The investigator will Novartis Clinical Trial Protocol (Version 00) Confidential Page 34 Protocol No. Subjects should be seen for all visits on the designated day or as closely as possible to the original planned visit schedule (Table 6-1). If for any reason the subject is a screen failure, the subject may be re-screened. There is no restriction on the number of times a potential subject may be re-screened or on how much time must pass from the date of screen failure and the date of re-screening. For subjects who discontinue study treatment prematurely before the end of the treatment epoch for any reason other than withdrawal of informed consent or loss to follow-up procedures as described in Section 5. Other procedures Novartis Clinical Trial Protocol (Version 00) Confidential Page 35 Protocol No. Prepare the corresponding study medication packs and allow to adapt to room temperature for about 20 minutes before administration (dispense for home administrations, as required). Provide guidance to subjects for self-administration prior to the first treatment administration (Section 5. A Follow-up Epoch is not needed for subjects who complete the study up to Visit Week 52; completers have their last visit at Week 52. A urine pregnancy test is not required for a woman who is sterile or who is not of childbearing potential. A shipment to reference laboratories for analysis will be done by the central laboratory. An additional pre-dose sample should be withdrawn in case of early discontinuations at Visit F8 or if an unscheduled visit (U) is conducted Appendix 2 in Table 14-1. If the subject or caregiver is not able/confident to perform home administration, the subject will be allowed to return to the site for administration of the medication. Relevant medical history/current medical condition data includes data prior to signing of the informed consent and until the start of study treatment. The assay measures the production of interferon-gamma and presents it relative to a negative and a positive control sample (Manuel and Kumar 2008). Details on the collection, shipment of samples and reporting of results by the central laboratory are provided to investigators in the studyspecific laboratory manual. If the test result is indeterminate, the investigator may repeat the test once or may proceed directly to perform the work-up for the test result as per local procedures. Compliance to the planned site administration schedule is expected to be high since the study treatment will be administered in the presence of the investigator or study personnel at pre-defined visits. Crosschecks should be performed in case of home administrations (H) and empty medication boxes/outer packing/devices should be collected for compliance checks by field monitors. It is recommended that the same evaluator conduct the assessment throughout the study whenever possible. The explanations/descriptions of the points on the scale have been improved to ensure an appropriate differentiation between them. Pink to light red coloration; just detectable to mild thickening; predominantly fine scaling. Dull bright red, clearly distinguishable erythema; clearly distinguishable to moderate thickening; moderate scaling. Short Description Clear Almost clear Mild Moderate Novartis Clinical Trial Protocol (Version 00) 4 Severe Confidential Page 45 Protocol No. The following calculations will be done by Novartis: each reported percentage will be multiplied by its respective body region corresponding factor (head = 0. The head, trunk, upper limbs and lower limbs are assessed separately for erythema, thickening (plaque elevation, induration), and scaling (desquamation). The average degree of severity of each sign in each of the four body regions is assigned a score of 0-4. The area covered by lesions on each body region is estimated as a percentage of the total area of that particular body region. In the modified scale, the two "very severe" and "severe" have been condensed into a single category, "severe" and the explanations/descriptions of the points on the scale have been improved to ensure appropriate differentiation between the points. If necessary, based on medical history and/or symptoms, additional exams will be performed at the discretion of the investigator.
On her skin she has multiple, small (2-3 mm in diameter), firm, flesh-coloured papules on her face. Many of the papules have a central umbilicated depression, the surrounding skin is normal. The flesh-coloured umbilicated papules are caused by a cutaneous infection with a highly contagious poxvirus. Gently squeezing an individual lesion characteristically causes the extrusion of semi-solid white material (comprising the molluscum bodies). When adults present with multiple lesions, then underlying immune compromise should be suspected. This dual respiratory infection is not uncommon in patients from sub-Saharan Africa. After discharge from hospital she was seen in the dermatology out-patient clinic and had the molluscum lesions treated fortnightly with cryotherapy (liquid nitrogen). The molluscum slowly cleared with a combination of cryotherapy and immune reconstitution. Molluscum contagiosum is usually self-resolving in children and those with an intact immune system. Most attempts at treating molluscum lesions revolve around destructive/ irritant methods, such as with acid chemicals, cryotherapy and immunotherapy (topical imiquimod 5% cream daily). The lesions have slowly been increasing in size and number over the last two years and are mainly asymptomatic. Examination She has multiple hyperkeratotic flesh-coloured papules and nodules, mainly over the dorsi of her fingers and hands. Consequently, when the keratinocytes reach the epithelial surface, viral particles are released with the sloughed-off cells into the environment where they can survive for many months. Although cutaneous warts are not harmful in themselves they can cause a considerable amount of distress to patients both psychologically and socially. Patients frequently feel embarrassed by their warts and can often feel stigmatized by others. Cure rates of 60 per cent are reported in immunosuppressed patients after 6 months of treatment. Topical bleomycin has also been used with some success to treat recalcitrant warts in this group of patients. In addition she complains of a temperature, vomiting, diarrhoea, productive cough and painful red eyes. She has an extensive erythematous maculopapular eruption, which is particularly marked on her face, neck and trunk. Examination of her mouth reveals marked erythema with prominent white spots on her palate and buccal mucosae. Viral serology and oral fluid tests, sputum culture and skin biopsy were performed. A viral illness was suspected but a possible reaction to amoxicillin was also considered. Her two children had recently had a viral illness that was subsequently confirmed as measles. Patients frequently experience a prodrome of fever and malaise with photophobia and conjunctivitis. The cutaneous eruption usually appears within days of the onset of symptoms, first appearing behind the ears and then spreading caudally. The rash is erythematous and mainly macular but can develop papules, which may coalesce and blister. This patient developed a chest infection as a complication of her measles; sputum culture grew Haemophilus influenzae.
Diseases
Simultaneously, we must drastically reduce the availability of these drugs in the United States. Increased availability increases the opportunity for individuals to initiate drug use, and the path from first use to chronic usecanbebrutallyshort,particularlyforpotentandhighlyaddictivedrugslikeopioids. Early intervention through informational media campaigns and community support mechanisms can alter the trajectory of young people in a positive direction and increase protective factors while reducing risk factors. Studies show that addiction is a disease that can be prevented and treated through soundpublichealthinterventions. Combining two or more evidence-based elements in a comprehensive prevention program is more effectivethanasingleactivityalone. The Administration is already addressing the unmetneedofacompellinganduniversalinformationcampaigntoeducateourNationonthedrug-relatedvulnerabilitiesofouryouthandotherat-riskpopulations. Thismajoreffort will reach audiences not targeted by RxAwareness by addressing topics this major effort will reach audiences not targeted by RxAwareness by addressing topics related to the speed at which chronic substanceusecandevelop,thedrasticmeasuresthosesufferingfromsubstanceusedisorderwilltaketo feedtheiraddiction,andtheneedtoreducethestigmaassociatedwithaddictionandtreatmentfor substance abuse. Prevention messages targeting youth are being disseminated through social media and other popular platforms utilized by young people. As the campaign moves forward, its messaging will use data analytics to determine appropriate messaging based on target population and substance, and will employ communication and marketing methods such as market segmentation, demographic data on users, and multiple formats and languages for individuals with disabilities and individuals with limited English proficiency. The campaign will be augmented by science-based primary prevention across multiple sectorsusingapproachesthateffectivelyengagestudents,parents,schools,healthcaresystems,faith communities,socialserviceorganizations,andothersectors,inthedevelopmentandimplementation ofcommunityandschool-basedpreventioninitiatives. Addressing Safe Prescribing Practices There is a compelling need for additional research on, and the implementation of, evidence-based guidelines for the dosages and duration of prescription opioid treatment for injuries and post-surgical pain management. This is particularly important for patients with a history of substance abuse oratelevatedriskfordrugmisuse. Moreover,clinicalguidelinesandbestpracticesshouldbestandardizedinprovidertraining programs and continuing medical education programs for those who prescribe and administer opioids suchassurgeons,emergencymedicineproviders,andemergencymedicaltechnicians. Underpinning these initiatives is the awareness that patients with chronic pain must receive thebestmedicalcareavailabletoamelioratetheirsufferingandenablethemtoenjoythebestpossible qualityoflife,whilesimultaneouslyreducingthelikelihoodthatpatientswillbecomeaddictedtothese treatment regimens. Enhancing Research and the Development of Evidence-Based Prevention Programs TheNationalAcademiesofSciences,Engineering,andMedicineoutlinethreecategoriesofprevention intervention:universal,selective,andindicated. Weknowthateverydollarweinvestinresearch-basedsubstanceabusepreventionprograms has the potential to save much more in treatment and criminal justice system costs and enhance the overall quality of life for communities and their citizens. There is a need to improve the availability of treatment while concurrently enhancing the quality of that treatment. Research shows that treatment is most effective when it addresses addiction as a chronic condition requiring continuing services and support structures over an extendedperiodoftime. Thiscanbeaccomplishedwithongoingoutpatientservicesprovidedthrough opioidtreatment,ormoreintensiveinitialservicessuchasdetoxificationandresidentialtreatment,followed by continued care and recovery support in the community. Every individual needs an assessment and individualized treatment plan to address their needs as they relate to opioid and other substances use disorders. First, a proactive response to overdoses to ensure that the patient can enter into a treatment program designed to meet hisorherindividualneeds. Expandingtreatment infrastructure will enable us to increase the initial treatment for the vast majority of people who requiretreatmentbutareunableorunwillingtoobtainit. Third,examiningwaystoexpandandencouragingtheexpansionoftreatmentinsurancewhilereducingreimbursementbarrierstoencouragethose on the margins of accepting treatment to make the positive decision to begin a treatment regimen. Addressingtheseandotherchallengeswillrequireacomprehensivemulti-year strategytoeducate the public and policymakers, reducestigma and misunderstandingof addiction, better integrate substance abuse screening and treatment into mainstream health care, build and stabilize the addiction treatment workforce, increase access to treatment, and foster more effective approaches to care for substance use disorders. Wewillbegintoincrease public awareness of the importance of rescue breathing in the event of an opioid overdose in those caseswhennaloxoneisnotavailableasacriticallive-savingmeasure. Moreover,wemustdomoreto ensure that the reversal of a potentially fatal overdose is not just another event in a long and protracted strugglewithanaddictiontodangerousdrugs,butratherthefirstimportantsteptowardeffectivetreatment and the path to sustained recovery. Enhancing Evidence-Based Addiction Treatment Wemustensurethathealthcareprovidersscreenforsubstanceusedisordersandknowhowtoappropriately counsel or refer patients they encounter with such a disorder. Additionally, identifying and treating pediatric patients with early substance use disorder can prevent their transition tolongerandmoreseveredruguse,potentiallysavingtheirlives. Therefore,wemustscaleupadolescent addiction screening and treatment in pediatrician and family medicine settings. Eliminating Barriers to Treatment Availability Individuals with substance use disorders, including opioid addiction, should have access to evidence-based treatment.
Older patients and patients with more severe medical problems were less likely to complete the questionnaire fully compared with younger and healthier patients (31). Reproducibility was measured by the coefficient of repeatability according to the method of Bland and Altman, and found to be acceptable (21,35). Higher correlations to measures of pain and function than to psychological measures have been established (21,29,32,39,40). According to Murray et al, the minimum clinically important difference can be expected Practical Application How to obtain. According to the updated version, "Each of the 12 questions is scored in the same way with the score decreasing as the reported symptoms increase. If 2 answers are indicated for 1 question, the worst response should be used for calculation of scores. The authors found that scores of 38 and 33 were associated with patient satisfaction at 12 and 24 months, respectively. However, the threshold varied according to preoperative scores and to body mass index limiting the clinical use of the threshold value. Nilsdotter and Bremander maximum disability) and is scored as the sum of all questions. The index was modified in 1991 when a question for sexual activity was included if appropriate, resulting in a maximum score of 28. A score over 11-12 points after appropriate treatment is suggested to indicate surgery (45). Some training may be needed for use of the interview-based questionnaire to reach interobserver reproducibility (43). Questions have also been raised about the lack of items concerning activities requiring a large angle of hip flexion, as well as aids and medication; this information has to be addressed by other means. The questionnaire is easy to use due to self-administered distribution, and it only takes a few minutes to complete. A single administration will not provide much information on an individual, but repeated administrations might give some information Research usability. Developed in France in the early 1980s as an interview format to use in clinical drug trials, the instrument is available currently in several versions: interview based (43), self-administered (46), and in modified versions due to changed scoring and wording (45). There are 11 items; the score ranges from 0 (no pain or no disability) to 24 (maximum pain or Psychometric Information Method of development. Rasch analysis has been applied later in validity studies and has questioned the psychometric properties of the questionnaire (47). Two of 10 patients needed some explanation to fill out the questionnaire in a French study using the Lequesne Index of Severity for Osteoarthritis of the Knee (49). For interrater reliability, the interview-based questionnaire had a mean deviation of 0. There are versions for the lower extremity, for global sports/knee, and for the foot and ankle (53). Critical Appraisal of Overall Value to the Rheumatology Community Caveats and cautions. Psychometric evaluations do not support the interpretation of scores on an individual level.
Piroxicam pharmacokinetics: recent clinical results relating kinetics and plasma levels to age, sex, and adverse effects. Pharmacokinetics of piroxicam, a new nonsteroidal anti-inflammatory agent, under fasting and postprandial states in man. Relative bioavailability of two oral formulations of piroxicam 20 mg: a single-dose, randomized-sequence, open-label, two-period crossover comparison in healthy Mexican adult volunteers. The pharmacokinetics of piroxicam in elderly persons with and without renal impairment. Renal effects of ibuprofen, piroxicam, and sulindac in patients with asymptomatic renal failure: a prospective, randomized, crossover comparison. Inhibition of mineralocorticoid receptor is a renoprotective effect of 3-hydroxy3-methylglutaryl coenzyme A reductase inhibitor pitavastatin. Comparative efficacy of pitavastatin and simvastatin in high-risk patients: a randomized controlled trial. Pharmacology of 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors (statins), including rosuvastatin and pitavastatin. Place of pitavastatin in the statin armamentarium: promising evidence for a role in diabetes mellitus. Co-administration of ezetimibe enhances proteinuria-lowering effects of pitavastatin in chronic kidney disease patients partly via a cholesterol-independent manner. Effect of pitavastatin on urinary liver-type fatty acid-binding protein levels in patients with nondiabetic mild chronic kidney disease. Effect of pitavastatin on urinary liver-type fatty acid-binding protein levels in patients with early diabetic nephropathy. Poolsup N, Suksomboon N, Wongyaowarat K, Rungkanchananon B, Niyomrat P, Kongsuwan S. Meta-analysis of the comparative efficacy and safety of pitavastatin in patients with dyslipidemia. Clinical efficacy of pitavastatin, a new 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor, in patients with hyperlipidemia: dose-finding study using the double-blind, three-group parallel comparison. Effect of low-dose (1 mg/day) pitavastatin on left ventricular diastolic function and albuminuria in patients with hyperlipidemia. Identification of prognostic factors for plerixafor-based hematopoietic stem cell mobilization. Plerixafor dosing and administration in a patient with dialysis-dependent renal failure. Efficacy of pre-emptively use plerixafor in patients mobilizing poorly after chemomobilization: a single centre experience. Plerixafor: a review of its use in stem cell mobilization in patients with lymphoma or multiple myeloma. A pharmacokinetic study of plerixafor in subjects with varying degrees of renal function. Plerixafor (Mozobil) for stem cell mobilization in patients with multiple myeloma previously treated with lenalidomide. Pharmacokinetics and pharmacodynamics of plerixafor in patients with non Hodgkin lymphoma and multiple myeloma. Efficacy and cost-benefit analysis of risk-adaptive use of plerixafor for autologous hematopoietic progenitor cell mobilization. Antimicrobial treatment and clinical outcomes of carbapenem-resistant Acinetobacter baumannii ventilator-associated pneumonia. The impact of polymyxin B dosage on in-hospital mortality of patients treated with this antibiotic. The use of intravenous and aerosolized polymyxin B for the treatment of infections in critically ill patients: a review of the recent literature. Polymyxins: pharmacology, pharmacokinetics, pharmacodynamics, and clinical applications. Polymyxin B in chronic pyelonephritis: observations on the safety of the drug and on its influence on the renal function. Polymyxin B versus other antimicrobials for the treatment of Pseudomonas aeruginosa bacteraemia. Pharmacokinetics of polymyxin B1 in patients with multidrug-resistant gram-negative bacterial infections.
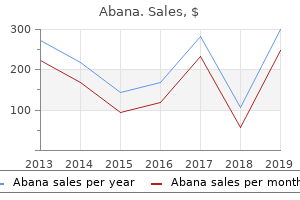
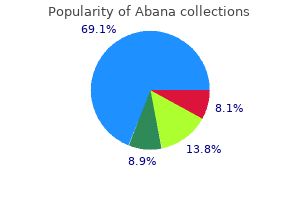
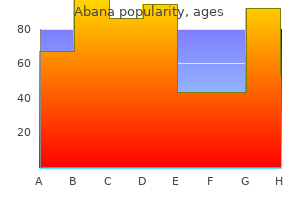
Maranta (Arrowroot). Abana.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96306
Dose-escalation study of pemetrexed in combination with carboplatin followed by pemetrexed maintenance therapy for advanced non-small cell lung cancer. A phase I and pharmacokinetic study of pemetrexed plus irinotecan in patients with advanced solid malignancies. Pemetrexed plus cisplatin/carboplatin in previously treated locally advanced or metastatic non-small cell lung cancer patients. Data not available; interindividual drug clearance varies widely, and available clinical data presently are not sufficient to recommend adequate and safe dose amounts in patients with impaired excretory kidney function. High-dose versus low-dose d-penicillamine in early diffuse systemic sclerosis: analysis of a two-year, double-blind, randomized, controlled clinical trial. Renal ultrastructure, renal function, and parameters of lead toxicity in workers with different periods of lead exposure. Predictors and outcomes of scleroderma renal crisis: the high-dose versus low-dose d-penicillamine in early diffuse systemic sclerosis trial. Fatal renal vasculitis and minimal change glomerulonephritis complicating treatment with penicillamine: report of two cases. A disorder of copper metabolism treated with penicillamine in a patient with primary biliary cirrhosis and renal tubular acidosis. Effects of long-term aurothiomalate and d-penicillamine treatments on renal function and urinary excretion of prostanoids in patients with rheumatoid arthritis. Progressive Proliferative glomerulonephritis in a patient with rheumatoid arthritis treated with d-penicillamine. Maturation of renal organic acid transport in vivo: substrate stimulation by penicillin. The bactericidal action of penicillin in vivo: the participation of the host, and the slow recovery of the surviving organisms. The interaction and transport of b-lactam antibiotics with the cloned rat renal organic anion transporter 1. Optimal dosing of penicillin G in the third trimester of pregnancy for prophylaxis against group B Streptococcus. Drug inhibition of penicillin tubular secretion: concordance between in vitro and clinical findings. Neurotoxicity of benzylpenicillin in experimental renal failure and Enterobacter cloacae meningitis. Neurotoxicity and "massive" intravenous therapy with penicillin: a study of possible predisposing factors. Organic anion transporter 3 (Oat3/Slc22a8) knockout mice exhibit altered clearance and distribution of penicillin G. Clinical pharmacokinetics of continuous intravenous administration of penicillins. Penicillin convulsions: the convulsive effects of penicillin applied to the cerebral cortex of monkey and man. Combined carbon haemoperfusion and haemodialysis in treatment of penicillin intoxication. Administer a full loading dose followed by one-half of the loading dose every 4 h. Administer a full loading dose followed by one-half of the loading dose every 8 h. Pharmacokinetics of intravenous pentamidine in patients with normal renal function or receiving hemodialysis. Inhaled or reduced-dose pentamidine for Pneumocystis carinii pneumonia: a pilot study. Nephrotoxicity and hyperkalemia in patients with acquired immunodeficiency syndrome treated with pentamidine. Plasma pentamidine concentrations vary between individuals with Pneumocystis carinii pneumonia and the drug is actively secreted by the kidney.
Fujimoto K, Hosokawa Y, Tomioka A et al: Variations of transition zone volume and transition zone index after transurethral needle ablation for symptomatic benign prostatic hyperplasia. Minardi D, Garofalo F, Yehia M et al: Pressure-flow studies in men with benign prostatic hypertrophy before and after treatment with transurethral needle ablation. Namiki K, Shiozawa H, Tsuzuki M et al: Efficacy of transurethral needle ablation of the prostate for the treatment of benign prostatic hyperplasia. Daehlin L, Gustavsen A, Nilsen A et al: Transurethral needle ablation for treatment of lower urinary tract symptoms associated with benign prostatic hyperplasia: outcome after 1 year. Braun M, Zumbe J, Korte D et al: Transurethral needle ablation of the prostate: an alternative minimally invasive therapeutic concept in the treatment of benign prostate hyperplasia. Minardi D, Galosi A, Recchioni A et al: Diagnostic accuracy of percent free prostate-specific antigen in prostatic pathology and its usefulness in monitoring prostatic cancer patients. Gravas S, Laguna M, de la Rosette J: Efficacy and safety of intraprostatic temperature-controlled microwave thermotherapy in patients with benign prostatic hyperplasia: results of a prospective, open-label, single-center study with 1-year follow-up. Dahlstrand C, Walden M, Geirsson G: Transurethral microwave thermotherapy versus transurethral resection for symptomatic benign prostatic obstruction: a prospective randomized study with 2-year follow-up. Floratos D, Kiemeney L, Rossi C et al: Long-term followup of randomized transurethral microwave thermotherapy versus transurethral prostatic resection study. Ohigashi T, Nakamura K, Nakashima J et al: Long-term results of three different minimally invasive therapies for lower urinary tract symptoms due to benign prostatic hyperplasia: comparison at a single institute. Laguna M, Kiemeney L, Debruyne F et al: Baseline prostatic specific antigen does not predict the outcome of high energy transurethral microwave thermotherapy. Vesely S, Knutson T, Dicuio M et al: Transurethral microwave thermotherapy: clinical results after 11 years of use. Djavan B, Seitz C, Roehrborn C et al: Targeted transurethral microwave thermotherapy versus alpha-blockade in benign prostatic hyperplasia: outcomes at 18 months. Thalmann G, Mattei A, Treuthardt C et al: Transurethral microwave therapy in 200 patients with a minimum followup of 2 years: urodynamic and clinical results. Osman Y, Wadie B, El-Diasty T et al: High-energy transurethral microwave thermotherapy: symptomatic vs urodynamic success. Miller P, Kastner C, Ramsey E et al: Cooled thermotherapy for the treatment of benign prostatic hyperplasia: durability of results obtained with the Targis System. Bock D, Price D, Fay R: Prolieve transurethral microwave thermodilation versus finasteride: results of a multicenter, randomized trial in symptomatic patients with benign prostatic hyperplasia. Semmens J, Wisniewski Z, Bass A et al: Trends in repeat prostatectomy after surgery for benign prostate disease: application of record linkage to healthcare outcomes. Bach T, Herrmann T, Ganzer R et al: RevoLix vaporesection of the prostate: initial results of 54 patients with a 1-year follow-up. Hettiarachchi J, Samadi A, Konno S et al: Holmium laser enucleation for large (greater than 100 mL) prostate glands. Kuntz R, Lehrich K: Transurethral holmium laser enucleation versus transvesical open enucleation for prostate adenoma greater than 100 gm. Tan A, Gilling P, Kennett K et al: A randomized trial comparing holmium laser enucleation of the prostate with transurethral resection of the prostate for the treatment of bladder outlet obstruction secondary to benign prostatic hyperplasia in large glands (40 to 200 grams). Montorsi F, Naspro R, Salonia A et al: Holmium laser enucleation versus transurethral resection of the prostate: results from a 2-center, prospective, randomized trial in patients with obstructive benign prostatic hyperplasia. Briganti A, Naspro R, Gallina A et al: Impact on sexual function of holmium laser enucleation versus transurethral resection of the prostate: results of a prospective, 2-center, randomized trial. Kuntz R, Ahyai S, Lehrich K et al: Transurethral holmium laser enucleation of the prostate versus transurethral electrocautery resection of the prostate: a randomized prospective trial in 200 patients. Aho T, Gilling P, Kennett K et al: Holmium laser bladder neck incision versus holmium enucleation of the prostate as outpatient procedures for prostates less than 40 grams: a randomized trial. Malek R, Kuntzman R, Barrett D: Photoselective potassium-titanyl-phosphate laser vaporization of the benign obstructive prostate: observations on long-term outcomes. Monoski M, Gonzalez R, Sandhu J et al: Urodynamic predictors of outcomes with photoselective laser vaporization prostatectomy in patients with benign prostatic hyperplasia and preoperative retention. The A, Malloy T, Stein B et al: Impact of prostate-specific antigen level and prostate volume as predictors of efficacy in photoselective vaporization prostatectomy: analysis and results of an ongoing prospective multicentre study at 3 years. Neill M, Gilling P, Kennett K et al: Randomized trial comparing holmium laser enucleation of prostate with plasmakinetic enucleation of prostate for treatment of benign prostatic hyperplasia.

Tumors arising in minor salivary glands (mucus-secreting glands in the lining membrane of the upper aerodigestive tract) are staged according to the anatomic site of origin. Primary tumors of the parotid constitute the largest proportion of salivary gland tumors. Sublingual primary cancers are rare and may be difficult to distinguish with certainty from minor salivary gland primary tumors of the anterior floor of the mouth. Major Salivary Glands 79 In order to view this proof accurately, the Overprint Preview Option must be set to Always in Acrobat Professional or Adobe Reader. Regional lymphatic spread from salivary gland cancer is less common than from head and neck mucosal squamous cancers and varies according to the histology and size of the primary tumor. Low-grade tumors rarely metastasize to regional nodes, whereas the risk of regional spread is substantially higher from high-grade cancers. Regional dissemination tends to be orderly, progressing from intraglandular to adjacent (periparotid, submandibular) nodes, then to upper and midjugular nodes, apex of the posterior triangle (level Va) nodes, and occasionally to retropharyngeal nodes. For pathologic reporting (pN), histologic examination of a selective neck dissection will ordinarily include six or more lymph nodes and a radical or modified radical neck dissection will ordinarily include ten or more lymph nodes. Negative pathologic evaluation of a lesser number of nodes still mandates a pN0 designation. T4a T4b Moderately advanced disease Tumor invades skin, mandible, ear canal, and/or facial nerve Very advanced disease Tumor invades skull base and/or pterygoid plates and/or encases carotid artery *Note: Extraparenchymal extension is clinical or macroscopic evidence of invasion of soft tissues. The assessment of primary salivary gland tumors includes a pertinent history (pain, trismus, etc. The soft tissues of the neck from the skull base to the hyoid bone must be studied, with the lower neck included whenever lymph node metastases are suspected. Images of the intratemporal facial nerve are critical to the identification of perineural spread of tumor in this area. Cancers of the submandibular and sublingual salivary glands merit cross-sectional imaging. The surgical pathology report and all other available data should be used to assign a pathologic classification to those patients who have resection of the cancer. Minor salivary gland tumors of the palate: Clinical and pathologic correlates of outcome. Prognostic factors in mucoepidermoid carcinomas of major salivary glands: a clinicopathologic and flow cytometric study. National Cancer Data Base report on cancer of the head and neck: acinic cell carcinoma. Multivariate survival analysis of 128 cases of oral cavity minor salivary gland carcinomas. Malignant parotid tumors in 110 consecutive patients: treatment results and prognosis. Long-term follow-up of over 1, 000 patients with salivary gland tumours treated in a single centre. Prognostic factors for long-term results of the treatment of patients with malignant submandibular gland tumors. Microscopic evidence alone does not constitute extraparenchymal extension for classification purposes. Lymph-vascular Invasion Not Present (absent)/Not Identified Lymph-vascular Invasion Present/Identified Not Applicable Unknown/Indeterminate Residual Tumor (R) the absence or presence of residual tumor after treatment. Both the histologic diagnosis and the age of the patient are of such importance in the behavior and prognosis of thyroid cancer that these factors are included in this staging system. The thyroid gland ordinarily is composed of a right and a left lobe lying adjacent and lateral to the upper trachea and esophagus. An isthmus connects the two lobes, and in some cases a pyramidal lobe is present extending cephalad anterior to the thyroid cartilage. Regional lymph node spread from thyroid cancer is common but of less prognostic significance in patients with well-differentiated tumors (papillary, follicular) than in medullary cancers. The adverse prognostic influence of lymph node metastasis in patients with differentiated carcinomas is observed, only in the older age group. Metastases secondarily involve the mid- and lower jugular, the supraclavicular, and (much less commonly) the upper deep jugular and spinal accessory lymph nodes. Retropharyngeal nodal metastasis may be seen, usually in the presence of exten- sive lateral cervical metastasis. The lymph node metastasis should also be described according to the level of the neck that is involved.
The 17 sites have administered over 5,000 maternal depression screens for families enrolled in the program. Data are being analyzed to determine the positive screen rate and disposition of the positive screens. The grant supports collaborative quality improvement projects in three high need counties (Erie, Niagara and Nassau) to improve maternal depression screening and follow-up as well as developmental screening and followup for young children. Kuo, Associate Professor and Division Chief for General Pediatrics at the University at Buffalo, the Erie/Niagara team organized a learning collaborative and designed a referral algorithm in 2017 for families with young children to use in five local pediatric practices. As part of the initiative, participating counties assessed how pregnant women using opioids would negotiate the health care and support systems in their respective counties. Drafts of plans of safe care and decision trees for hospital staff have been developed. The participating counties recently began piloting implementation of plans of safe care and provided initial feedback to the state to inform revisions of to the plans of safe care and decision trees. The data analysis planning team, comprised of Title V staff and other state agency representatives, has been addressing questions and concerns that arise throughout the study period. The application continues to reflect ongoing efforts to address these priority public health issues to achieve selected targets. Racial disparities in maternal deaths are persistent the statewide 3-year rolling Black to White mortality ratio ranged from a high of 4. The majority of women who died of pregnancy-related causes were affected by risk factors including hematologic issues (26%), pulmonary conditions (23%), hypertension (19%), endocrine issues (19%), cardiac problems (18%), and psychiatric disorders (17%). Improving birth outcomes for mothers and infants requires a life course perspective. This priority is closely linked to other state priorities including: Priority #2: Reduce infant mortality and morbidity Priority #3: Support and enhance social-emotional development and relationships for children and adolescents and all four Life Course priorities (#5-8). Strategies to address maternal mortality and morbidity are largely inextricable from those to address infant mortality and morbidity thus, the strategies described for Domain 1 and Domain 2 should be considered part of the continuum of public health activities to improve both maternal and infant maternal mortality and morbidity. Efforts implemented to date related to these initiatives were reviewed in the Annual Report section of this application. The Maternal Mortality Review Initiative will continue to conduct a complete assessment of the causes of death, factors leading to death, preventability, and opportunities for intervention. Title V plans to continue this review process while aiming to release data reports every two years to support prevention and clinical improvement strategies with partners. Work also continues Centering Pregnancy to improve access to and quality of prenatal care. Title V staff helped inform the selection of the high priority areas for the Centering Pregnancy project and will help promote the benefits of both initiatives. A focus in the coming year will be to expand programs in clinics with already established Centering Pregnancy programs by June 2019 and then focus on clinics seeking to establish new programs. As discussed in the annual report section of this Domain, under the pilot, doula services are available for any Medicaid-eligible pregnant woman in fee-for-service or Medicaid Managed Care in specific geographic locations. Phase 2 of the project will include selected zip codes in Kings County once provider capacity has been achieved. In addition to improving prenatal care in high need communities, it is imperative to ensure quality inpatient perinatal care. Hospitals are designated as one of four levels of perinatal care based upon the types of patients that are treated, sub-specialty consultation available, qualifications of staff, types of equipment available and volume of high-risk perinatal patients treated. The concentration of high-risk patients makes it possible to maintain the substantial expertise and expense required for the care of high-risk women and newborns and attending level sub-specialty consultation in maternal-fetal medicine and neonatology.
The Wellbeing Assessment must be completed before you or your covered spouse/domestic partner can earn the incentive. Make better informed healthcare choices: Receive personalized recommendations based on your past care and innetwork options, along with helpful tips about ways to save money and find high-quality care. Participate in online evidence-based therapy to address stress, depression, anxiety and other behavioral health concerns. Register for Castlight on or before the Open Enrollment deadline of November 18, 2016, and receive a $50 deposit to your Health Reimbursement Account or Health Savings Account on January 13, 2017. If you miss the deadline, you can still receive the account credit if you register by July 31, 2017. Manage Your Health through Doctor On Demand You can access a national network of board-certified doctors and licensed professionals all day, every day, at very affordable rates. In addition, behavioral health counseling is available by appointment with licensed professionals. Use Doctor On Demand for non-emergency care when you need to see a physician and do not need to use an emergency room. In the event of a true medical emergency (such as shortness of breath, chest pains or broken bones) dial 911 or go to your local emergency room. You can also download the Doctor On Demand app to your iPhone or iPad (App Store), or Android device (Google Play). These walk-in medical centers are available across the United States, with on-staff nurse practitioners and physician assistants who specialize in family care (for patients who are 18 months or older). After that time, the excess amounts are subject to both income taxes and an excise tax. You may report the event in the online benefits system from work through MyReward (MySource > MyReward > Log on to MyReward > Proceed to My Personal Total Reward Data > MyBenefit Solutions > Life Events), from home at mybenefits. The consistency rule means that you can only change benefits that are directly linked to the qualified change you experience. For example, if you have or adopt a child you can add a new dependent to your coverage. However, you cannot change your medical plan election when you have or adopt a child since the life event does not have a direct impact on your coverage choice. The following table lists some common life event changes and the types of benefit adjustments you may request in each situation. You may cancel coverage for your child if your spouse, former spouse or other individual provides coverage for the child because he or she is required to do so due to a judgment, decree or order resulting from a divorce, legal separation, annulment or change in legal custody. If you, your spouse/domestic partner or dependent becomes entitled to coverage under Medicare or Medicaid (other than solely under the program for distribution of pediatric vaccines), you may elect to cancel coverage for the entitled person. If you cancel your coverage, coverage for your spouse/domestic partner and dependent(s) will end as well. You and your dependents are not eligible for Special Enrollment Rights, however, if you lost coverage because you did not pay premiums on time, voluntarily dropped coverage or are guilty of fraud. Note: You may add coverage for yourself in order to cover an eligible dependent who loses coverage under these circumstances. If you gain a new dependent, you may add coverage for yourself and your dependents (if you are not already covered) or, if you are already covered, you may add coverage for the new dependent and other eligible family members. See "How to Report a Qualified Life Event Change" on page 20 for more information. Depending on the covered individual (you, your spouse, your domestic partner or your other dependent), one of the plans will be designated as the primary coverage and will be responsible for paying benefits first; the other plan will be considered secondary (which means it will only pay benefits after the primary plan has paid, and up to a maximum amount of the actual charge). This means that the plan of the parent with the earlier birthday in the calendar year (using month and date only, not year) will be considered primary. Medicare generally pays second: - - - When the domestic partner is entitled to Medicare on the basis of disability and is covered by a large group health plan on the basis of his/her own current employment status or the status of a family member For the 30-month coordination period when the domestic partner is eligible on the basis of end-stage renal disease, and is covered by a group health plan on any basis When the domestic partner is entitled to Medicare on the basis of age and has group health plan coverage on the basis of his/her own current employment status.
References:




