborrheic dermatitis including dandruff. However, relapse rates are high on discontinuation and prolonged use can produce adverse effects like atrophy, poor healing, purpura, etc. They sensitize the skin to sunlight which then induces erythema, inflammation and pigmentation. Methoxsalen is absorbed better, undergoes less first pass metabolism and is more effective than trioxsalen. Their plasma tЅ is short (~ 1 hr); sensitization of skin is maximal at 12 hours, but lasts for 8 hours or more. Pigmentation usually begins to appear after a few weeks; months are needed for satisfactory results. This therapy should be undertaken only under direct supervision of physician because longer exposure causes burning and blistering. Eyes, lips and other normally pigmented areas should be protected during exposure to sunlight. Topically applied emollients, keratolytics, antifungals afford variable symptomatic relief, but topical corticosteroids are the primary drugs used.
References:




