Exceptions to this rule do occur, especially in those with late onset in the sixth decade or beyond, when one may see primarily chorea, with little or no cognitive deficit (Britton et al. Chorea may initially present as fidgetiness, clumsiness, or a tendency to drop things; obvious choreiform movements are generally first visible on the face (including the forehead), from where they spread to involve the trunk and extremities. Importantly, these choreiform movements are quite brief, appearing and disappearing on a random basis from one location to another with lightning-like rapidity. Interestingly, although some patients seem fully aware of their chorea, it is not at all uncommon to find patients with obvious chorea denying that anything is amiss. The depth of this denial is at times extreme: I have seen patients with chorea of such severity as to preclude safe ambulation who nevertheless stoutly deny that anything at all is amiss. Early on in the course of the disease, patients may attempt, with varying degrees of success, to disguise the choreic movements by merging them with purposeful movements: for example, a choreic fling of the arm up to the head may be purposefully extended to draw the fingers through the hair, as if the purpose had all along been to straighten the hair. Dysarthria often occurs, as does dysphagia, which may lead to aspiration (Leopold and Kagel 1985). The chorea eventually makes almost all purposeful activity, whether eating, dressing, or walking, almost impossible, and patients eventually become chairbound or bedridden. At the end, the chorea may gradually disappear, to be replaced by a rigid, akinetic state (Feigin et al. The personality change presents with poor judgment, impulsivity, irritability, and an overall coarsening of behavior. Over time, as noted earlier, a dementia develops, characterized by deficits in memory, concentration, calculation, and abstraction; focal signs, such as aphasia and apraxia, are generally not seen. Associated symptoms are found in the vast majority of patients (Caine and Shoulson 1983; Folstein et al. These include depression of variable severity in roughly half, agitation, irritability, apathy and anxiety, and, in a minority, euphoria or, rarely, mania. A positive family history is almost universally found, and in one American family it was possible to trace the disease back to an ancestor who arrived with the Puritans (Vessie 1932). Exceptions to this rule may occur secondary to rarely occurring spontaneous mutations or, more commonly, to uncertain parentage (Ramos-Arroyo et al. Those with an earlier age of onset, for example those with the Westphal variant, experience a more rapid course, with death within about 10 years; conversely, those with a late onset, in the fifth decade or beyond, typically experience a more leisurely course. Differential diagnosis Genetic testing has greatly simplified the differential diagnostic task, and should be considered in any patient with the gradual onset of chorea in late adolescence or early adult years. Another differential possibility to consider is schizophrenia, especially when this is complicated by tardive dyskinesia. Certain features of the chorea seen in these two situations, however, may enable a clinical differentiation. The chorea of tardive dyskinesia is generally stereotyped and repetitive, almost never involves the forehead, and generally leaves gait relatively unaffected. Although an inverse correlation has been found with the number of repeats and the age of onset (Marder et al. Neuronal loss and reactive astrocytosis is noted in these areas; in the caudate nucleus in particular, spiny neurons are lost first (Mann et al. Surviving neurons may display intranuclear inclusions, which contain the huntingtin protein. Of the antipsychotics, the first-generation agent haloperidol is most often used, in doses from 1 to 10 mg/day (Barr et al. Akathisia may occur with haloperidol and, hence, second-generation agents, such as olanzapine (Bonelli et al. Tetrabenazine, a dopamine depleter not available in the United States, is also beneficial (Huntington Study Group 2006). In cases complicated by agitation or delusions or hallucinations, antipsychotics may also be useful. Ongoing research efforts are underway to find treatments that may retard the progression of the disease, and many patients are highly motivated to participate. As noted earlier, genetic testing is now available, and should be offered to patients with a compatible clinical Figure 8. Extensive counselling resources should be available for instances when the test is positive. This last characteristic, namely acanthocytosis, qualifies choreoacanthocytosis as one member of a larger group of disorders known as the neuroacanthocytoses, which, as noted below in the discussion on differential diagnosis, includes such conditions as the McLeod syndrome.
Occasionally, there may be obliteration of the ducts by fibrous tissue and varying amount of inflammation and is termed obliterative mastitis. M/E There is disruption of the regular pattern of lipocytes with formation of lipid-filled spaces surrounded by neutrophils, lymphocytes, plasma cells and histiocytes having foamy cytoplasm and frequent foreign body giant cell formation. The mammary duct is obstructed and dilated to form a thin-walled cyst filled with milky fluid. Its incidence has been reported to range from 10-20% in adult women, most often between 3rd and 5th decades of life, with dramatic decline in its incidence after menopause suggesting the role of oestrogen in its pathogenesis. As such, fibrocystic change of the female breast is a histologic entity characterised by following features: i) Cystic dilatation of terminal ducts. Presently, the spectrum of histologic changes is divided into two clinicopathologically relevant groups: A. The usual large cyst is rounded, translucent with bluish colour prior to opening (blue-dome cyst). Frequently, there is apocrine change or apocrine metaplasia in the lining of the cyst resembling the cells of apocrine sweat glands. Fibrosis There is increased fibrous stroma surrounding the cysts and variable degree of stromal lymphocytic infiltrate. The latter condition, lobular hyperplasia, must be distinguished from adenosis (discussed separately) in which there is increase in the number of ductules or acini without any change in the number or type of cells lining them. M/E Epithelial hyperplasia is characterised by epithelial proliferation to more than its normal double layer. In general, ductal hyperplasia is termed as epithelial hyperplasia of usual type and may show various grades of epithelial proliferations (mild, moderate and atypical) as under, while lobular hyperplasia involving the ductules or acini is always atypical. Mild hyperplasia of ductal epithelium consists of at least three layers of cells above the basement membrane, present focally or evenly throughout the duct. Moderate and florid hyperplasia of ductal type is associated with tendency to fill the ductal lumen with proliferated epithelium. Such epithelial proliferations into the lumina of ducts may be focal, forming papillary epithelial projections called ductal papillomatosis, or may be more extensive, termed florid papillomatosis, or may fill the ductal lumen leaving only small fenestrations in it. Of all the ductal hyperplasias, atypical ductal hyperplasia is more ominous and has to be distinguished from intraductal carcinoma. The proliferated epithelial cells in the atypical ductal hyperplasia partially fill the duct lumen and produce irregular microglandular spaces or cribriform pattern. Atypical lobular hyperplasia is closely related to lobular carcinoma in situ but differs from the latter in having cytologically atypical cells only in half of the ductules or acini. The lesion may be present as diffusely scattered microscopic foci in the breast parenchyma, or may form an isolated palpable mass. G/A the lesion may be coexistent with other components of fibrocystic disease, or may form an isolated mass which has hard cartilage-like consistency, resembling an infiltrating carcinoma. The histologic appearance may superficially resemble infiltrating carcinoma but differs from the latter in having maintained lobular pattern. Simple fibrocystic change or nonproliferative fibrocystic changes of fibrosis and cyst formation do not carry any increased risk of developing invasive breast cancer. Identification of general proliferative fibrocystic changes are associated with 1. Multifocal and bilateral proliferative changes in the breast pose increased risk to both the breasts equally. Within the group of proliferative fibrocystic changes, atypical hyperplasia in particular, carries 4 to 5 times increased risk to develop invasive breast cancer later. Since the male breast does not contain secretory lobules, the enlargement is mainly due to proliferation of ducts and increased periductal stroma. Such excessive oestrogenic activity in males is seen in young boys between 13 and 17 years of age (pubertal gynaecomastia), in men over 50 years (senescent gynaecomastia). G/A One or both the male breasts are enlarged having smooth glistening white tissue. Proliferation of branching ducts which display epithelial hyperplasia with formation of papillary projections at places. Though it can occur at any age during reproductive life, most patients are between 15 to 30 years of age.
Diseases
It may occur sporadically or be a part of von HippelLindau syndrome (along with cysts in the liver, kidney, and benign/malignant renal tumour). Thus, about a quarter haemangioblastomas secrete erythropoietin and cause polycythaemia. M/E the features are as under: i) Large number of thin-walled blood vessels lined by plump endothelium. G/A the tumour is frequently periventricular in location and may appear nodular or diffuse. M/E the features are as under: i) Characteristically, the tumour grows around blood vessels i. Some common examples of such tumours are germinoma (seminoma/dysgerminoma), teratoma and embryonal carcinoma. Their most common sites are in the front half of the head and include: lateral cerebral convexities, midline along the falx cerebri adjacent to the major venous sinuses parasagittally, and olfactory groove. Less frequent sites are: within the cerebral ventricles, foramen magnum, cerebellopontine angle and the spinal cord. They have an increased frequency in patients with neurofibromatosis 2 and are often multiple in these cases. They are usually found in 2nd to 6th decades of life, with slight female preponderance. G/A Meningioma is well-circumscribed, solid, spherical or hemispherical mass of varying size (110 cm in diameter). The tumour is generally firmly attached to the dura and indents the surface of the brain but rarely ever invades it. Cut surface of the tumour is firm and fibrous, sometimes with foci of calcification. Meningotheliomatous (syncytial) meningioma this pattern of meningioma resembles the normal arachnoid cap cells. The tumour consists of solid masses of polygonal cells with poorlydefined cell membranes. The cells have round to oval, central nuclei with abundant, finely granular cytoplasm. Fibrous (fibroblastic) meningioma A less frequent pattern is of a spindleshaped fibroblastic tumour in which the tumour cells form parallel or interlacing bundles. Transitional (mixed) meningioma this pattern is characterised by a combination of cells with syncytial and fibroblastic features with conspicuous whorled pattern of tumour cells, often around central capillary-sized blood vessels. Some of the whorls contain psammoma bodies due to calcification of the central core of whorls. Angioblastic meningioma An angioblastic meningioma includes 2 patterns: haemangioblastic pattern resembling haemangioblastoma of the cerebellum, and haemangiopericytic pattern which is indistinguishable from haemangiopericytoma elsewhere in the body. Anaplastic (malignant) meningioma Rarely, a meningioma may display features of anaplasia and invade the underlying brain or spinal cord. This pattern of meningioma is associated with extraneural metastases, mainly to the lungs. Most common primary tumours metastasising to the brain are: carcinomas of the lung, breast, skin (malignant melanoma), kidney and the gastrointestinal tract and choriocarcinoma. G/A the metastatic deposits in the brain are usually multiple, sharplydefined masses at the junction of grey and white matter. A less frequent pattern is carcinomatous meningitis or meningeal carcinomatosis in which there is presence of carcinomatous nodules on the surface of the brain and spinal cord, particularly encountered in carcinomas of the lung and breast. M/E Metastatic tumours in the brain recapitulate the appearance of the primary tumour of origin with sharp line of demarcation from adjoining brain tissue. A peripheral nerve is surrounded by an outer layer of fibrous tissue, the epineurium. Each nerve is made of several fascicles enclosed in multilayered membrane of flattened cells, the perineurium. Nodes of Ranvier on myelinated fibres are the boundaries between each Schwann cell surrounding the fibre. Following transection, initially there is accumulation of organelles in the proximal and distal ends of the transection sites. Subsequently, the axon and myelin sheath distal to the transection site undergo disintegration upto the next node of Ranvier, followed by phagocytosis.
Neutrophil, eosinophil, antibody (pre-existing), mast cell, and basophil mediated. Acute inflammation is rapid onset (seconds to minutes) and of short duration (minutes to days). Outcomes include complete resolution, abscess formation, or progression to chronic inflammation. Mononuclear cell (monocytes/macrophages, lymphocytes, plasma cells) and fibroblast mediated. Free radicals can be eliminated by scavenging enzymes (eg, catalase, superoxide dismutase, glutathione peroxidase), spontaneous decay, antioxidants (eg, vitamins A, C, E), and certain metal carrier proteins (eg, transferrin, ceruloplasmin). Pleural effusion is exudative if 1 of the following criteria is met: Pleural effusion protein/serum protein ratio > 0. Amyloid deposits visualized by Congo red stain A, polarized light (apple green birefringence) B, and H&E stain (C shows deposits in glomerular mesangial areas [white arrows], tubular basement membranes [black arrows]). Heterogeneous group of disorders, including familial amyloid polyneuropathies due to transthyretin gene mutation. Isolated atrial amyloidosis due to atrial natriuretic peptide is common in normal aging and can predispose to increased risk of atrial fibrillation. Autopsy of elderly person will reveal deposits in heart, colon, liver, kidney, eye, and other organs. May be a risk factor for future malignancy (eg, endometrial hyperplasia) but not considered premalignant. Causes include disuse, denervation, loss of blood supply, loss of hormonal stimulation, poor nutrition. Mild dysplasia is usually reversible; severe dysplasia usually progresses to carcinoma in situ. Reversible if the irritant is removed but may undergo malignant transformation with persistent insult (eg, Barrett esophagus esophageal adenocarcinoma). The degree to which a malignant tumor resembles its tissue of origin: Well-differentiated tumors (often less aggressive) closely resemble their tissue of origin. Poorly differentiated tumors (often more aggressive) look almost nothing like their tissue of origin. See cervical example A, which shows normal cells and spectrum of dysplasia, as discussed below. Dysplasia Abnormal proliferation of cells with loss of size, shape, and orientation (eg, koilocytic change, arrow in A). Carcinoma in situ/ preinvasive Neoplastic cells have not invaded the intact basement membrane. Invasive carcinoma Cells have invaded basement membrane using collagenases and hydrolases (metalloproteinases). Soil = target organ is often the first-encountered capillary bed (eg, liver, lungs, bone, brain, etc). Range from low grade (well differentiated) to high grade (poorly differentiated, undifferentiated or anaplastic). Example: cT3N1M0 Stage generally has more prognostic value than grade (eg, a high-stage yet low-grade tumor is usually worse than a low-stage yet high-grade tumor). Stage Tumor nomenclature Carcinoma implies epithelial origin, whereas sarcoma denotes mesenchymal origin. Benign tumors are usually well differentiated, well demarcated, low mitotic activity, no metastasis, no necrosis. Malignant tumors may show poor differentiation, erratic growth, local invasion, metastasis, and apoptosis. Terms for non-neoplastic malformations include hamartoma (disorganized overgrowth of tissues in their native location, eg, Peutz-Jeghers polyps) and choristoma (normal tissue in a foreign location, eg, gastric tissue located in distal ileum in Meckel diverticulum).
Instead of inserting an indent "tuberculous" under each anatomical site, the index uses one single indent "tuberculous see Tuberculosis, abscess" under the lead term "Abscess". Some special lead terms, or "key" words, are used for these, indicating the type of problem or circumstances. The main key words are "Counseling", "Examination", "History", "Observation", "Pregnancy", "Problem", "Screening", "Status", and "Vaccination". Some obstetric complications, especially the more common ones, can be found under the specific condition. More often, however, the complication will be listed under "Labor", "Pregnancy", "Puerperal", or "Maternal condition affecting fetus or newborn". Code numbers the code numbers that follow the terms in the Index are those of the three- or four-character categories to which the terms are classified. This indicates that a fourth character exists and should be used, and that it will be found either in a note in the Index. When a set of fourth characters is applicable to a group of categories, the common fourth characters may be presented in a note or, in the case of pregnancies with abortive outcome, in a table in order to facilitate their application to different types of complete or incomplete abortion and to molar pregnancies. In other cases, the complication or main manifestation is listed in the Index with a cross-reference to the entire group of categories, with specification of the fourth character. Where an index term is one of the diagnostic statements for which there is a dual classification according to etiology and manifestation (see Volume 2), both codes are given, the first followed by a dagger and the second by an asterisk (*). Multiple diagnoses the Tabular List includes a number of categories for the classification of two or more conditions jointly reported. Such combinations of conditions, which are specifically classified in the Tabular List, also appear in the Index. Classification rules for certain other combinations appear in Volume 2 in the section "Mortality: guidelines for certification and rules for coding" under the heading "Notes for use in underlying cause mortality coding". These provisions, since they are not inherent in the classification itself, are not indexed. Users familiar with the British form should remember that the first letter of the vowel combinations ae and oe and the u in words ending in -our have been dropped, and the "re" reversed to "er" in words ending thus. It is only when the initial letters are affected that any great displacement in alphabetical order is caused, and in this case, the word is usually also listed with the British spelling and a reference given to the American spelling, thus: "Oedema, oedematous see Edema". Conventions used in the Index Parentheses In the Index, as in the Tabular List, parentheses have a special meaning which the coder must bear in mind. A term that is followed by other terms in parentheses is classified to the given code number whether any of the terms in parentheses are reported or not. Cross-references Some categories, particularly those subject to notes linking them with other categories, require rather complex indexing arrangements. To avoid repeating this arrangement for each of the inclusion terms involved, a cross-reference is used. On looking up the latter term, the coder will find listed various forms of osteomyelitis: acute, acute hematogenous, chronic, etc. There alternative codes will be found for the condition if further or otherwise qualified as, for example, due to drugs or syphilitic. Enlargement, enlarged see also Hypertrophy If the coder does not find the site of the enlargement among the indentations beneath "Enlargement", he or she should look among the indentations beneath "Hypertrophy" where a more complete list of sites is given. Bladder see condition Hereditary see condition As stated previously, anatomical sites and very general adjectival modifiers are not usually used as lead terms in the Index and the coder is instructed to look up the disease or injury reported on the medical record and under that term to find the site or adjectival modifier. For other abdominal conditions, the coder should look up the disease or injury reported.
Primary tubular diseases that include tubular injury by ischaemic or toxic agents i. Tubulointerstitial diseases that include inflammatory involvement of the tubules and the interstitium i. Shock (post-traumatic, surgical, burns, dehydration, obstetrical and septic type). Non-traumatic rhabdomyolysis induced by alcohol, coma, muscle disease or extreme muscular exertion (myoglobinuric nephrosis). M/E Predominant changes are seen in the tubules, while glomeruli remain unaffected. Eosinophilic hyaline casts or pigmented haemoglobin and myoglobin casts in the tubular lumina. Disruption of tubular basement membrane adjacent to the cast may occur (tubulorrhexis). In general, cases that follow severe trauma, surgical procedures, extensive burns and sepsis have much worse outlook than the others. General poisons such as mercuric chloride, carbon tetrachloride, ethylene glycol, mushroom poisoning and insecticides. Drugs such as sulfonamides, certain antibiotics (gentamycin, cephalosporin), anaesthetic agents (methoxyflurane, halothane), barbiturates, salicylates. Epithelial cells of mainly proximal convoluted tubules are necrotic and desquamated into the tubular lumina. The regenerating epithelium, which is flat and thin with few mitoses, may be seen lining the tubular basement membrane. The bacteria gain entry into the urinary tract, and then into the kidney by one of the two routes: 1. The common pathogenic organisms are inhabitants of the colon and may cause faecal contamination of the urethral orifice, especially in females in reproductive age group. Ascending infection may occur in a normal individual but the susceptibility is increased in patients with diabetes mellitus, pregnancy, urinary tract obstruction or instrumentation. After having caused urethritis and cystitis, the bacteria in susceptible cases ascend further up into the ureters against the flow of urine, extend into the renal pelvis and then the renal cortex. The role of vesico-ureteral reflux is not a significant factor in the pathogenesis of acute pyelonephritis as it is in chronic pyelonephritis. Haematogenous infection Less often, acute pyelonephritis may result from blood-borne spread of infection. This occurs more often in patients with obstructive lesions in the urinary tract, and in debilitated or immunosuppressed patients. G/A Well-developed cases of acute pyelonephritis show enlarged and swollen kidney that bulges on section. M/E Acute pyelonephritis is characterised by extensive acute inflammation involving the interstitium and causing destruction of the tubules. Generally, the glomeruli and renal blood vessels show considerable resistance to infection and are spared. The acute inflammation may be in the form of large number of neutrophils in the interstitial tissue and bursting into tubules, or may form focal neutrophilic abscesses in the renal parenchyma. Papillary necrosis Papillary necrosis or necrotising papillitis develops more commonly in analgesic abuse nephropathy and in sickle cell disease but may occur as a complication of acute pyelonephritis as well. Pyonephrosis Rarely, the abscesses in the kidney in acute pyelonephritis are extensive, particularly in cases with obstruction. This results in inability of the abscesses to drain and this transforms the kidney into a multilocular sac filled with pus. Perinephric abscess the abscesses in the kidney may extend through the capsule of the kidney into the perinephric tissue and form perinephric abscess. Refluxnephropathy Reflux of urine from the bladder into one or both the ureters during micturition is the major cause of chronic pyelonephritis.
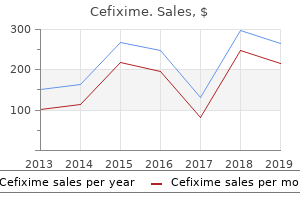
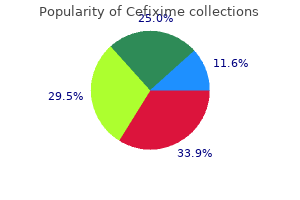
Casein-derived peptide (Casein Peptides). Cefixime.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97053
Young children from 1-4 years are exposed to higher risk of sustaining injuries, and manifest certain congenital anomalies. Older children from 5-14 years too have higher risk of injuries from accidents and have other problems related to congenital anomalies and certain malignant tumours at this age. Benign tumours are more common than malignant neoplasms but they are generally of little immediate consequence. Many other tumours originate in abnormally developed organs and organ rests; (embryonic tumours). In embryonic tumours, proliferation of embryonic cells occurs which have not reached the differentiation stage essential for specialised functions i. Tumours of infancy and childhood have some features of normal embryonic or foetal cells in them which proliferate under growth promoting influenceofoncogenes. Under appropriate conditions, these malignant embryonal cells may cease to proliferate and transform into non-proliferating mature differentiated cells. Hamartomas Hamartomas are focal accumulations of cells normally present in that tissue but are arranged in an abnormal manner. Choristoma (heterotopia) Choristoma or heterotopia is collection of normal cells and tissues at aberrant locations. Children between 5 to 9 years of age: haematopoietic malignancies are more common. In the age range of 10-14 years (prepubertal age): soft tissue and bony sarcomas are the prominent tumours. For chromosomal study, the dividing cells are arrested by colchicine in the following phase of cell cycle: A. Denver classification divides chromosomes based on their length into the following groups: A. Out of the following glycogenosis, the following is example of 155 lysosomal storage disease: A. Conventionally, it includes study of constituents of circulating blood and blood-forming organs. Based on these modifications in classification systems, the section on diseases of blood, bone marrow and lymphoreticular tissues has been structured into three chapters: introduction to haematopoietic system and disorders of erythroid series (Chapter 10), disorders of platelets, bleeding disorders and basic transfusion medicine (Chapter 11) and disorders of leucocytes (myeloid and lymphoid series) and diseases of lymphoreticular tissues (Chapter 12). Circulating blood normally contains 3 main types of mature blood cells-the red cells (erythrocytes), the white cells (leucocytes) and the platelets (thrombocytes). These blood cells perform their respective major physiologic functions: erythrocytes largely concerned with oxygen transport, leucocytes play various roles in body defense against infection and tissue injury, while thrombocytes are primarily involved in maintaining integrity of blood vessels and in preventing blood loss. By about 3rd month, however, the liver and spleen are the main sites of blood cell formation and continue to do sountilabout2weeksafterbirth. Haematopoiesiscommencesinthebone marrow by 4th and 5th month and becomes fully active by 7th and 8th month so that at birth practically all the bones contain active marrow. During normal childhood and adult life, therefore, the marrow is the only source of new blood cells. However, during childhood, there is progressive fatty replacement throughout the long bones so that by adult life the haematopoietic marrow is confined to the central skeleon (vertebrae, sternum, t ribs, skull, sacrum and pelvis) and proximal ends of femur, tibia and humerus. Monocytes on entering the tissues form a variety of phagocytic macrophages, both of which together constitute mononuclearphagocyte system. Haematopoiesis or myelopoiesis is regulated by certain endogenous glycoproteinscalledhaematopoieticgrowthfactors,cytokinesandhormones. Smears are prepared immediately from the bone marrow aspirate and are fixed in 95% methanol after airdrying. The usual Romanowsky technique is emplo ed for staining and a y stain for iron is performed routinely so as to assess the reticuloendothelial stores of iron. The marrow film provides assessment of cellularity, details of developing blood cells. Thetissueisthenfixed,softdecalcifiedandprocessed for histological sections and stained with haematoxylin and eosin and for reticulin. Red cell production is influenced by growth factors and hormones, notably erythropoietin. The principal site of erythropoietin productionisthekidneythoughthereisevidenceofitsextra-renalproduction in certain unusual circumstances.
Urease produces ammonia, creating an alkaline environment, which helps H pylori survive in acidic mucosa. Colonizes mainly antrum of stomach; causes gastritis and peptic ulcers (especially duodenal). Most common initial treatment is triple therapy: Amoxicillin (metronidazole if penicillin allergy) + Clarithromycin + Proton pump inhibitor; Antibiotics Cure Pylori. Only Borrelia can be visualized using aniline dyes (Wright or Giemsa stain) in light microscopy due to size. Leptospira interrogans Spirochete with hook-shaped ends found in water contaminated with animal urine. Leptospirosis-flu-like symptoms, myalgias (classically of calves), jaundice, photophobia with conjunctival suffusion (erythema without exudate). Weil disease (icterohemorrhagic leptospirosis)-severe form with jaundice and azotemia from liver and kidney dysfunction, fever, hemorrhage, and anemia. Lyme disease A B Caused by Borrelia burgdorferi, which is transmitted by the Ixodes deer tick A (also vector for Anaplasma spp. Stage 1-early localized: erythema migrans (typical "bulls-eye" configuration B is pathognomonic but not always present), flu-like symptoms. If available, use dark-field microscopy to visualize treponemes in fluid from chancre B. Disseminated disease with constitutional symptoms, maculopapular rash C (including palms D and soles), condylomata lata E (smooth, moist, painless, wart-like white lesions on genitals), lymphadenopathy, patchy hair loss; also confirmable with dark-field microscopy. To prevent, treat mother early in pregnancy, as placental transmission typically occurs after first trimester. Quantitative, inexpensive, and widely available test for syphilis (sensitive but not specific). Campylobacter Chlamydophila psittaci Coxiella burnetii Ehrlichia chaffeensis Francisella tularensis Leptospira spp. Mycobacterium leprae Pasteurella multocida Rickettsia prowazekii Rickettsia rickettsii Rickettsia typhi Salmonella spp. Presents as a gray vaginal discharge with a fishy smell; nonpainful (vs vaginitis). Bacterial vaginosis is also characterized by overgrowth of certain anaerobic bacteria in vagina. Clue cells (vaginal epithelial cells covered with Gardnerella) have stippled appearance along outer margin (arrow in A). Despite its name, disease occurs primarily in the South Atlantic states, especially North Carolina. Rash typically starts at wrists A and ankles and then spreads to trunk, palms, and soles. Reticulate body Replicates in cell by fission; Reorganizes into elementary bodies. Chlamydophila pneumoniae and Chlamydophila psittaci cause atypical pneumonia; transmitted by aerosol. Treatment: azithromycin (favored because onetime treatment) or doxycycline (+ ceftriaxone for possible concomitant gonorrhea). The chlamydial cell wall lacks classic peptidoglycan (due to reduced muramic acid), rendering -lactam antibiotics ineffective. Lymphogranuloma venereum-small, painless ulcers on genitals swollen, painful inguinal lymph nodes that ulcerate (buboes). Types L1, L2, and L3 Mycoplasma pneumoniae A Classic cause of atypical "walking" pneumonia (insidious onset, headache, nonproductive cough, patchy or diffuse interstitial infiltrate). Treatment: macrolides, doxycycline, or fluoroquinolone (penicillin ineffective since Mycoplasma have no cell wall). Treatment: fluconazole or itraconazole for local infection; amphotericin B for systemic infection. Three varieties: Interdigital E; most common Moccasin distribution F Vesicular type Onychomycosis; occurs on nails. Degradation of lipids produces acids that damage melanocytes and cause hypopigmented G, hyperpigmented, and/or pink patches.
These are, of course, delicate areas, but, if approached in a straightforward and non-judgmental way, it is remarkable how forthcoming, and indeed relieved, some patients may be at being given an opportunity to speak of them. Most patients will require, however, either encouragement or some gentle shepherding at various times. If asked whether they have anything else to add, many patients will offer important information that they may have either withheld or simply not recalled earlier. Should patients remain uncooperative, it may at times be possible to infer their cognitive status indirectly; for example, during history taking, by asking the date of a recent event brought up by the patient. As noted below, abnormalities on the mental status examination typically indicate the presence of one of the major syndromes, such as dementia (Section 5. This is especially the case when patients are confused or suffer from poor memory: it is remarkable how often a collateral history will change a diagnostic impression, guide further testing or alter proposed treatments. Inquiry should also be made regarding hobbies, such as playing cards or chess, or doing crossword puzzles. In cases characterized by cognitive deficits, the loss of these abilities may serve to establish the onset of the current illness. Some have expressed concern that interviewing the family or acquaintances may violate patient confidentiality but this is simply not the case, provided that the contact knows already that the patient is in the hospital and that the physician reveals nothing about the patient while interviewing the collateral contact. This is sometimes a tedious task but, as with interviewing collateral sources, it may reveal critical information. Grooming and dress Good habits of grooming and dress may suffer in certain illnesses, sometimes with diagnostically suggestive results. Depressive patients may find that hopelessness, fatigue, and anhedonia make them give up all hope of maintaining their appearance, with the result that grooming and dress are left in a greater or lesser degree of disarray. Manic patients, overflowing with exuberance, may truly make a spectacle of themselves with decorations of make-up and garish clothing. Rarely, one may see evidence of neglect wherein dress and grooming suffer on only one side of the body (Section 2. Comments should be made on the relationship of the patient to the interviewer, noting, for example, whether the patient is cooperative or uncooperative, guarded, evasive, hostile, or belligerent. For example, as noted by Bleuler (1924), in schizophrenia, there is often a `defect in. Many of these may be determined during the non-directive portion of the interview; however, some, especially those concerning cognition. Psychomotor retardation may range from an almost total quietude and immobility to a mere slowing of speech and behavior. Mere exhaustion may slow patients down, but the response to rest is generally robust. Apathetic patients, lacking in motivation, may evidence little speech or behavior; depressed patients may appear similar but here one also sees a depressed mood. Delirium may be characterized by quietude and inactivity but is distinguished by the presence of confusion and deficits in memory and orientation. Other behavioral disturbances may occur during the interview and examination, including mannerisms, stereotypies, and echopraxia. Mannerisms represent more or less bizarre transformations of speech, gesture, or other behaviors (Section 4. Stereotypies are a kind of perseveration wherein patients repeatedly engage in the same behaviors, to no apparent purpose (Section 4. Echopraxia is said to be present when patients involuntarily mimic what others, such as the examining physician, do (Section 4. Anxious patients are beset with apprehensions, may plead for help, and may complain of tremor and palpitations. Affect has been variously defined as representing either the combination of the immediately present emotion and its accompanying expression in tone of voice, gesture, facial expression, etc. Given that, as with mood, affect may be depressed, euphoric, anxious, or irritable it may appear academic to distinguish between the two; however, disparities between mood and affect may arise. Mood is enduring, whereas affect is relatively changeable: in a sense, mood is to climate p 01. Affect, in addition to being depressed, euphoric, anxious or irritable, may also be flattened or labile. Some investigators believe flattened affect is also present in severe depression; however, in my experience there is little difficulty in distinguishing a flattened from a depressed affect.
This image is a derivative work, adapted from the following source, available under: Immunofluorescence of acute poststreptococcal glomerulonephritis. The role of nephritis-associated plasmin receptor (naplr) in glomerulonephritis associated with streptococcal infection. This image is a derivative work, adapted from the following source, available under: Hakim W, Sherman R, Rezk-MACROS-, et al. Membranoproliferative glomerulonephritis with "tram tracks" appearance on H&E stain. This image is a derivative work, adapted from the following source, available under: Ahmadi F, Zafarani F, Haghighi H, et al. This image is a derivative work, adapted from the following source, available under: M. Hereditary papillary renal cell carcinoma primarily diagnosed in a cervical lymph node: a case report of a 30-year-old woman with multiple metastases. This image is a derivative work, adapted from the following source, available under: Refaie H, Sarhan M, Hafez A. This image is a derivative work, adapted from the following source, available under: Geavlete B, Stanescu F, Moldoveanu C, et al. Improving inter-observer variability in the evaluation of ultrasonographic features of polycystic ovaries. This image is a derivative work, adapted from the following source, available under: Katoh-MACROS-, Yasuda M, Hasegawa K, et al. This image is a derivative work, adapted from the following source, available under: Costarelli L, Campagna D, Mauri M, et al. Intraductal proliferative lesions of the breast-terminology and biology matter: premalignant lesions or preinvasive cancer This image is a derivative work, adapted from the following source, available under: Montesinos L, Acien P, Martinez-Beltran M, et al. This image is a derivative work, adapted from the following source, available under: Muttarak M, Siriya B, Kongmebhol P, et al. This image is a derivative work, adapted from the following source, available under: Hic et nunc. This image is a derivative work, adapted from the following source, available under: Zhou X-C, Zhou, Ye Y-H, et al. This image is a derivative work, adapted from the following source, available under: Franceschini G, Manno A, Mule A, et al. Gastro-intestinal symptoms as clinical manifestation of peritoneal and retroperitoneal spread of an invasive lobular breast cancer: report of a case and review of the literature. Ovarian dysgerminoma and synchronic contralateral tubal pregnancy followed by normal intra-uterine gestation: a case report. This image is a derivative work, adapted from the following source, available under: Leonardi S, Barone P, Gravina G, et al. This image is a derivative work, adapted from the following source, available under: Fehrenbach H, Tews S, Fehrenbach A, et al. Improved lung preservation relates to an increase in tubular myelin-associated surfactant protein A. This image is a derivative work, adapted from the following source, available under: Gokhale S. This image is a derivative work, adapted from the following source, available under: Courtesy of Dr. This image is a derivative work, adapted from the following source, available under: Bai C, Huang H, Yao X, et al. This image is a derivative work, adapted from the following source, available under: Strek P, Zagolski O, Sktadzien J. This image is a derivative work, adapted from the following source, available under: Oikonomou A, Prassopoulo P. This image is a derivative work, adapted from the following source, available under: Toshikazu A, Takeoka H, Nishioka K, et al. Successful management of refractory pleural effusion due to systemic immunoglobulin light chain amyloidosis by vincristine adriamycin dexamethasone chemotherapy: a case report.
References:




