A systematic review of the published literature was conducted to answer these key questions and provide the evidence base for the guideline. Controlled vocabulary supplemented with keywords was used to search for studies according to each defined question. This search included articles published between January 1, 1980 February 6, 2017. The search yielded 15,217 references, 546 (enrolling approximately 350,000 men) of which were used to support guideline statements. Of the outcomes included in the protocol of this systematic review, data were available on quality of life (QoL), sexual function, cardiovascular events, anemia, bone health, insulin resistance, cardiovascular risk factors, mood, cognitive function, body composition, and numerous adverse events. Minimal data were found regarding outcomes of frailty, risk of venous thromboembolism, hyperestrogenemia, sleep apnea, prostate biopsy, recurrence of treated prostate cancer, and incidence of breast cancer. Evidence tables (for included studies) and evidence profiles (showing estimates of effect for the outcomes of interest) were generated and presented to the Panel. The categorization of evidence strength is conceptually distinct from the quality of individual studies. Evidence strength refers to the body of evidence available for a particular question and includes not only individual study quality but consideration of study design, consistency of findings across studies, adequacy of sample sizes, and generalizability of samples, settings, and treatments for the purposes of the guideline. By definition, Grade A evidence is evidence about which the Panel has a high level of certainty, Grade B evidence is evidence about which the Panel has a moderate level of certainty, and Grade C evidence is evidence about which the Panel has a low level of certainty. Strong Recommendations are directive statements that an action should (benefits outweigh risks/burdens) or should not (risks/burdens outweigh benefits) be undertaken because net benefit or net harm is substantial. Moderate Recommendations are directive statements that an action should (benefits outweigh risks/burdens) or should not (risks/burdens outweigh benefits) be undertaken because net benefit or net harm is moderate. Conditional Recommendations are non-directive statements used when the evidence indicates that there is no apparent net benefit or harm or when the balance between benefits and risks/ burdens is unclear. All three statement types may be supported by any body of evidence strength grade. Body of evidence strength Grade A in support of a Strong or Moderate Recommendation indicates that the statement can be applied to most patients in most circumstances and that future research is unlikely to change confidence. Body of evidence strength Grade B in support of a Strong or Moderate Recommendation indicates that the statement can be applied to most patients in most circumstances but that better evidence could change confidence. Body of evidence strength Grade C in support of a Strong or Moderate Recommendation indicates that the statement can be applied to most patients in most circumstances but that better evidence is likely to change confidence. Body of evidence strength Grade C is only rarely used in support of a Strong Recommendation. When body of evidence strength is Grade A, the statement indicates that benefits and 6 Copyright © 2018 American Urological Association Education and Research, Inc. When body of evidence strength Grade B is used, benefits and risks/burdens appear balanced, the best action also depends on individual patient circumstances, and better evidence could change confidence. When body of evidence strength Grade C is used, there is uncertainty regarding the balance between benefits and risks/burdens, alternative strategies may be equally reasonable, and better evidence is likely to change confidence. Where gaps in the evidence existed, the Panel provides guidance in the form of Clinical Principles or Expert Opinion with consensus achieved using a modified Delphi technique if differences of opinion emerged. A Clinical Principle is a statement about a component of clinical care that is widely agreed upon by urologists or other clinicians for which there may or may not be evidence in the medical literature. For additional information on the challenges associated with reviewing the literature on testosterone deficiency, refer to Appendix A. Additionally, identifying drugs solely by their chemical compound formulation allows guidelines to remain current, despite the dynamic nature of the marketplace. For most pharmaceutical products, the usage, dosage, and application is consistent across brands, and identification by chemical compound is sufficient to communicate to the reader when to use a given medication. While all products contain the same medication (testosterone), each product and modality has distinct pharmacokinetic and application attributes based on the excipient agents and the permeator components. Within this modality family alone, there are three different application sites, including upper body, thigh, and axilla, with four different dosing ranges for each gel. While there are three injectable drugs, two of them are short-acting and one is long-acting.
Case management, disease management and population health management programs to support the coordination and integration of care between providers. Fostering a culture of collaboration and cooperation helps Healthy Blue sustain a seamless continuum of care that positively impacts our member outcomes. To maintain continuity of care, patient safety and member well-being, communication between integrated health care providers is critical, especially for members with comorbidities receiving pharmacological therapy. Each offer of consent or release of substance use information should be documented and reported to Healthy Blue as requested. You should be able to provide initial and summary reports to the primary care provider or to Healthy Blue upon request. Continuity of Care To assist in the transition of Healthy Blue members from one level of care to another, Healthy Blue recommends transition meetings or appointments are held prior to the member moving from higher to lower 70 restrictive levels of care to assure continuity of treatment. Healthy Blue encourages providers to include Healthy Blue care managers in these meetings and appointments. Provider Success We believe the success of providers is necessary to achieve our goals. We are committed to supporting and working with qualified providers to ensure we jointly meet quality and recovery goals. Our commitment includes: · Improving communication of the clinical aspects of behavioral health care to improve outcomes and recovery. Health Plan Clinical Staff All clinical staff members are licensed and have prior health care experience. Our behavioral health medical director is board-certified in adult, adolescence and child psychiatry and licensed in the state of Louisiana. Our highly trained and experienced team of clinical care managers, case managers and support staff provide high-quality care management and care coordination services to our members and strive to work collaboratively with all providers. Member Records and Treatment Planning: Comprehensive Assessment Member records must meet the following standards and contain the following elements, if applicable, for effective service provision and quality reviews. Information related to the provision of appropriate services to members must be included in the records, with documentation in a prominent place whether there is an executed declaration for mental health treatment. Additionally, the development of a crisis prevention plan is required for those members with multiple hospitalizations or more than three visits to the emergency room for urgent or nonemergent care. Disclosures of substance use information must include a prohibition against redisclosure. There must be documentation that referral to appropriate medical or social support professionals have been made. A provider who discovers a gap in care is responsible to help the member get that gap in care fulfilled, and documentation should reflect the action taken. For providers of multiple services, one comprehensive treatment/care/support plan is acceptable as long as at least one goal is written and updated as appropriate for each of the different services that are being provided to the member. Psychotropic Medications Prescribing providers must inform all members considered for prescription of psychotropic medications of the benefits, risks and side effects of the medication; alternate medications; and other forms of treatment. If obesity is also a problem, the medical record needs to reflect that a healthy diet and exercise plan has been prepared and given to the member, or if appropriate, a referral to a nutritionist or obesity medical professional. Members on psychotropic medications may be at increased risk for various disorders. As such, it is expected that providers are knowledgeable about side effects and risks of medications and they regularly inquire about and look for any side effects. This especially includes: · Follow-up to inquire about suicidality or self-harm in children placed on antidepressant medications as per Food and Drug Administration and American Psychiatric Association guidelines. Summary guidelines are referenced in our clinical practice guidelines, located on our website at providers. While the prescriber is not expected to personally conduct all of these tests, the prescriber is expected to ensure these tests occur where indicated and to initiate appropriate interventions to address any adverse results. Timeliness of Decisions on Requests for Authorization the following are guidelines around the timeliness of decisions on authorization requests for behavioral health services: · If the referral is made from an emergency room or a facility that does not have a psychiatric unit, the decision will be made and communicated to the provider within one hour of the request. Access to Care Standards this grid outlines standards for timely and appropriate access to quality behavioral health care.
The evidence is unclear and limited regarding the use of this device in the chronic and subacute stroke phases. There is level 1b evidence that interferential current therapy may improve balance. There is level 1b and limited level 2 evidence that peroneal nerve stimulation may improve gait and quality of life post-stroke. There is level 1a evidence that neuromuscular electrical stimulation may not improve gait. Medications There is level 1a evidence that amphetamines may not improve lower limb function. There is level 1a evidence that methylphenidate not improve motor function following stroke. There is level 1b evidence that ropinirole may not be superior to placebo at increasing gait, functional recovery and activities of daily living post-stroke. There is level 1b evidence that citalopram may improve neurological function but not functional recovery following stroke. There is level 1b evidence that Almitrine in combination with Raubasine may improve functional outcomes post stroke. Spasticity and Contractures There is level 1b evidence that both a tilt table and night splint may prevent ankle contracture in the early period following stroke. There is level 1a evidence that treatment with botulinum toxin compared to placebo improves lower limb spasticity, but gains for functional recovery have not been significant. There is level 1b and limited level 2 evidence that treatment with botulinum toxin compared to phenol may improve lower limb spasticity. There is level 1b and limited level 2 evidence that treatment with botulinum toxin combined with casting or taping may improve lower limb spasticity but not gait. There is level 1b evidence that thermocoagulation treatment may improve lower limb spasticity, Achilles tendon flexion, and ankle clonus. There is conflicting level 1b and level 2 evidence regarding the use of Dantrolene on lower limb spasticity. There is level 1b evidence that there is no significant difference between treatment with Tizanidine or Baclofen for spasticity. There is level 1b evidence that total glucosides from Shaoyao and Gancao offered with rehabilitation exercise therapy may improve lower limb spasticity and functional recovery. There is level 1a and limited level 2 evidence transcutaneous electrical stimulation may improve spasticity outcomes post-stroke. There is level 1a and limited level 2 evidence functional electrical stimulation may improve spasticity outcomes post-stroke. There is limited level 2 evidence that therapeutic ultrasound may reduce alpha motor neuron excitability that is associated with ankle plantar flexor spasticity. There is level 1b evidence that rehabilitation programs compared to standard medications may improve spasticity for the elbows, fingers and plantar flexion. There is level 1a evidence that ankle exercises compared to conventional therapy may not improve gait, ankle range of motion or spasticity but may improve balance. There is level 3 evidence that robotic training may not improve spasticity, gait, or spasticity. There is level 1b evidence that a single session of isokinetic or isotonic muscle stretch may not improve measures of gait. There is level 1a evidence that transcranial direct current stimulation may not improve gait or balance outcomes, but may improve functional recovery and knee extension force. There is level 1b evidence that galvanic vestibular stimulation may not improve pusher behaviour or lateropulsion. Acupuncture and Chinese Herbal Medicine There is level 1a evidence from high-quality, high-powered studies that acupuncture may not improve balance, gait, motricity, spasticity or independent functioning. However, there is limited level 2 evidence from low-quality studies that balance, motor function and performance of activities of daily living may be improved following acupuncture. There is level 1b evidence that acupressure led by nurses may improve lower limb motor function.
Five-day cefdinir course vs ten-day cefprozil course for treatment of acute otitis media. A pooled comparison of cefdinir and penicillin in the treatment of group A beta-hemolytic streptococcal pharyngotonsillitis. Comparison of amoxicillin/clavulanic acid high dose with cefdinir in the treatment of acute otitis media. Comparison of cefdinir and cefaclor in the treatment of community-acquired pneumonia. Comparison of a 5 day regimen of cefdinir with a 10 day regimen of cefprozil for treatment of acute exacerbation of chronic bronchitis. A comparison of cefditoren pivoxil and amoxicillin/clavulanate in the treatment of community-acquired pneumonia: a multicenter, prospective, randomized, investigator-blinded, parallel-group study. A comparison of single-dose cefixime with ceftriaxone as a treatment for uncomplicated gonorrhea. Comparative study of ceftibuten and cefixime in the treatment of complicated urinary tract infections. Cefdinir versus cefaclor in the treatment of uncomplicated urinary tract infection. Cefpodoxime proxetil suspension compared with cefaclor suspension for treatment of acute otitis media in pediatric patients. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. A prospective, randomized, double dummy, placebo-controlled trial of oral cefditoren pivoxil 400mg once daily as switch therapy after intravenous ceftriaxone in the treatment of acute pyelonephritis. Comparison of cefdinir and penicillin for the treatment of streptococcal pharyngitis. Orally administered cefpodoxime proxetil for treatment of uncomplicated gonococcal urethritis in males: a doseresponse study. Five-day oral cefditoren pivoxil versus 10-day oral amoxicillin for pediatric group A streptococcal pharyngotonsillitis. Effective short-course treatment of acute group A beta-hemolytic streptococcal tonsillopharyngitis. Double-blind comparison of cefixime and cefaclor in the treatment of acute otitis media in children. Single-dose cefixime versus single-dose ceftriaxone in the treatment of antimicrobial resistant Neisseria gonorrhoeae infection. Oral cefixime versus intramuscular ceftriaxone in patients with uncomplicated gonococcal infections. Comparative evaluations of cefpodoxime versus cefixime in children with lower respiratory tract infections. Clinical practice guideline for the diagnosis and management of group a streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Practice guidelines for the diagnosis and management of skin and soft-tissue infections: 2014 update by the Infectious Diseases Society of America. Comparison of oral cefpodoxime proxetil and cefaclor in the treatment of skin and soft tissue infections. Cefdinir versus cephalexin for the treatment of skin and skin structure infections. Study of use of cefdinir versus cephalexin for treatment of skin infections in pediatric patients. International study comparing cefdinir and cefuroxime axetil in the treatment of patients with acute exacerbation of chronic bronchitis. Cefditoren pivoxil versus cefpodoxime proxetil for community-acquired pneumonia: results from a multi-center, prospective, randomized, double-blind study. Randomized comparative study of cefixime versus cephalexin in acute bacterial exacerbations of chronic bronchitis.
Medicaid has a rule that says only one preferred product needs to be tried for anti-psychotics. So even if down the road we make some products non-preferred, only a single agent is required to be tried first. It is important to realize that trying one drug before going to another is not always a good idea with these long-acting injectables. Most of us will try an oral drug first if we have a new patient to find what works. Having to back up and do a trial first is a very bad idea with a patient with schizophrenia because there is time involved. We want open access to allow the physician, patient and family to make the decision. I do want to add that the long-acting injectable products have really turned around psychiatric treatment of the seriously mentally ill. They are working well with drug courts, the criminal justice system and outpatient treatment. We support open access to allow individualized and appropriate treatment with patients with serious mental illness. These patients are heterogeneous in nature and given the open access that Optum has proposed is something we support. There are a number of meta-analysis and systemic reviews that have been conducted trying to compare them. But this is really an individual treatment and disease and different antipsychotics work differently for different people. The guidelines suggest a long-acting injectable if the patient is having trouble with adherence, or if they are just having chronic relapses. Some have more flexibility or longer duration, from two weeks to monthly to every two months. Optum recommends the board consider the medications in this class be considered clinically and therapeutically equivalent. Sapandeep Khurana: How will this vote affect what was presented from the audience in regard to open access? Carl Jeffery: the board is voting on if these medications are all loosely interchangeable and are recognizing the products have similar indications or are in the same class of medications. Page 10 of 18 57 Sapandeep Khurana: As a psychiatrist, while their mechanisms of action might make them similar and therapeutically equivalent, their effect is extremely different for what they do for patients. I want to add a comment that it is no longer a recommendation that we have to wait for people to fail multiple trials and have multiple episodes of non-adherence before trying a long-acting. There is evidence that starting long-acting prevents relapses and improve the life of people with mental illness. Carl Jeffery: the board could make the recommendation that if there were one or two agents that were clearly superior to the rest of them, then you could call those out. That would document that statement where you go into the next vote for preferred or non-preferred. If you identify a product with a clinical advantage, but we recommend it added as non-preferred, that would have an impact in your voting. For example, if we were trying to include older agents like Haldol Decanoate with this class, we might say they are not the same. Carl Jeffery: Optum recommends all the products in this class, the long-acting injectable atypical antipsychotics be added as preferred. For Possible Action: Discussion and possible adoption of biologic response modifiers, multiple sclerosis agents, oral Carl Jeffery: We will move to the Established Drug Classes and our first class is the Biologic Response Modifiers, Multiple Sclerosis Agents, Oral. Looking at the indications for the different agents, the only one that has something different is Mavenclad. Most of them are once or twice daily except for Mavenclad that has a unique dosing cycle. Carl Jeffery: Optum recommends the new product, Vumerity, be added as non-preferred and the rest of the class remain the same. For Possible Action: Discussion and possible adoption of cardiovascular agents, antihypertensive agents, calcium-channel blockers Carl Jeffery: the next class is calcium channel blockers and Optum requests the chair to bypass this class. Hearing none, by unanimous consent, we will move along to the next item on the agenda. Penny Higashi: this Penny Higashi with Boehringer-Ingelheim, I have a quick question about the combinations not being covered?
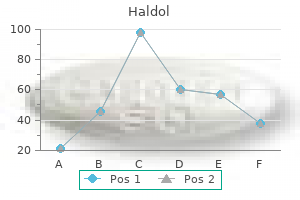
Zinc. Haldol.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96943
This research project, a safety study in rats, found no drug-related deaths or organ toxicity when the drug was administered at a level 30-60 times higher than what has been found to be effective. Based on these findings, the National Cancer Institute has agreed to support additional preclinical studies on this new anti-cancer agent. Inhibition of Brain Metastases in Breast Cancer Up to 30 percent of breast cancer patients will have their cancer metastasize to the brain. Because current treatments for breast cancer metastases are not very successful, new approaches are needed. This work led them to identify a new molecular target on metastatic breast cancer cells. The target is a cell adhesion receptor, called the activated conformer of integrin avЯ3. The team found that this receptor promotes breast cancer cell metastases to the brain and central nervous system. They also showed that treatment with antibodies against activated avЯ3 could reach target organs of breast cancer metastasis, including the brain. This 47 work could lead to the development of a new therapy for brain metastases in breast cancer patients. Susan Love Research Foundation 51 the Biology of the Breast Cell To understand the origin of breast cancers, more research is needed on the pre-cancerous, causative events in the normal breast. In breast development, cell populations must co-ordinate migration, proliferation, and apoptosis (cell death) over space and time. In cancer progression, these same processes become dysregulated, initially at the genetic level, it leads to the physiological changes associated with malignancy. To better mimic breast and tumor architecture, 3-D cell culture models provide a means to explore potential underlying mechanisms and show the structure of the breast and interaction of its different cell types lead to the development of a tumor. Stem cell populations reside in body organs to provide the raw material for tissue regeneration, repair, and for the cyclic proliferation responses to hormones and pregnancy in the breast. If this theory proves correct, then only a small fraction (1- 2 percent) of cells in a tumor mass retain stem cell properties, and these "cancer stem cells" must be selectively targeted to achieve an effective eradication of the disease. However, over the past decade researchers have realized that the underlying mechanistic driving forces of tumor biology operate though complex, concurrent genetic changes in numerous molecular pathways. Still, it remains the metastatic process that presents the greatest hurdle in our efforts to contain and destroy cancer as it too often presents itself at the time of diagnosis. Breast cancer can spread to almost any region of the body, although metastases are most common to the bone, lung and liver. Understanding the gene and physiological regulatory mechanisms for this cancer cell diaspora is crucial for the design of therapeutic strategies. This communication organizes the cells into tissues and prevents uncontrolled cell growth. Two types of proteins, called integrins and dystroglycan receptors, are known to contribute to cancer progression. The Role of Gli3 in Mouse Embryonic Mammary Gland Formation Scientists recognize that tumors arise when the genes that play a role in normal development stop functioning properly. Mutant mice in which the genes Gli3, Fgf10, or Fgfr2b do not properly function have similar defects in breast development. Veltmaat and her team found that in the Gli3 and Fgf10 mutant mice, the fourth breast pair developed, but the third pair did not. The team also found that when Gli3 was absent, the production level of Fgf10 remained too low to induce signaling between Fdf10 and another molecule called Wnt. It also suggested that Gli3 might start to function as a breast cancer gene when its levels get too high. The team is now investigating how to return Gli3 functioning that is too high to normal levels. Epithelial Polarity, Organization, and the Angiogenic Switch For a tumor to become invasive, it first must develop the new blood vessels that will allow it to grow and spread, a process known as angiogenesis. Boudreau and her team found that normal cells, which appear organized (or polarized) inside, suppressed expression of angiogenic factors whereas disorganized cells and breast tumors cells had higher levels of these factors. They also found that by restoring expression of a gene, called HoxD10, which is missing in aggressive tumors, they could revert tumor cells back to an organized, polarized state.
There is level 1b evidence that Attention Process Training may improve aspects of visual and auditory attention. There is level 1b evidence that an intensive, computerized training program may result in improvements in both working memory and attention. Remediation of Memory Deficits Post Stroke There is level 1a evidence that compensatory strategies may be effective at improving memory outcomes, including imagery-based, process-oriented, and self-efficacy training. There is level 1b evidence that home visits combined with mailed letters containing resources and information may result in an improvement of self-reported health status for both patients and caregivers after 6 months compared to mailed letters only. There is level 1b and level 2 evidence that mental imagery may improve relearning of activities of daily living in patients with acute stroke and minimal cognitive deficits. There is limited level 2 evidence that patients in group-based interventions may not improve memory abilities any better than patients who did not receive intervention while on a waiting list. Rehabilitation of Executive Function and Problem Solving Post Stroke There is level 1b evidence that an analogical problem solving skills approach may increase problem solving abilities and performance of extended activities of daily living. There is level 1b evidence that self-regulation training may increase executive control over motor but not cognitive function, although these findings may be biased. There is level 2 evidence that goal management training may be beneficial in the rehabilitation of executive function. Multi-Modal Interventions Post Stroke There is level 1b evidence that standard care combined with computerized training may improve cognitive performance more than standard care alone. There is limited level 2 evidence that virtual reality training combined with computerized training may improve cognitive performance more than computerized cognitive training alone. Music Listening Therapy Post Stroke There is level 1b evidence that self-regulated music therapy may have a positive impact on verbal memory and focused attention in individuals with left hemisphere stroke. Exercise Programs Post Stroke There is conflicting level 1a evidence regarding the effect of exercise therapy on cognitive rehabilitation post stroke. There is level 1b and level 2 evidence that exercise programs with a focus on resistance, balance and aerobics can result in significant cognitive gains. Repetitive Transcranial Magnetic Stimulation Post Stroke Executive Summary (17th Edition) Aspirin for Vascular Dementia There is level 1b evidence that aspirin is effective in stabilizing and/or improving cognitive outcomes in patients with multi-infarct dementia. Donepezil for Vascular Dementia There is level 1a evidence that donepezil taken for 24 weeks may improve cognitive function in patients with probable or possible vascular dementia. There is level 1a evidence that treatment with donepezil is associated with improvement in global function for individuals with probable or possible vascular dementia. Rivastigmine for Vascular Dementia There is conflicting level 1a evidence regarding treatment with rivastigmine and its effect on vascular dementia and cognitive decline. There is level 2 evidence that treatment with rivastigmine is associated with more stable cognitive performance and improved behavioural outcomes among patients with vascular dementia. Galantamine for Vascular Dementia There is level 1a evidence that treatment with galantamine is associated with improvements in cognitive and global function. However, the benefits associated with treatment are more clearly demonstrated among patients with mixed dementia than vascular dementia. Nimodipine for Vascular Dementia There is level 1a evidence that nimodipine may not be beneficial in the treatment of vascular dementia. There is level 1b evidence that treatment with nimodipine may slow cognitive deterioration in patients with vascular dementia. Conclusions Regarding Memantine for Vascular Dementia There is level 1a evidence that treatment with memantine is associated with stabilization or improvement of cognitive function in patients with vascular dementia. Pentoxifylline for Vascular Dementia There is level 1a evidence that treatment with pentoxifylline is associated with cognitive benefits in patients with multi-infarct dementia. Citicoline for Cognitive Function There is conflicting level 1a evidence regarding the effect of citicoline in the long term management of cognitive function post stroke. Selegiline for Cognitive Function There is level 1b evidence that selegiline may improve cognitive function post stroke, with benefits lasting as long as six weeks. Prevention of Delirium There is level 2 evidence that a multi-component approach to the management of known risk factors may be associated with reduced incidence and duration of delirium.
Department of Ophthalmology, Buddhist Tzu Chi General Hospital, Taipei Branch, New Taipei, Taiwan,1 School of Medicine, Tzu Chi University, Hualien, Taiwan. Methods: Fifty-eight women 30 to 60 years of age with lateral canthal rhytides were prospectively recruited one regional hospital. Botulinum toxin type A was injected at the lateral canthal areas; one eye of each subject was randomly chosen for dose A (3 injections, 2 U in 0. Conclusions: Tear film stability decreased as soon as 1 week after botulinum toxin treatment for lateral canthal rhytides, and the effect persisted for more than 3 months. Tear production decreased to the trough at 1 month after treatment and then recovered gradually. Methods: Sixty eyes of 30 rabbits were divided into three groups according to the intensity of light exposure by an operating microscope: Control group, no exposure to light; Group A, 40,000-lux intensity for 30 min; and Group B, 100,000-lux intensity for 30 min. Conclusions: Light exposure from an operating microscope had a phototoxic effect on the ocular surface and tear film in this in vivo experiment. Therefore, excessive light exposure during ophthalmic procedures could be a pathogenic factor of dry eye syndrome after surgery. Kyu Yeon Hwang, Kyung-Sun Na, Jee-Won Mok, Choun-Ki Joo Department of Ophthalmology and Visual Science, Catholic university of Korea, Catholic Institute of Visual Science, Seoul, Republic of Korea. Methods: Thirteen eyes of 13 patients with essential blepharospasm were included in this prospective study. Patients were evaluated prior to and at 2-week and 1-, 3- and 6-month time points following injections. Subjects with a history of ocular surgery, trauma, contact lens and topical medication use were excluded. None of the Schirmer test values at follow-up visits were significantly different as compared to baseline levels (11. Department of Ophthalmology, University of Erlangen-Nuremberg, Germany Purpose: To investigate the density of Langerhans cells in the central cornea of patients with dry eye syndrome under topical antiinflammatory therapy with cyclosporine A 0. Methods: 31 patients (age 21-85 years) with severe dry eye were enrolled in the trial. Results: There was a significant reduction in Langerhans cell density in the central corneal epithelium after anti-inflammatory treatment from 110±12 cells/mmІ to 56±10 cells/mmІ. Tear film osmolarity, Schirmer test with anesthesia and meibomian gland dysfunction did not show significant changes. Conclusions: Evaluation of Langerhans cell density in the central corneal epithelium by in vivo confocal microscopy could be an effective objective diagnostic feature in monitoring anti-inflammatory therapy in patients with dry eye disease or other ocular surface pathologies. Conclusions: Botulinum toxin-A injection appears to have a positive but temporary effect on ocular surface parameters in patients with blepharospasm. Following evaporative stress there is a marked increase in cell proliferation that is 67 - Tear Film & Ocular Surface Society coupled with abnormal maturation of gland lipid that leads to a higher meibum protein content within the lipid of the central duct. Together these findings suggest that the meibomian gland can respond dynamically to environmental stress and that stress can affect meibum lipid maturation leading to changes in meibum quality. Methods: the superior and inferior eyelids from a single eye of 40 participants were imaged 3 times on the K4 and K5M. The images were organized into 3 sets each containing 160 images (2 devices x 40 images each for inferior superior eyelid). The first set of images served to train 2 observers, O1 and O2; the second and third sets were presented to both observers (24 hours apart) on a 50" high definition monitor in a darkened room. Results: For both devices combined, the mean difference in ratings between O1 and O2 was 0. When looking at both devices individually, the inter-observer mean differences in ratings when using the K4 was -0. When comparing ratings between sessions for each observer, the intra-observer mean difference in ratings for O1 was -0. Conclusion: the repeatability of the K5M was slightly better than the K4 when using a 4-point grading scale. In all cases, both observers graded within -1 to +1 grades of each other and against themselves. Contact lens case contamination with biofilms occurs often due to the resistance of the bacterial aggregates to the antimicrobials present in contact lens care solutions. Methods: Staphylococcus aggregates were formed by growing the bacteria on Mueller-Hinton Agar, harvesting with physiological saline and washing using centrifugation (500 x g for 5 minutes).
References:




