Indolent disseminated disease is associated with fever, cough, weight loss, chest pain, skin lesions, and osteolytic lesions. In severe cases, initiate amphotericin B therapy instead, and follow treatment response with serology. At presentation in most cases, disease has already spread to bone marrow, liver, spleen, skin, or bone. Skin lesions develop in two-thirds of pts; these erythematous papules can have central necrosis. Blood cultures are positive in 59% of cases; in contrast, blood cultures are rarely positive in aspergillosis or mucormycosis. For extracutaneous disease, itraconazole (200 mg bid) can be given, but amphotericin B is more effective. In contrast to most fungi, Pneumocystis lacks ergosterol and is not susceptible to antifungal drugs that inhibit ergosterol synthesis. Both airborne transmission and person-toperson transmission have been demonstrated. Pathogenesis Defects in cellular and humoral immunity predispose to Pneumocystis pneumonia. Other persons at risk include those receiving immunosuppressive therapy (particularly glucocorticoids) for cancer, organ transplantation, or other disorders; malnourished premature infants; and children with primary immunodeficiency disorders. The organisms are inhaled and attach tightly to type I cells in alveoli, although they remain extracellular. With immunosuppression, the organisms propagate and fill the alveoli, resulting in increased alveolar-capillary permeability and damage to alveolar type I cells. Severe disease may cause interstitial edema, fibrosis, and hyaline membrane formation. Clinical and Laboratory Features Pts develop dyspnea, fever, and nonproductive cough. On physical examination, pts are found to have tachypnea, tachycardia, and cyanosis, but findings on pulmonary examination are often unremarkable. Reduced arterial oxygen pressure, increased alveolar-arterial oxygen gradient, and respiratory alkalosis are evident. Methenamine silver, toluidine blue, and cresyl echt violet selectively stain the wall of Pneumocystis cysts. Course and Prognosis Therapy is most effective if started early, before there is extensive alveolar damage. Secondary prophylaxis is indicated for all pts who have recovered from pneumocystosis. After progressively consuming and degrading intracellular proteins (principally hemoglobin), trophozoites become schizonts. After ingestion by female anopheline mosquitoes during a blood meal, male and female gametocytes mature in the mosquito midgut to begin a new cycle of transmission. Sequestration is central to the pathogenesis of falciparum malaria but is not evident in the other three "benign" forms. With repeated exposure to malaria, a specific immune response develops and limits the degree of parasitemia. Over time, pts are rendered immune to disease but remain susceptible to infection. Genetic disorders more common in endemic areas protect against death from malaria. Cerebral malaria: coma, obtundation, delirium, encephalopathy without focal neurologic signs. Premature labor, stillbirths, delivery of low-birth-weight infants, and fetal distress are common.
Academic and governmental research laboratories, as well as the research efforts of suppliers (new processing methods, packaging, and ingredients), have supplied much of the new technology used by the food industry for product innovation, leading to its economic growth [12]. Although the success of any new product from a single company can be (and always will be) problematic, overall the industry-wide new-product efforts have been highly successful. The introduction of waves of new products with increasing consumer utility, in turn, gave the food industry greater influence over what Americans ate, and do eat [7]. Unfortunately, this great industry accomplishment is marred today by the association of its products and marketing methods with the obesity pandemic. In fact, even today, much of public policy (agricultural, industrial, and economic) still greatly favors the growth of the American processed-food industry, despite the fact that many of the products resulting from the current industrial policies have potentially serious negative health implications for Americans. Commercial interests largely set our table and often promote an overeating culture. There is probably no one answer, but many answers, to this question, depending on the individual and his or her particular lifestyle. We must acknowledge that to date our efforts to control or reduce the obesity pandemic at both the individual and the population levels have been largely futile. This lack of success, at either the individual or the societal level, requires new thinking, new insights, and new approaches. With this new thinking, the role of "commercial sectors" in creating a societal environment that fosters population-wide obesity needs to be more aggressively addressed. Any solution to the obesity pandemic requires "coordinated policy actions" on both the demand and the supply sides of the food supply chain. In crafting future public policies, we can learn much about what will work and what will not from the governmental policies for other orally used substances- tobacco, alcohol, and drugs-which at one time were completely unfettered in their commercial activities, causing socially unacceptable human suffering and harm and incurring high related societal costs. A modern industrial nation such as the United States requires a well-functioning and economically sound commercial food supply chain. Changes are needed in the manner in which commercial interests supply our food while still retaining their necessary function of feeding us without motivating overconsumption. Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 2005, to the Secretary of Agriculture and the Secretary of Health and Human Services. Further motivating this muchneeded reevaluation are projections of future human suffering and the economic costs from the unchecked obesity pandemic. Unless solutions are found, future human suffering will be staggering and the related medical costs astronomical. Can any nation afford or be willing to bear such suffering for the sake of the unfettered economic interests of one of its commercial sectors From our agricultural lands to our mouths, our daily food is shaped, controlled, and marketed by commercial interests. American Agriculture in the Twentieth Century: How It Flourished and What it Cost. Annual medical spending attributable to obesity: Payer- and service-specific estimates. In most places there is a wide array of transportation options, but simple behavioral economics may cause people to favor certain modes of transportation over others. In places where governments have invested heavily in public transit and in building cities and towns that are conducive to walking and bicycling, obesity rates are lower than in places that are more car dependent. In contrast, the percentage of trips taken by private vehicles has gradually risen and now stands between 80% and 90% of total trips. Similar trends have been observed in many other industrialized nations including Great Britain11 and Finland. In particular, European countries such as Denmark, the Netherlands, and Germany have high modal shares for bike trips, at 15%, 25%, and 9%, respectively (Figure 38. Pucher and Buehler14 noted that during the 1950s through the 1970s these countries experienced dramatic declines in modal shares of walking and bicycling and became more and more dependent on cars. During the mid1970s, however, their governments made a concerted shift in transportation and land use policies to favor active transportation. Not surprisingly, in these nations obesity rates are far lower than in countries that are more reliant on personal automobiles.
Previously, the candidate gene approach had limited success in identifying loci that were robustly associated with obesityrelated traits. This was likely due to insufficient knowledge of the biology of energy metabolism, an often incomplete survey of the genetic variation in the candidate gene, and generally small study populations (N < 1000), resulting in low power to detect the small effect sizes that are anticipated for common obesity. More recently, an increasing number of candidate gene studies have examined associations in larger samples (N > 5000), sometimes followed by a meta-analysis of all available evidence. The most widely studied variants encode the amino acid changes V103I (rs2229616) and I251L. Meta-analyses of all available data have shown that carriers of the 103I-encoding allele had a 21% lower risk of obesity than V103V homozygotes,11 whereas carriers of the 251L-encoding allele had a 48% reduced risk of obesity when compared with I251I homozygotes. The 64R-encoding allele is more common in East Asians (frequency 18%) than in Europeans (7. Recently, a metaanalysis of all available data could not confirm an association with obesity for any of the three variants. In addition to being sufficiently powered to identify common variants for obesity-related traits, large-scale candidate gene studies are also capable of refuting associations between variants in candidate genes and obesity-related traits. The Advances in the field of obesity genetics have largely been driven by technological developments, with improved technology allowing genotyping of many variants in many individuals simultaneously and in little time. These improvements have facilitated the development of catalogs with detailed information on human genetic variation, such as the Human Genome Project,58 the International HapMap Project,59 and, more recently, the 1000 Genomes Project. However, studies in children and in individuals of East Asian and African descent are beginning to be reported as well. Results files of independent studies are subsequently meta-analyzed to obtain summary statistics that represent the association in all studies combined. Confirmed loci are often further examined in a third stage, in which associations with related traits or diseases are assessed. For each trait, summary statistics are shown as provided in the largest study to date (Speliotes et al. Secondary analyses showed that associations were significantly more pronounced in women than in men for 7 of the 14 loci. Given the results described here, it seems likely that the true effects of established loci are larger in subgroups of the population with lifestyles that favor penetrance of their genetic predisposition. However, most established loci contain multiple genes, and deep-sequencing and fine-mapping efforts, as well as animal studies, are warranted to identify causal variants and genes within these loci. Only then can physiologists and biochemists start exploring their functional relevance for obesity susceptibility. In mice, Fto was shown to be ubiquitously expressed, including in the hypothalamus. So far, follow-up studies in humans have shown associations with appetite regulation and energy intake but not energy expenditure. Identifying currently unanticipated loci, as well as causal 116 Handbook of Obesity variants within established loci, will likely increase the explained variance in obesity-related traits substantially. Such intermediate traits may increase our understanding of obesity genetics when studied as an outcome or as an exposure in interaction with genetic information. Future studies aiming to identify causal genes and variants within these loci are required before their relevance for obesity etiology can be established. In addition, improved knowledge of human genetic variation acquired by large-scale sequencing efforts like the 1000 Genomes Project118 has already led to the development of more dense genome wide arrays. These arrays cover variants with a minor allele frequency as low as 1% and provide improved coverage of common variants when compared with previously described arrays. Variability in the heritability of body masss index: A systematic review and metaregression. Non-synonymous polymorphisms in melanocortin-4 receptor protect against obesity: the two facets of a Janus obesity gene. Examining all available variants in extremes of the population may identify novel loci as well as identify causal variants within established loci. Functional follow-up in animal models can help pinpoint the causal genes within loci by selectively overexpressing or inactivating positional candidate genes, either at the wholebody or tissue level.

Therefore, we cannot use the presence/absence of the metabolic syndrome as a therapeutic end point. As a simple example, an individual meeting all five variables could improve on all criteria in response to whichever lifestyle modification program or therapy he/she wants to try, but if he or she still meets three out of the five criteria, he or she would nevertheless be considered as a nonresponder to treatment. This example clearly shows that the metabolic syndrome cannot be used as a therapeutic target and that changes in its individual components should rather be considered. We have suggested that the presence/absence of the metabolic syndrome could increase/decrease the level of risk predicted by the Framingham algorithm. These results clearly indicate that the metabolic syndrome is infrequently observed among lean individuals and that some excess of abdominal fat accompanies this constellation of metabolic abnormalities. However, the cutoff values defining abdominal obesity have not been defined on solid scientific grounds, and further work in this area is clearly warranted. Obesity and Metabolic Syndrome 553 130 125 Waist circumference (cm) 120 115 110 105 100 95 90 85 Clinical criteria Waist girth >102 cm Triglycerides 1. Although the most prevalent form of the metabolic syndrome is found among sedentary individuals who have too much visceral adipose tissue, the reasons for this relationship are not fully understood and are still under investigation. Elegant animal studies by Bergman and colleagues64 have even suggested that the nocturnal rise in free fatty acid levels associated with excess visceral adiposity could be particularly detrimental to insulin resistance and related metabolic abnormalities. Finally, the third possibility does not exclude the two aforementioned scenarios: excess visceral adiposity may also be a marker of the relative inability of subcutaneous adipose tissue to store excess energy. Altered metabolic pro le: Insulin resistant milieu Pro-inflammatory state Pro-thrombotic state Pro-hypertensive state Ectopic fat deposition: Liver fat Intramuscular lipids Pancreas fat Perivascular fat Epi/pericardial fat Renal fat Etc. However, when facing the same energy surplus the individual who cannot expand his or her adipose tissue mass through hyperplasia will first accumulate energy through hypertrophy of adipose cells. As fat cell size expansion has limits, the storage capacity of adipose tissue will eventually reach saturation, leading to an energy spillover and to the accumulation of lipids at undesirable sites such as the liver, heart, muscle, pancreas, and kidney, a process referred to as ectopic fat deposition, which has been associated with insulin resistance and with the clustering abnormalities of the metabolic syndrome. Reviewing the link between these various ectopic fat depots and features of insulin resistance is way beyond the scope of this chapter; suffice it to mention that all ectopic lipid depots are associated with various features of insulin resistance. To clarify their respective roles, Britton and Fox74 suggested that we could classify the various ectopic fat depots into those with systemic effects (visceral adipose tissue, liver, and skeletal muscle) and those more likely to have local effects (heart, kidney, pancreas, and perivascular adipose tissue). Extensive imaging studies are currently under way on large samples, which should help us better understand the respective roles of these ectopic fat depots as key players, partners in crime, or innocent bystanders. The latter possibility is a less likely scenario: it is more probable that some lipid depots have a greater influence than others depending on the metabolic variable considered, whereas some others may also contribute to the development of specific clinical outcomes. Such a proper, extensive mapping of ectopic fat depots is key to redefining what really is overweight/obesity as a condition associated with comorbidities. All studies have shown that there is a strong correlation between visceral adiposity and liver fat content and that both adipose tissue/liver lipid depots are associated with features of the metabolic syndrome. It is more likely that these two depots are key determinants/correlates of the systemic cardiometabolic risk profile, with the relative weight of the two variables depending on the variable/end point considered. There was therefore a need to identify simple markers of excess visceral adiposity associated with a given waistline. In 2000, we proposed that the simultaneous elevation of waist circumference and of fasting triglyceride levels, a phenotype that we have described as "hypertriglyceridemic waist," was predictive of a very high probability (between 75% and 85% depending on the study/sample considered) of being characterized by excess visceral adiposity, insulin resistance, and features of the metabolic syndrome. It is now clear that a combination of insulin resistance and impaired -cell insulin secretion is necessary to develop this metabolic disease. As a sedentary lifestyle and abdominal obesity are key underlying causes of the metabolic syndrome, it will never be emphasized enough that a clinical diagnosis of the metabolic syndrome should not necessarily first lead to pharmacotherapy. Rather, it should represent "a window of opportunity" for treating physicians and their patients diagnosed with this condition. Clearly, these patients would considerably benefit from regular physical activity/exercise, leading to an improvement in their cardiorespiratory fitness and a reduction in their waist circumference.

Isolated sixth or third cranial nerve palsies, asymmetric proximal motor neuropathy in the legs, truncal neuropathy, autonomic neuropathy, and an increased frequency of entrapment neuropathy (see below). The remainder have an axonal disorder; 50% of these have vasculitis- usually due to a connective tissue disorder. In this latter group, immunosuppressive treatment of the underlying disease (usually with glucocorticoids and cyclophosphamide) is indicated. Sensory and motor symptoms are in the distribution of a single nerve- most commonly ulnar or median nerves in the arms or peroneal nerve in the leg. Surgical decompression considered if chronic course (lack of response to conservative treatment), motor deficit, and electrodiagnostic evidence of axonal loss. Patterns of weakness, sensory loss, and conservative/ surgical treatment options are listed in Table 197-3. Characteristic distribution: cranial muscles (lids, extraocular muscles, facial weakness, "nasal" or slurred speech, dysphagia); in 85%, limb muscles (often proximal and asymmetric) become involved. Complications: aspiration pneumonia (weak bulbar muscles), respiratory failure (weak chest wall muscles), exacerbation of myasthenia due to administration of drugs with neuromuscular junction blocking effects (tetracycline, aminoglycosides, procainamide, propranolol, phenothiazines, lithium). Postsynaptic folds are flattened or "simplified," with resulting inefficient neuromuscular transmission. Thymectomy improves likelihood of longterm remission in adult (less consistently in elderly) pts. Myasthenic crisis is defined as an exacerbation of weakness, usually with respiratory failure, sufficient to endanger life; expert management in an intensive care setting essential. These disorders are usually painless; however, myalgias, or muscle pains, may occur. A muscle contracture due to an inability to relax after an active muscle contraction is associated with energy failure in glycolytic disorders. Myotonia is a condition of prolonged muscle contraction followed by slow muscle relaxation. It is important to distinguish between true muscle weakness and a complaint of fatigue; fatigue without abnormal clinical or laboratory findings almost never indicates a true muscle disorder. Weakness typically becomes obvious in the second to third decade and initially involves the muscles of the face, neck, and distal extremities. This results in a distinctive facial appearance ("hatchet face") characterized by ptosis, temporal wasting, drooping of the lower lip, and sagging of the jaw. Myotonia manifests as a peculiar inability to relax muscles rapidly following a strong exertion. Respiratory function should be carefully followed, as chronic hypoxia may lead to cor pulmonale. Facioscapulohumeral Dystrophy An autosomal dominant, slowly progressive disorder with onset in the third to fourth decade. Weakness involves facial, shoulder girdle, and proximal arm muscles and can result in atrophy of biceps, triceps, scapular winging, and slope shoulders. Foot drop and leg weakness may cause falls and progressive difficulty with ambulation. Limb-Girdle Dystrophy A constellation of diseases with proximal muscle weakness involving the arms and legs as the core symptom. Age of onset, rate of progression, severity of manifestations, inheritance pattern (autosomal dominant or autosomal recessive), and associated complications. At least eight autosomal recessive forms have been identified by molecular genetic analysis. Duchenne Dystrophy X-linked recessive mutation of the dystrophin gene that affects males almost exclusively.

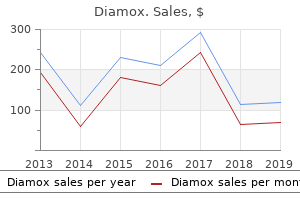
Sweet Mandulin (Hemp Agrimony). Diamox.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96497
Other uses (a) To potentiate hypnotics, analgesics and anaesthetics: such use is rarely justified now. In 1949, it was found to be sedative in animals and to exert beneficial effects in manic patients. In the 1960s and 1970s the importance of maintaining a narrow range of serum lithium concentration was realized and unequivocal evidence of its clinical efficacy was obtained. Over the past 2 decades, several anticonvulsants and atypical antipsychotics have emerged as alternatives to lithium with comparable efficacy. It is neither sedative nor euphorient; but on prolonged administration, it acts as a mood stabiliser in bipolar disorder. However, the following mechanisms have been proposed: (a) Li+ partly replaces body Na+ and is nearly equally distributed inside and outside the cells (contrast Na + and K + which are unequally distributed); this may affect ionic fluxes across brain cells or modify the property of cellular membranes. However, relative to Na+ and K+ concentration, the concentration of Li + associated with therapeutic effect is very low. An attractive hypothesis has been put forward based on the finding that lithium in therapeutic concentration range inhibits hydrolysis of inositol-1-phosphate by inositol monophosphatase. The hyperactive neurones involved in the manic state may be preferentially affected, because supply of inositol from extracellular sources is meagre. Lithium inhibits release of thyroid hormones resulting in feedback stimulation of thyroid through pituitary. Majority of Li+ treated patients remain in a state of compensated euthyroidism, but few get decompensated and become clinically hypothyroid. Pharmacokinetics and control of therapy Lithium is slowly but well absorbed orally and is neither protein bound nor metabolized. It first distributes in extracellular water, then gradually enters cells and penetrates into brain, ultimately attaining a rather uniform distribution in total body water. When Na+ is restricted, a larger fraction of filtered Na+ is reabsorbed, so is Li+. Thus, with the same daily dose, different individuals attain widely different plasma concentrations. Since the margin of safety is narrow, monitoring of serum lithium concentration is essential for optimising therapy. Serum lithium level is measured 12 hours after the last dose to reflect the steady-state concentration; 0. Peaks in plasma lithium level over and above the steady-state level occur after every dose. Nausea, vomiting and mild diarrhoea occur initially, can be minimized by starting at lower doses. Thirst and polyuria are experienced by most, some fluid retention may occur initially, but clears later. In acute intoxication these symptoms progress to muscle twitchings, drowsiness, delirium, coma and convulsions. Vomiting, severe diarrhoea, albuminuria, hypotension and cardiac arrhythmias are the other features. Enough hormone is usually produced due to feedback stimulation so that patients remain euthyroid. Lithium induced goiter and hypothyroidism does not warrant discontinuation of therapy; can be easily managed by thyroid hormone supplementation. Lithium is contraindicated during pregnancy: foetal goiter and other congenital abnormalities, especially cardiac, can occur; the newborn is often hypotonic.
A history of stroke suggests multi-infarct dementia, which may also occur with hypertension, atrial fibrillation, peripheral vascular disease, and diabetes. A history of gastric surgery may result in loss of intrinsic factor and vitamin B12 deficiency. A careful review of medications, especially of sedatives and tranquilizers, may raise the issue of drug intoxication. Insomnia or weight loss is often seen with pseudodementia due to depression, which can also be caused by the recent death of a loved one. Examination It is essential to document the dementia, look for other signs of nervous system involvement, and search for clues of a systemic disease that might be responsible for the cognitive disorder. Dementia with a myelopathy and peripheral neuropathy suggests vitamin B12 deficiency. A peripheral neuropathy could also indicate an underlying vitamin deficiency or metal intoxication. Confusion associated with repetitive stereotyped movements may indicate ongoing seizure activity. Hearing impairment or visual loss may produce confusion and disorientation misinterpreted as dementia. Choice of Diagnostic Studies the choice of tests in the evaluation of dementia is not straightforward. A reversible or treatable cause must not be missed, yet no single etiology is common; thus a screen must employ multiple tests, each of which has a low yield. Lumbar puncture need not be done routinely but is indicated if infection is a consideration. Memory loss is often not recognized initially, in part due to preservation of social graces until later phases; impaired activities of daily living (keeping track of finances, appointments) draw attention of friends/family. Disorientation, poor judgment, poor concentration, aphasia, and apraxia are increasingly evident as the disease progresses. Help may be needed with the simplest tasks, such as eating, dressing, and toilet function. Often, death results from malnutrition, secondary infections, pulmonary emboli, or heart disease. The focus is on judicious use of cholinesterase inhibitor drugs; symptomatic management of behavioral problems; and building rapport with the pt, family members, and other caregivers. Management of behavioral problems in conjunction with family and caregivers is essential. Extremely heterogeneous; presents with combinations of disinhibition, dementia, apraxia, parkinsonism, and motor neuron disease. May be sporadic or inherited; some familial cases due to intronic mutations of tau gene on chromosome 17. Treatment is symptomatic; no therapies known to slow progression or improve cognitive symptoms. Anticholinesterase compounds, exercise programs to maximize motor function, antidepressants to treat depressive syndromes, and antipsychotics in low doses to alleviate psychosis may be helpful. Peak age of onset in the 60s (range is 35 to 85); course progressive over 10 to 25 years. Other findings: rigidity ("cogwheeling"- increased ratchet-like resistance to passive limb movements), bradykinesia (slowness of voluntary movements), fixed expressionless face (facial masking) with reduced frequency of blinking, hypophonic voice, drooling, impaired rapid alternating movements, micrographia (small handwriting), reduced arm swing while walking, flexed "stooped" posture with walking, shuffling gait, difficulty initiating or stopping walking, en-bloc turning (multiple small steps required to turn), retropulsion (tendency to fall backwards). Etiology Degeneration of pigmented pars compacta neurons of the substantia nigra in the midbrain resulting in lack of dopaminergic input to striatum; accumulation of eosinophilic intraneural inclusion granules (Lewy bodies). Cause of cell death is unknown, but it may result from generation of free radicals and oxidative stress. Rare genetic forms of parkinsonism exist; most common are mutations in -synuclein or parkin genes.
The obvious cause in this patient is the additive hypoprothrombinaemic action of inj ceftriaxone given for treatment of pelvic infection. This complication could have been prevented either by selecting an antibiotic that does not cause hypoprothrombinaemia/interact with warfarin or by reducing the dose of warfarin when ceftriaxone was started. Because Hb level is 9 g/dl, blood transfusion is not required at this stage, but must be kept handy in case she bleeds further. Changing the antibiotic to one which does not cause hypoprothrombinaemia or bleeding may be considered on the basis of bacteriological sensitivity of the organism causing pelvic infection. Thus, apart from lifestyle changes to regulate diet, reduce body weight and increase physical exercise, he requires lipid lowering medication. However, it alone cannot prevent recurrences, which most commonly are caused by persistent Contd. Since the same cannot be confirmed in the absence of testing facility, he should be given the benefit of H. This child has developed acute muscular dystonia, an extrapyramidal motor reaction that can be caused by drugs with dopaminergic D2 receptor blocking action. Antiemetics with D2 blocking action are chlorpromazine and related neuroleptics like triflupromazine, prochlorperazine, etc. Though the dystonic reaction usually passes off within a few hours, it can be rapidly reversed by a parenterally administered centrally acting anticholinergic drug. This patient of diarrhoea seems to have lost only small amount of fluid and there are no signs of dehydration. Thus, there is no need of rehydration therapy, but normal fluid intake and nutrition should be continued. The features of this patient including fever are indicative of moderately severe enteroinvasive infection. A well absorbed fluoroquinolone like ciprofloxacin or ofloxacin would be suitable first line antibiotic for empiric therapy. Antimotility-antidiarrhoeal drug is contraindicated in this patient, because in all likelyhood there is enteroinvasive infection, so that restriction of bowel clearance can favour further bowel wall invasion and systemic spread of the pathogen. Therefore, prophylaxis covering aerobic as well as anaerobic organisms and both gram-negative as well as gram-positive bacteria would be appropriate. Normally, there is no need to repeat the injection, but if the surgery lasts more than 2 hours, a repeat injection after surgery may be given. Moreover, it has a convenient once a day oral dosing schedule and is generally well tolerated. These could be the considerations on the basis of which the doctor has decided to use moxifloxacin. However, moxifloxacin is not appropirate for this patient because she is receiving amitryptyline, a tricyclic antidepressant which has proarrhythmic potential. Moxifloxacin can prolong Q-T interval and increase the risk of serious cardiac arrhythmias such as Torsades de pointes when given along with amitryptyline. Other antibiotics which are active against gram-positive cocci and suitable for treating sinusitis are amoxicillin alone or with clavulanic acid, a first generation cephalosporin or azithromycin. In this patient antibiotic therapy should be started on the basis of clinical diagnosis, because the patient is quite sick. Moreover, blood culture is not necessarily positive in all cases of typhoid fever. The most appropriate antibiotic is ceftriaxone (or a similar 3rd generation cephalosporin like cefoperazone, cefotaxime), becuase it produces the fastest and surest response. The daily dose for this boy would be (75 mg/kg x 25 kg) = 1875 mg or rounded off to 2. In case of typhoid fever, a single antibiotic is sufficient, since addition of another antibiotic has not been found to hasten or improve the response. The most appropriate drugs and regimens for treating chlamydial endocervicitis are: Azithromycin 1. Both these regimens are adequate to treat uncomplicated gonococcal infection as well as concurrent chlamydial and gonococcal infection.
References:




