A mental status examination is crucial in identifying signs of depression, associated psychosis, cognitive deficits, and factors influencing suicide risk. Because major depressive disorder is associated with functional impairment, the presence, type, and severity of the dysfunction should be evaluated. Impairments can include deficits in interpersonal relationships and family functioning, work performance, maintenance of health and hygiene, and deficits in quality of life. A family history is also important to obtain and involves the collection of the family pedigree including parents, grandparents, and number and sex of siblings and children. For patients with children at home, information on their symptom state may be useful because of the high possibility of psychiatric problems in the offspring of a depressed parent (11, 12). Such problems may require intervention or may be an added stressor for the patient. In establishing a diagnosis of major depressive disorder as part of the initial assessment, other differential diagnostic possibilities are important to consider. An initial consideration in the differential diagnosis is mood disorder due to a general medical condition. Specific medical conditions that are important to consider and that may be associated with a major depressive episode include neurological conditions. Depressive symptoms that would otherwise be diagnosable as major depressive disorder are diagnosed instead as a mood disorder due to a general medical condition if the mood disturbance is judged to be the direct physiological consequence of a specific general medical condition. Similarly, medications used to treat general medical conditions may induce depressive syndromes. Such medications include transplant anti-rejection agents, chemotherapy agents, interferon, steroids, some antibiotics, and others. Psychosocial stressors and other antecedent events, and their possible contribution to the generation of depressive symptoms, should be explored in the course of a psychiatric assessment. Depressive symptoms are a common response to psychosocial stressors, particularly bereavement. Following a stressor, depressive symptoms that do not reach sufficient number or severity to be classified as a major depressive episode may be better described as an adjustment disorder. Despite the possible presence of antecedent stressors, psychiatrists should not dismiss potentially disabling depressive symptoms as "normal," thereby depriving patients of needed therapeutic attention. A thorough assessment of depression also includes the evaluation of psychotic symptoms. Major depressive disorder may be associated with mood-congruent and moodincongruent hallucinations and delusions. Depressed patients may not initially present with psychotic symptoms, and patients may wish to hide shaming or distressing thoughts. This distinction is especially important because the treatments for bipolar disorders often differ from those for major depressive disorder. All patients who present for treatment for a major depressive episode should be screened for a past history of manic or hypomanic episodes and for past adverse reactions to antidepressants that might be consistent with a "switch" into hypomania or mania. However, since patients are often unaware of prior hypomanic or manic episodes, even when questioned carefully, collateral sources of information, such as family members living with the patient, may be crucial in uncovering such episodes. Clinical assessment should also include whether or not the patient is experiencing a mixed episode, which is characterized by symptoms of both a major depressive episode and a manic episode that occur nearly every day for at least 1 week. It is also important to consider the frequency and chronicity of prior episodes of major depressive disorder. Practice Guideline for the Treatment of Patients With Major Depressive Disorder, Third Edition Chronic forms of depression-such as dysthymic disorder, "double depression" (dysthymic disorder and major depressive disorder), and major depressive disorder with the "chronic" specifier-are all depressions with a duration of at least 2 years. In clinical studies, chronic depression has a lower response rate than nonchronic depression, but because the placebo-response rate is also lower, the relative clinical benefit is comparable. The onset of benefit in chronic depression appears more gradual than in nonchronic depression. However, despite a smaller response rate and slower response, it is important to recognize that chronic depression is not treatment refractory (20). Unfortunately, however, in many patients, chronic depression remains undiagnosed or, if diagnosed, undertreated (21). Family histories of major depressive disorder and bipolar disorder are common in those with major depressive disorder, but a family history of bipolar disorder may indicate increased risk of bipolar disorder in the patient. Evaluate the safety of the patient Addressing safety concerns may take precedence over establishing a full differential diagnosis or completing the psychiatric assessment.
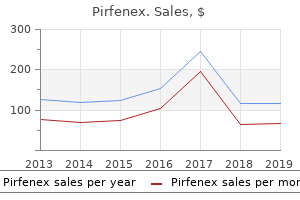
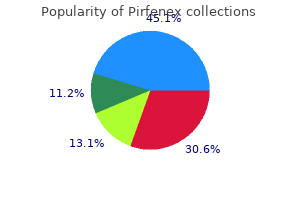
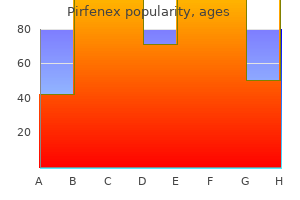
Bishopsweed (Goutweed). Pirfenex.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96072
Text Content the text of each disorder has been developed in a standardized manner to ensure the comprehensiveness of descriptions and consistency among sections. Sex Ratio this section includes the relative frequency with which the disorder is diagnosed in each sex. The presence of a disorder in several family members, however, does not necessarily mean that the disorder has a genetic basis. Pathology this section describes, if known, the gross or microscopic pathologic features of the disorder. Associated Features this section contains those features that are often but not invariably present. Complications this section includes other disorders or events that may develop during the course of the disorder. Information may be presented on the number of nights of polysomnographic recording required for diagnosis and whether certain special conditions are necessary for appropriate interpretation of the polysomnographic results. Prevalence this section presents the prevalence of the specific sleep disorder, if the prevalence is known. For some disorders, the exact prevalence is unknown, and only the prevalence of the underlying medical disorder can be stated. Other Laboratory Features this section describes features of laboratory tests, other than polysomnographic procedures, that aid in either establishing the diagnosis or eliminating other disorders that may have a similar presentation. Diagnostic criteria were considered by the classification committee to be helpful not only for clinical but also for research purposes. The final assignment of a particular diagnosis depends upon clinical judgment, and the criteria do not exclude those disorders in which there may be variability of the clinical features. These criteria should provoke discussion and appropriate clinical testing in field trials to refine and enhance their diagnostic reliability. As with the diagnostic and severity criteria, future research will refine the duration criteria. Classic articles from a variety of authors and sources have been selected, and the number of abstracts and review articles is limited. Minimal Criteria the minimal criteria aid in the early diagnosis of a sleep disorder, usually before diagnostic testing. The minimal criteria usually are dependent upon the available patient history and clinical features. Objective testing is included in the minimal criteria when it is essential to define a disorder. The purpose of this database is to establish a format for epidemiologic tracking of sleep disorders at sleep disorders centers. As with the diagnostic criteria, ongoing research will refine the severity criteria. The subgroups are partly descriptive and suggest a diagnosis from information available at initial presentation. The bibliography is not exhaustive and includes only books of classic importance or that provide current, additional clinical information. The American Medical Association has published a list of the names and appropriate procedure-code numbers of services and procedures performed by physicians. This list of code numbers is particularly useful for reimbursement coding purposes. This list assists the clinician in finding the appropriate code number for a specific sleep disorder. This list aids the clinician familiar with the 1979 classification in finding the new terminology and code numbers. Additional codes are included for procedures and physical signs of particular interest to sleep disorders clinicians and researchers. The diagnoses and code numbers are listed in order of clinical importance to the patient. This classification is not intended to provide a differential diagnostic listing of sleep and arousal disorders.
In the guideline summary recommendation section, each recommendation is accompanied by itslevelofevidence:standard,guideline,option,orconsensus based. The development of these recommendations and their appropriate use are described below. Consensus-based recommendations reflect the shared judgment of the committee members and reviewers, based on the literature and common clinical practice of topic experts, and weredevelopedusingamodifiednominalgrouptechnique. Using a face-to-face meeting, voting sur489 I nsomnia symptoms occur in approximately 33% to 50% of theadultpopulation;insomniasymptomswithdistressorimpairment(generalinsomniadisorder)in10%to15%. Consistent risk factors for insomnia include increasing age, female sex, comorbid (medical, psychiatric, sleep, and substance use) disorders, shift work, and possibly unemployment and lower socioeconomicstatus. Inthisguideline, an insomnia disorder is defined as a subjective report of difficultywithsleepinitiation,duration,consolidation,orquality that occurs despite adequate opportunity for sleep, and that Journal of Clinical Sleep Medicine, Vol. Acomplaintofdifficultyinitiatingsleep,difficultymaintainAcomplaintofdifficultyinitiatingsleep,difficultymaintain ing sleep, or waking up too early, or sleep that is chronically nonrestorative or poor in quality. Itreflects the state of knowledge at the time of publication and will be reviewed, updated, and revised as new information becomes available. In this guideline, an insomniadisorderisdefinedasasubjectivereportofdifficulty with sleep initiation, duration, consolidation, or quality that occurs despite adequate opportunity for sleep, and that result in someformofdaytimeimpairment(Table2). Exceptwhereotherwisenoted,theword"insomnia"refersto an insomnia disorder in this guideline. Insomnia disorders have been categorized in various ways in differentsleepdisorderclassificationsystems. Insomnia complaints may also occur in association with comorbid disorders or other sleep disorder categories, such as sleep related breathing disorders, circadian rhythm sleep disorders, and sleep related movement disorders. Epidemiology Insomnia occurs in individuals of all ages and races, and has been observed across all cultures and countries. Insomniasymptomsoccurinapproximately33% to 50% of the adult population; insomnia symptoms with distressorimpairment(i. Patients with comorbid medical and psychiatric conditions are at particularly increased risk, with psychiatric and chronicpaindisordershavinginsomniaratesashighas50%to 75%. Tominimize individual expert bias, the group anonymously voted and ratedconsensusrecommendationsfrom1:stronglydisagreeto 9:stronglyagree. If consensus was not evident after thefirstvote,theconsensusrecommendationswerediscussed again, amended as appropriate, and a second anonymous vote was conducted. If consensus was not evident after the second vote, the process was repeated until consensus was attained to include or exclude a recommendation. Clinicalguidelinesprovideclinicianswitha working overview for disease or disorder evaluation and management. These guidelines include practice parameter papers and also include areas with limited evidence in order to provide acomprehensivepracticeguideline. Theyshouldnot,however,be considered exhaustive, inclusive of all available methods of care, or exclusive of other methods of care reasonably expected to obtain the same results. The ultimate judgment regarding appropriateness of any specific therapy must be made by the clinician and patient in light of the individual circumstances presented by the patient, available diagnostic tools, accessible Journal of Clinical Sleep Medicine, Vol. Although details of current models are beyond the scope of this practice guideline, general model concepts are critical for identifying biopsychosocial predisposing factors (such as hyperarousal, increased sleep-reactivity, or increased stress response), precipitatingfactors,andperpetuatingfactorssuch as(1)conditionedphysicalandmentalarousaland(2)learned negative sleep behaviors and cognitive distortions. In particular,identificationofperpetuatingnegativebehaviorsandcognitive processes often provides the clinician with invaluable information for diagnosis as well as for treatment strategies. In contrast to evolving models and diagnostic classifications for insomnia, procedures for clinical evaluation have remained relatively stable over time. Evaluation continues to rest on a careful patient history and examination that addresses sleep and wakingfunction(Table4),aswellascommonmedical,psychiatric, and medication/substance-related comorbidities (Tables 5,6,and7). The Primary Complaint: Patients with insomnia may complainofdifficultyfallingasleep,frequentawakenings,difficultyreturningtosleep,awakeningtooearlyinthemorning, or sleep that does not feel restful, refreshing, or restorative. Although patients may complain of only one type of symptom, it is common for multiple types of symptoms to co-occur, and for thespecificpresentationtovaryovertime. Keycomponentsincludecharacterizationofthecomplainttype,duration(months, years,lifetime),frequency(nightsperweekornumberoftimes pernight),severityofnighttimedistressandassociateddaytime symptomatology,course(progressive,intermittent,relentless), factors which increase or decrease symptoms, and identification of past and current precipitants, perpetuating factors, treatments, and responses. Pre-Sleep Conditions: Patients with insomnia may develop behaviors that have the unintended consequence of perpetuating their sleep problem. These behaviors may begin as strategies to combat the sleep problem, such as spending more timeinbedinaneffortto"catchup"onsleep.
Evidence for other clinically relevant interactions appears to be generally lacking. For information on the interactions of flavonoids, see under flavonoids, page 186, and for the interactions of resveratrol, see under resveratrol, page 335. The author suggests that grapeseed therefore has the potential to cause interactions. Furthermore, a study in rats suggests that grapeseed extract does not G 239 240 Grapeseed Grapeseed + Ascorbic acid (Vitamin C) the concurrent use of grapeseed and ascorbic acid (vitamin C) appears to increase systolic and diastolic blood pressure. Clinical evidence A placebo-controlled study in 69 hypertensive patients taking one or more antihypertensive medications investigated the effects on cardiovascular parameters of vitamin C 250 mg twice daily, grapeseed polyphenols 500 mg twice daily, or a combination of the two, for 6 weeks. However, treatment with the combination of vitamin C and polyphenols increased systolic blood pressure by 4. Endothelium-dependent and -independent vasodilatation, and markers of oxidative damage were not significantly altered. Importance and management Evidence is limited to one study, with no supporting mechanism to explain the effects seen, and so an interaction between vitamin C and grapeseed extract is not established. The authors of this study suggest that caution should be used when advising patients with hypertension on taking a combination of vitamin C and grapeseed. However, the general importance of any interaction is difficult to assess as the effect of taking these two supplements together is likely to vary depending on the patient and the degree to which their hypertension is controlled. It may be prudent to question a patient with poorly controlled blood pressure to establish if they are taking supplements containing both vitamin C and grapeseed, and discuss the option of stopping them to see if this improves their blood pressure control. The combination of vitamin C and grape-seed polyphenols increases blood pressure: a randomized, doubleblind, placebo-controlled trial. Grapeseed + Midazolam the interaction between grapeseed and midazolam is based on experimental evidence only. Experimental evidence In a study in rats, a single dose of an aqueous grapeseed extract had no significant effects on the pharmacokinetics of midazolam. However, after one week of treatment, grapeseed extract increased the elimination rate of midazolam by about 30%, and reduced its half-life by 28%. Some in vitro studies support this suggestion, although stronger effects may occur if the catechin content is high, see Pharmacokinetics, page 239. Importance and management Clinical evidence regarding an interaction between grapeseed and midazolam appears to be lacking. However, evidence from rat studies suggests that a clinically relevant interaction is unlikely and therefore no dose adjustments of midazolam are likely to be needed if grapeseed extract is also taken. Nishikawa M, Ariyoshi N, Kotani A, Ishii I, Nakamura H, Nakasa H, Ida M, Nakamura H, Kimura N, Kimura M, Hasegawa A, Kusu F, Ohmori S, Nakazawa K, Kitada M. Effects of continuous ingestion of green tea or grape seed extracts on the pharmacokinetics of midazolam. In Chinese medicine it has been used as an antitussive, anti-inflammatory and detoxicant. However, information on the safety and toxicity of greater celandine is limited: hepatotoxic effects, including severe hepatitis, severe cholestasis and fibrosis, have been reported with long-term use (one month or more). Pharmacokinetics No relevant pharmacokinetic data for greater celandine found, but see berberine, page 58, for details on this constituent of greater celandine. Constituents All parts of the plant contain benzylisoquinoline alkaloids, including berberine, chelerythrine, chelidonine, coptisine, cryptopine, protopine and sanguinarine. Use and indications Greater celandine has been traditionally used in the treatment of jaundice, gallbladder and biliary diseases, and eczema and G 241 Ground ivy Glechoma hederacea L. Use and indications Ground ivy is used as a mild expectorant for chronic bronchial catarrh. It is also said to be astringent, and therefore used for wound healing, haemorrhoids, gastritis and diarrhoea. Constituents Ground ivy contains flavonoids including isoquercitrin, luteolin diglucoside and rutin, and other polyphenolic compounds such as glycosides of icariol, cistanoside E and rosmarinic acid. Other compounds present include -sitosterol, the triterpenes oleanolic acid, and - and -ursolic acids, and a volatile oil containing the monoterpenes p-cymene, linalool, limonene and terpineol, among others.
A high Modified Mallampati score (Class 3 or 4) is associated with more difficult intubation as well as a higher incidence of sleep apnea. Physical examination: Mallampati score as an independent predictor of obstructive sleep apnea. A systematic review (metaanalysis) of the accuracy of the Mallampati tests to predict the difficult airway. The test is a list of eight situations where you rate your tendency to become sleepy on a scale of 0, no chance of dozing, to 3, high chance of dozing. Adapted from: Friedman M: Friedman tongue position and the staging of obstructive sleep apnea/hypopnea syndrome; in: Scheidt S, Clansey N, eds. High level of sleepiness suggestive of significance sleep disorder A score above 10 suggests excessive daytime sleepiness and should be discussed with a sleep specialist. Tonsil grades 1 and 2 comprise the small tonsil group, while grades 3 and 4 comprised the big tonsil group. Pediatr Clin North Am 1989;36(6):1551-69 18 Appendix 9 19 Appendix 9 Friedman Tonsil Grading System. In the Friedman grading scale, the tonsil size is classified on the basis of the location of the tonsil in relation to its surrounding structures in the oral cavity. Based on your unique breathing patterns, the system delivers mild stimulation to key airway muscles, which keeps the airway open during sleep. Using the small handheld sleep remote, simply turn Inspire therapy on at night before bed and off in the morning when you wake up. Here are some reasons people like you have chosen Inspire therapy to treat their sleep apnea. Concerns about sleep deprivation and lack of oxygen during sleep, which may cause short- and longterm health risks. If you want to check on the progress of your insurance approval, you can call (844) 515-6182. Risks associated with the surgical implant procedure are low but may include infection and temporary tongue weakness. Most patients acclimate well to the presence of the Inspire system and to the therapeutic stimulation. Sleep Disorders Many people experience problems sleeping including not getting enough sleep, not feeling rested and not sleeping well. In addition to affecting sleep itself, many medical and mental health conditions can be worsened by sleeprelated problems. Insomnia is an inability to get the amount of sleep needed to function efficiently during the daytime. Insomnia is rarely an isolated medical or mental illness but rather a symptom of another illness to be investigated by a person and their medical doctors. A doctor or sleep specialist can diagnose sleep apnea and provide treatment to improve sleep. Early morning wakefulness can be a sign of depression, along with low energy, inability to concentrate, sadness and a change in appetite or weight. While alcohol is sedating in limited quantities, intoxication with alcohol can make you wake up numerous times in the night and disturbs your sleep patterns. Poor sleep has been shown to significantly worsen the symptoms of many mental health issues. Treatment the first-line treatment for insomnia is good sleeping habits and taking care of any underlying conditions that may be causing the problems with sleeping. Sleep Apnea Therapy Software User Manual Page ii Sleep Apnea Therapy Software User Manual Notices Revised Notice Trademark Copyright Sleep Apnea Therapy Software User Manual 103392 Rev C Published May, 2017 and supersedes all previous versions. Somnetics and Transcend are registered trademarks of Somnetics International, Inc.

Amputated body parts should be transported with patient for possible re-implantation a. Frequency that weight or length-based estimate are documented in kilograms o Trauma-01: Pain assessment of injured patients. An evidence-based prehospital guideline for external hemorrhage control: American College of Surgeons Committee on Trauma. Prehospital control of life-threatening truncal and junctional haemorrhage is the ultimate challenge in optimizing trauma care: a review of treatment options and their applicability in the civilian trauma setting. A multi-institutional study of hemostatic gauze and tourniquets in rural civilian trauma. A systematic review of the use of tourniquets and topical haemostatic agents in conflicts in Afghantistan and Iraq. Advanced hemostatic dressings are not superior to gauze for care under fire scenarios. Revision Date September 8, 2017 205 Facial/Dental Trauma Aliases None noted Patient Care Goals 1. Preservation of dentition Patient Presentation Inclusion Criteria Isolated facial injury, including trauma to the eyes, nose, ears, midface, mandible, dentition Exclusion Criteria 1. Stable dentition (poorly anchored teeth require vigilance for possible aspiration) 3. Mental status assessment for possible traumatic brain injury [see Head Injury guideline] 6. Specific re-examination geared toward airway and ability to ventilate adequately Treatment and Interventions 1. Alternatively, an alert and cooperative patient can hold tooth in mouth using own saliva as storage medium 5. Expect patient cannot spit/swallow effectively and have suction readily available b. Preferentially transport sitting up with emesis basin/suction available (in the absence of a suspected spinal injury, see Spinal Care guideline) 7. Epistaxis - squeeze nose (or have patient do so) for 10-15 minutes continuously 8. Transport with tissue wrapped in dry sterile gauze in a plastic bag placed on ice c. Severe ear and nose lacerations can be addressed with a protective moist sterile dressing Patient Safety Considerations 1. Maintenance of a patent airway is the highest priority; therefore, conduct cervical spine assessment for field clearance (per Spinal Care guideline) to enable transport sitting up for difficulty with bleeding, swallowing, or handling secretions Notes/Educational Pearls Key Considerations 1. After nasal fractures, epistaxis may be posterior and may not respond to direct pressure over the nares with bleeding running down posterior pharynx, potentially compromising airway 3. Avulsed teeth may be successfully re-implanted if done so in a very short period after injury b. Revision Date September 8, 2017 208 Head Injury Aliases None noted Patient Care Goals 1. Administer oxygen as appropriate with a target of achieving 94-98% saturation 209 2. If patient unable to maintain airway, consider oral airway (nasal airway should not be used with significant facial injury or possible basilar skull fracture) c. Assume concomitant cervical spine injury in patients with moderate/severe head injury 3. Geriatric Consideration: Elderly patients with ankylosing spondylitis or severe kyphosis should be padded and immobilized in a position of comfort and may not tolerate a cervical collar Notes/Educational Pearls Key Considerations 1. If endotracheal intubation or invasive airways are used, continuous waveform capnography is required to document proper tube placement and assure proper ventilation rate 4. Prognostic factors in civilian gunshot wounds to the head: a series of 110 surgical patients and brief literature review. Influence of prehospital treatment on the outcome of patients with severe blunt traumatic brain injury: a single-centre study. The relationship between out-of-hospital airway management and outcome among trauma patients with Glasgow Coma Scale scores of 8 or less. Inappropriate prehospital ventilation in severe traumatic brain injury increases in-hospital mortality.
Syndromes
A 10 mg/mL dilution may be made by adding 1 mL of this solution to 9 mL of sterile water for injection. Atropine, aztreonam, calcium gluconate, clindamycin, dexamethasone, heparin (concentrations 1 unit/mL), hydrocortisone succinate, iron 580 Micormedex NeoFax Essentials 2014 dextran, isoproterenol, linezolid, metronidazole, norepinephrine, potassium chloride, procainamide, remifentanil, sodium bicarbonate, and vitamin K1. Zidovudine plus 3 doses of nevirapine is recommended for infants born to women who received only intrapartum antiretroviral therapy and for infants born to mothers who received no antepartum or intrapartum antiretroviral therapy [1]. Nevirapine is rapidly absorbed after oral administration to pregnant women and is highly lipophilic, resulting in therapeutic concentrations being readily transferred across the placenta to the fetus. Special Considerations/Preparation Available as an oral suspension in a concentration of 10 mg/mL. Birth weight greater than 2 kg: 12 mg/dose orally for 3 doses in the first week of life; give first dose within 48 hours of birth, second dose 48 hours after first dose, and third dose 96 hours after second dose [1]. There are no recommendations for use of nevirapine in premature neonates due to lack of safety and dosing data [1]. The zidovudine/nelfinavir/lamivudine regimen was associated with increased toxicity (eg, neutropenia) [3]. Special Considerations/Preparation 584 Micormedex NeoFax Essentials 2014 Available as an oral suspension in a concentration of 10 mg/mL. Product Information: Viramune(R) oral tablets, suspension, nevirapine oral tablets, suspension. Mirochnick M, Fenton T, Gagnier P et al: Pharmacokinetics of nevirapine in human immunodeficiency virus type 1-infected pregnant women and their neonates. Blood pressure equilibrium will not be achieved for approximately 50 hours (adult data). Administration Intravenous: Dilute prior to administration to a concentration of 0. Pharmacology Nicardipine is a dihydropyridine calcium channel blocker that significantly decreases systemic vascular resistance. Following infusion in adults, nicardipine plasma concentrations decline tri-exponentially, with a rapid early distribution phase (alpha half-life of 2. Experience in neonates is limited, and there are no reported pharmacokinetic data. Monitoring Continuous monitoring of blood pressure, heart rate and rhythm during initiation of therapy, and frequently thereafter. Store ampuls and premixed solution at controlled room temperature in carton until ready to use. Freezing does not adversely affect the product, but exposure to elevated temperatures should be avoided. Amikacin, aminophylline, aztreonam, calcium gluconate, cefazolin, ceftizoxime, chloramphenicol, cimetidine, clindamycin, dobutamine, dopamine, enalaprilat, epinephrine, erythromycin lactobionate, esmolol, famotidine, fentanyl, gentamicin, heparin (concentrations of 1 unit/mL or less), hydrocortisone, lidocaine, linezolid, lorazepam, magnesium sulfate, metronidazole, midazolam, milrinone, morphine, nafcillin, nitroglycerin, norepinephrine, penicillin G potassium, piperacillin, potassium chloride, potassium phosphate, ranitidine, sodium acetate, sodium nitroprusside, tobramycin, trimethoprim/sulfamethoxazole, vancomycin, and vecuronium. Michael J: Nicardipine for hypertensive emergencies in children with renal disease. Blood pressure will begin to decrease within minutes of starting the infusion, reaching half of its ultimate decrease in approximately 45 minutes. Administration 587 Micormedex NeoFax Essentials 2014 Intravenous: Dilute prior to administration to a concentration of 0. Contraindications/Precautions Contraindicated in patients with advanced aortic stenosis [1]. Adverse Effects No adverse effects have been reported in neonates (small numbers). Terminal Injection Site Incompatibility Ampicillin, cefepime, cefoperazone, ceftazidime, furosemide, heparin (concentrations greater than 1 unit/mL), micafungin, sodium bicarbonate and thiopental. Infants who cannot be weaned off after 4 days should undergo further diagnostic testing for other diseases. Contraindications/Precautions Contraindicated in infants dependent on right-to-left cardiac blood flow. Pulmonary edema has been reported in patients with preexisting left ventricular dysfunction. Abrupt discontinuation may result in worsening oxygenation and increased pulmonary artery pressures. Small increases in methemoglobin cause significant decreases in available oxygen content.
Examination of the nasal airway should include evaluation for symmetry of the nares, nasal septum deviation (Figure 2-1),12 and nasal turbinate hypertrophy. A bedside assessment of nasal airflow can be accomplished by February 2013 36 Mandibular retrognathia is suggested if the anterior prominence of the chin is 2 mm or more behind the virtual line. The Mallampati classification14 was developed to identify patients in whom tracheal intubation would be difficult; the initial description divided patients into three classes. Figure 2-3 16 illustrates the modified Mallampati classification assessed with the tongue protruded. The Friedman palate position classification,17 also commonly referenced, utilizes the same four categories but is done with the tongue at rest and not extended. Either the Mallampati or Friedman classification may be used to describe the patency of the oral airway. The class is determined by looking at the anatomy of the oral cavity and describes tongue size relative to oropharyngeal size. The test is conducted with the patient seated, the head held in a neutral position, and the mouth wide open and relaxed. The subsequent classification is assigned based upon the pharyngeal structures that are visible. This structural abnormality can predispose a patient to have sleep-disordered breathing. Two features to note in evaluation of the anterior dentition are overjet and overbite (Figure 2-6). Overjet is defined as increased projection of the upper teeth in front of the lower teeth as measured parallel to the occlusal plane. Overbite is the vertical overlapping of maxillary teeth over mandibular teeth, usually measured perpendicular to the occlusal plane. Displacement of the mandibular teeth posteriorly in relationship to the maxillary teeth results in more posteriorly crowded upper airways, predisposing patients for the development of obstructive sleep apnea. Of note, the mesiobuccal surface is the aspect of the tooth that is adjacent to the cheek mucosa. The mandibular and maxillary dental arches have a normal anterior-posterior relationship. The mesiobuccal groove of the mandibular first molar interdigitates with the mesiobuccal cusp of the maxillary first molar. The mandibular dental arch is in distal anterior-posterior relationship to the maxillary dental arch. The mesiobuccal groove of the mandibular first molar is distal to the mesiobuccal cusp of the maxillary first molar. The mandibular dental arch is in mesial anterior-posterior relationship to the maxillary dental arch. The mesiobuccal groove of the mandibular first molar is mesial to the mesiobuccal cusp of the maxillary first molar. To prevent overlooking these findings, a thorough head and neck assessment as described in Table 2-2 should be incorporated into the physical examination of all patients who present with sleep-related complaints. They can help to increase standardization in evaluations of patients by different clinicians or across centers. As shown in Appendix A, the Epworth Sleepiness Scale asks the responder to use a four-point Likert scale (0, 1, 2, or 3) to indicate the likelihood of dozing in eight distinct sedentary conditions. A total score of 10 or greater, out of a possible 24, suggests excessive daytime sleepiness. Many other questionnaires may be utilized in a clinical sleep evaluation; some pertain to overall sleep quality, while others are disorder-specific. Review of this information allows the clinician to estimate the total amount of sleep the patient obtains in a 24-hour period. Vertical lines represent when the patient went to bed, ``M' refers to when medication was taken, black shading represents time asleep, and unshaded white areas are time spent awake. Use of sleep diaries can be particularly helpful in patients with suspected circadian rhythm sleep disorders (including shift work), behaviorally induced insufficient sleep, or inadequate sleep hygiene. Other recorded parameters include thoracic and abdominal effort, oxygen saturation, nasal/oral airflow, and body position. Even electrode numbers (2, 4, 6, 8) represent the right hemisphere, and odd electrode numbers (1, 3, 5, 7) represent the left hemisphere.
Quality of life in bed partners of patients with obstructive sleep apnea or hypopnea after treatment with continuous positive airway pressure. A systematic review of treatments for settling problems and night waking in young children. Health care services utilization in children with obstructive sleep apnea syndrome. Daytime consequences and correlates of insomnia in the United States: Results of the 1991 National Sleep Foundation survey. Reducing motorvehicle collisions, costs, and fatalities by treating obstructive sleep apnea syndrome. Racial differences in clinical presentation of patients with sleep-disordered breathing. Technical report: Diagnosis and management of childhood obstructive sleep apnea syndrome. Sleep habits, excessive daytime sleepiness and school performance in high school students. Impaired sleep increases the risk of falls in older women: A prospective atigraphy study. Associations of frequent sleep insufficiency with health-related quality of life and health behaviors. Fatigue as a risk factor for being injured in an occupational accident: Results from the Maastricht Cohort Study. Thomas M, Sing H, Belenky G, Holcomb H, Mayberg H, Dannals R, Wagner H, Thorne D, Popp K, Rowland L, Welsh A, Balwinski S, Redmond D. Neural basis of alertness and cognitive performance impairments during sleepiness. Excessive daytime sleepiness at work and subjective work performance in the general population and among heavy snorers and patients with obstructive sleep apnea. Nocturnal arterial oxygen saturation and academic performance in a community sample of children. The cumulative cost of additional wakefulness: Dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation. Increasing the awareness and improving the diagnosis and treatment of sleep disorders necessitates a multipronged effort that includes three key components: public education, training for health professionals, and surveillance and monitoring. First, a public health campaign is required to increase awareness among the general population. Second, specific education and training strategies are needed to increase awareness among health care professionals, including improved curriculum content and certification requirements. There are a number of surveillance and monitoring tools, but very few examine issues pertaining to sleep loss and sleep disorders. Thus, third, improved surveillance and monitoring of the general population is needed. The preeminent goal of this strategy is to create and sustain a broad societal commitment to engaging in proper sleep habits as a primary tenet of health. In fact, being able to "get by on 4 hours of sleep" (and thus being able to increase productivity) is often considered an enviable trait. Daily sleeping and waking patterns are no longer driven by the light and dark cycle but, rather, by work schedules, economic interests, and increasing globalization. Unfortunately, the resulting "24/7" schedules are typically not optimal in terms of filling physiological requirements for sleep. Thus, daytime sleepiness and its consequences are becoming increasingly common problems affecting up to 15 percent of the population (Punjabi et al.
The prevalence, cost implications, and management of sleep disorders: An overview. The relationship between insomnia and health-related quality of life in patients with chronic illness. Sleep-disordered breathing and neuropsychological deficits: A population-based study. Accidents in obstructive sleep apnea patients treated with nasal continuous positive airway pressure: A prospective study. Utilization of health care services in patients with severe obstructive sleep apnea. The cost of sleep-related accidents: A report for the National Commission on Sleep Disorders Research. Successful behavioral treatment for reported sleep problems in elderly caregivers of dementia patients: A controlled study. Excessive sleepiness in adolescents and young adults: Causes, consequences, and treatment strategies. Empirically supported treatments in pediatric psychology: Bedtime refusal and night wakings in young children. A family intervention to delay nursing home placement of patients with Alzheimer disease: A randomized controlled trial. The Twenty-Four-Hour Society: Understanding Human Limits in a World That Never Stops. Daily social and physical activity increases slow-wave sleep and daytime neuropsychological performance in the elderly. Safety Study: Fatigue, Alcohol, Other Drugs, and Medical Factors in Fatal-to-the-Driver Heavy Truck Crashes (Volume I). Grounding of the Liberian Passenger Ship Star Princess on Poundstone Rock, Lynn Canal, Alaska June 23, 1995: Marine Accident Report. Sleep and neurobehavioral characteristics of 5- to 7-year-old children with parentally reported symptoms of attention-deficit/ hyperactivity disorder. Comparison of the severity of sleep-disordered breathing in Asian and Caucasian patients seen at a sleep disorders center. For some, sleep disruption and constant sleepiness are often deemed an inevitable part of their social roles as spouses, workers, caregivers, and so on. Although improving diet and exercise as a part of a healthy lifestyle program is acceptable, sleep continues to be considered an expendable luxury (Dzaja et al. Thus, performance and social responsibilities may often take precedence over sleep, largely because of multiple role demands and expectations. Acceptable standards for roles and activities are socially determined, and individuals who deviate from these expectations because of chronic illness are often labeled as "different" and are thus stigmatized (Falvo, 2005). Similarly, individuals with certain sleep disorders, which are often chronic in nature, may also be stigmatized because of the inability to fulfill role expectations. An additional factor that may underlie this stigma is that sleep is typically misperceived as an "asocial" activity. However, sleep is actually a very important type of social interaction-an activity that is negotiated with self, family, friends, employers, lawmakers, fellow drivers on the road, and so on (Meadows, 2005). The lack of awareness among the general public that results from the absence of sleep content in public health education programs causes patients to be hesitant about discussing sleep problems with their health care providers. In addition, fear of being labeled as having a psychiatric problem or exhibiting drug-seeking behaviors are also deterrents (Culpepper, 2002). In the case of insomnia, the most common of all sleep-related complaints, patients typically do not seek help because they believe either that nothing can be done or that the health care providers will do nothing to address the problem (Engstrom et al. Patients with excessive daytime sleepiness represent the largest group seeking help at sleep laboratories but often only after they have encountered numerous problems that interfere with performance of normal activities of daily living, their ability to hold a job and maintain a marriage, interact socially, or have had an accident. For children with narcolepsy, for example, the stigma associated with their increased daytime sleep tendency can affect social acceptance owing to unusual behavior as well as future risk of increased psychiatric disorders, potential obesity, and depressive symptoms (Dahl et al. Thus, individuals may have to overcome a stigma attached to having a sleep disorder, and seeking appropriate treatment is a very serious issue.
References:




