These lesions, which were quite pronounced upon inspection, formed concentric rings in a serpiginous fashion. There was central clearing without a leading or trailing scale, and areas of secondary hyperpigmentation. Examination of his fingernails revealed pitting, as well as subungual thickening and discoloration. Pathologic examination (via punch biopsy taken from the edge of a plaque on the left thigh) demonstrated an epidermal acanthosis with elongated, club-shaped epidermal ridges, as well as thinning of the suprapapillary plates and a diminished granular layer. Additionally, there was prominent, confluent parakeratosis with collections of neutrophils. Based on the clinical presentation described above, as well as the findings appreciated on frozen section, a diagnosis of psoriasis was made. Empirical therapy with topical triamcinolone was initiated and resulted in modest improvement. Discussion the figurate erythemas are a unique group of dermatoses that represent the cutaneous manifestation of various underlying diseases. Although appearing similar in its clinical presentation, the pathogenesis of erythema gyratum repens is oftentimes much more serious in nature and thus requires significant consideration when evaluating a patient with this disease. Radiographic, laboratory, and histologic modalities are all part of this comprehensive evaluation, as internal malignancy has been found in approximately 80% of the cases identified. Our case of er ythema gyratum repens-like psoriasis represents a unique presentation of an extremely common disease. This disease has been reported previously during resolution of pustular psoriasis, following treatment with acitretin, and now following trauma. Although a direct correlation cannot be proven, the onset of this rash, along with the koebnerization, makes this a likely association. Additionally, this case exemplifies the mathematical modeling of pattern formation that appears due, at least in part, to the perturbation of the predisposed genetic regulatory network, as well as to external factors and other entities not yet fully understood. Erythema annulare centrifugum-type psoriasis: a particular variant of acute-eruptive psoriasis. Modeling skin disease: Lessons from the worlds of mathematics, physics, and computer science. Of the various types of morphea, the linear form is the most common subtype among pediatric patients. Case Report A 13-year-old black female presented to our clinic with a two-year history of non-healing, scarring and bruising on the right side of her face. Her past medical history was unremarkable, and there were no prior related medical problems. The patient denied any other symptoms such as headaches, jaw and tooth pain, eating difficulties, joint pain, seizures or learning disabilities. Physical examination revealed a moderately well-demarcated, tan-yellow, bound-down, linear plaque with brown hyperpigmented borders encompassing the entire right forehead and involving the right upper eyelid and the right side of the nose (Figure 1). On the right cheek extending to the right jaw line and the chin, there was a moderately well-demarcated, tan-yellow, bound down, atrophic plaque with brown hyperpigmented and violaceous borders (Figure 2). Based on the history and physical exam, the diagnosis of facial morphea, en coup de sabre, was established. In an attempt to attenuate any further disfigurement, our patient was started on a regimen of oral prednisone 60 mg daily, oral methotrexate 15 mg weekly, and folic acid 1 mg daily. Discussion Morphea is an inflammatory disease primarily of the dermis and subcutaneous fat, which ultimately leads to a scar-like sclerosis. Classic features of morphea include asymmetric, linear, sclerotic plaques, usually 2-15 cm in diameter. Active lesions can have a lilac border, and inactive lesions often become hyperpigmented.
Dosimetriccomparisonbetweenprotonbeamtherapyandphoton radiation therapy for locally advanced esophageal squamous cell carcinoma. Proton beam therapy with high-dose irradiation for superficial and advanced esophagealcarcinomas. Comparison of adverse effects of proton and X-ray chemoradiotherapyforesophagealcancerusinganadaptivedosevolumehistogramanalysis. Clinical outcomes of intensity-modulated proton therapy and concurrent chemotherapy in esophageal carcinoma: a single institutional experience. Thepotentialofprotontherapytoreduceacutehaematological toxicity in concurrent chemoradiotherapy for oesophageal cancer. Proton beam therapy for hepatocellular carcinoma: a retrospectivereviewof162patients. ChangeinPlateletCountandNormalLiverDosimetryinPatients Receiving Proton Radiation Therapy for Unresectable Hepatocellular Carcinoma or Intrahepatic Cholangiocarcinoma. Follow-up study of liver metastasis from breast cancer treatedbyprotonbeamtherapy. HepatocyteGrowthFactorisAssociatedWithLiverDysfunction and Survival: Biomarker Results of a Phase 2 Study of Proton Beam Therapy in Patients with HepatocellularCarcinomaandIntrahepaticCholangiocarcinoma. Complete response of unresectable icteric-type hepatocellular carcinomatohypofractionatedprotonbeamtherapywithconcurrentplusadjuvantsorafenib:acase report. Dose-volume histogram analysis for risk factors of radiation-induced rib fracture after hypofractionated proton beam therapy for hepatocellular carcinoma. Optimal time of tumour response evaluation and effectiveness of hypofractionated proton beam therapy for inoperable or recurrent hepatocellular carcinoma. Hepatocellular carcinoma radiation therapy: review of evidence and future opportunities. Clinical results and risk factors of proton and carbon ion therapyforhepatocellularcarcinoma. A phase I study on combined therapy with proton-beam radiotherapyandinsitutumorvaccinationforlocallyadvancedrecurrenthepatocellularcarcinoma. Evaluation of the risk for radiation-induced liver disease following photon- or proton-beam radiosurgery of liver metastases. Monitoring of hepatocellular carcinoma, following proton radiotherapy, with contrast-enhanced color Doppler ultrasonography. Normal liver tissue sparing by intensity-modulated proton stereotacticbodyradiotherapyforsolitarylivertumours. Riskofsecondmalignantneoplasmfollowingprotonversus intensity-modulated photon radiotherapies for hepatocellular carcinoma. Feasibility of pancreatectomy following high-dose proton therapyforunresectablepancreaticcancer. Comparison of proton beam radiotherapy and hyperfractionated accelerated chemoradiotherapy for locally advanced pancreatic cancer. Proton therapy with concomitant capecitabine for pancreaticandampullarycancersisassociatedwithalowincidenceofgastrointestinaltoxicity. Protons offer reduced normal-tissue exposure for patients receivingpostoperativeradiotherapyforresectedpancreaticheadcancer. Spot-scanned pancreatic stereotactic body proton therapy: a dosimetricfeasibilityandrobustnessstudy. Protons offer reduced bone marrow, small bowel, and urinary bladder exposure for patients receiving neoadjuvant radiotherapy for resectable rectal cancer. Irradiationwithprotonsfortheindividualizedtreatmentof patients with locally advanced rectal cancer: A planning study with clinical implications. Which technique for radiation is most beneficial for patientswithlocallyadvancedcervicalcancer Toward amodel-based patient selection strategy for proton therapy:Externalvalidationofphoton-derivednormaltissuecomplicationprobabilitymodelsinahead andneckprotontherapycohort. Proton therapy for carcinoma of the nasopharynx: a study in comparativetreatmentplanning. Impactofearlyradiologicalresponseevaluationonradiotherapeutic outcomes in the patients with nasal cavity and paranasal sinus malignancies. Proton therapy reduces treatment-related toxicities for patients with nasopharyngeal cancer: a case-match control study of intensity-modulated proton therapyandintensity-modulatedphotontherapy.
Syndromes
Contents of the nucleus pulposus in the neural canal may cause an inflammatory reaction and irritate the dural sac, its nerve root sleeves, or the nerve roots. The symptoms may persist for extended periods and are not responsive to purely mechanical changes. Poor resolution of this inflammatory stimulus may lead to fibrotic reactions, nerve mobility impairments, and chronic pain. Onset is usually between 20 and 55 years of age but most frequently from the mid-thirties to forties. Except in cases of trauma, symptomatic onset in the lumbar spine is Disk Pathologies and Related Conditions Disk herniation, tissue fluid stasis, diskogenic pain, and swelling from inflammation are conditions that may result from prolonged flexion postures, repetitive flexion microtrauma, or traumatic flexion injuries. Initially, symptoms may be exacerbated when attempting extension but then may be decreased when using carefully controlled extension motions. Several studies have documented that patients with a herniated nucleus pulposus who have symptom reduction with an extension approach to treatment respond favorably to conservative nonsurgical treatment. Pain may occur without nerve root involvement, although there may be referred pain in the extremities. Tissue Fluid Stasis With sustained flexed postures in the spine, the disks, facet joints, and ligaments are placed under sustained loading. The intradiskal pressure increases, and there is compression loading on the cartilage of the facets and a distractive tension on the posterior longitudinal ligament and posterior fibers of the annulus fibrosus. Sudden movement into extension does not allow for redistribution of the fluids and so increases the vulnerability of the distended tissue to injury and inflammation. Signs and Symptoms of Disk Lesions and Fluid Stasis Etiology of Symptoms the disk is largely aneural; therefore not all disk protrusions are symptomatic. C H A P T E R 1 5 the Spine 413 usually associated simply with bending, bending and lifting, or attempting to stand up after having been in a prolonged recumbent, sitting, or forward-bent posture. The patient often describes increased pain when attempting to get out of bed in the morning or when first standing up. Symptoms are usually aggravated with activities that increase the intradiskal pressure, such as sitting, forward bending, coughing, or straining or when attempting to stand after being in a flexed position. Usually, symptoms are lessened when walking except when the bulge is large or the nuclear material has prolapsed and moved beyond the confines of the annulus. When there is a lumbar disk lesion, initially discomfort is noticed in the lumbosacral or buttock region. In the cervical spine, initially pain is noticed in the midscapular and shoulder area. Numbness or muscle weakness (neurological signs) are not noted unless the protrusion has progressed to a degree to which there is nerve root, spinal cord, or cauda equina compression. Objective Clinical Findings in the Lumbar Spine N O T E: the following information relates to a contained posterior or posterolateral nuclear protrusion in the lumbar spine. The patient may have a decrease in or loss of lumbar lordosis and may have some lateral shifting of the spinal column. Backward bending is limited; when repeating the backward-bending test, the pain lessens or centralizes. Centralization means that the symptoms recede up the leg or become localized to the back. If the protrusion cannot be mechanically reduced, backward bending peripheralizes or increases the symptoms. If there is a lateral shift of the spinal column, backward bending increases the pain. If the lateral shift is first corrected, repeated backward bending lessens or centralizes the pain. Testing passive lumbar flexion in the supine position (double knees-to-chest) and passive extension in the prone position (press-ups) usually produces signs similar to those of the standing tests, but results may not be as dramatic because gravity is eliminated. Pain between 30 and 60 of straight-leg raising is considered positive for interference of dural mobility but not pathognomonic for a disk protrusion. A complete tear of the outer layers of the annulus disrupts the hydrostatic mechanism, so the herniated or prolapsed nuclear material cannot be influenced by movement.
The left fifth intercostal space close to the sternum is the tricuspid or right ventricular area. Inspect and palpate the aortic and pulmonic areas, observing them at an angle and to the side, to note the presence or absence of pulsations. Auscultate the heart in all four anatomic sites: aortic, pulmonic, tricuspid, and apical (mitral). Auscultation need not be limited to these areas; however, the nurse may need to move the stethoscope to find the most audible sounds for each client. Rationale: this ensures adequate blood flow through the other artery to the brain. Rationale: Pressure can occlude the artery, and carotid sinus massage can precipitate bradycardia. The carotid sinus is a small dilation at the beginning of the internal carotid artery just above the bifurcation of the common carotid artery, in the upper third of the neck. If you hear a bruit, gently palpate the artery to determine the presence of a thrill. Although either the internal or the external jugular vein can be used, the internal jugular vein is more reliable. Rationale: the external jugular vein is more easily affected by obstruction or kinking at the base of the neck. If splitting of S2 is heard during normal respirations, it is abnormal and may indicate an atrial-septal defect, pulmonary stenosis, or another heart problem. Certain aspects of peripheral vascular assessment are often incorporated Peripheral Vascular System into other parts of the assessment procedure. For example, blood pressure is usually measured at the beginning of the physical examination (see the section on assessing blood pressure in Chapter 29). However, many aspects of the vascular system are observed during usual care and may be recorded by individuals other than the nurse. Perform hand hygiene and observe other appropriate infection prevention procedures. If you have difficulty palpating some of the peripheral pulses, use a Doppler ultrasound probe. Inquire if the client has any of the following: past history of heart disorders, varicosities, arterial disease, and hypertension; lifestyle habits such as exercise patterns, activity patterns and tolerance, smoking, and use of alcohol. Inspect the peripheral veins in the arms and legs for the presence and/or appearance of superficial veins when limbs are dependent and when limbs are elevated. Rationale: Palpation augments inspection findings, particularly in darker pigmented people in whom redness may not be visible. Inspect the skin of the hands and feet for color, Skin color pink temperature, edema, and skin changes. Document findings in the client record using printed or electronic forms or checklists supplemented by narrative notes when appropriate. If coarctation is present, femoral pulses will be diminished and radial pulses will be stronger. The lower extremities are more likely to show signs of arterial and venous impairment because of the more distal and dependent position. Peripheral arteries become thicker and dilate less effectively because of arteriosclerotic changes in the vessel walls. Often, however, the most distal pulses of the lower extremities are more difficult to palpate because of decreased arterial perfusion. Any client with a blood pressure reading above 140/90 mmHg should be referred for follow-up assessments. Educate clients and families regarding skin and nail care, exercise, and positioning to promote circulation. Men have some glandular tissue beneath each nipple, a potential site for malignancy, whereas mature women have glandular tissue throughout the breast. In females, the largest portion of glandular breast tissue is located in the upper outer quadrant of each breast.
Feeding difficulties in premature infants are usually secondary to (choose one): a. In contrast to term infants, the following statements are true regarding physiologic jaundice in the premature infant in the neonatal period (choose one): a. The following statements regarding the persistence of ductus arteriosus are true in the premature infant (choose one): a. Obstructive secondary to collapse of the upper airway structures and closure of the glottis. True/False: the weight of the premature infant is an absolute criterion for discharge from the hospital. The sudden onset of significant respiratory distress and hypotension should suggest what respiratory disorder Respiratory distress syndrome of the premature infant is caused by what deficiency What disorder would you consider in a cyanotic infant without respiratory distress What are the 2 most common congenital heart diseases leading to cyanosis in the newborn period What therapies are used as a bridge to definitive therapy in cyanotic congenital heart disease True/False: the definitive treatment for pulmonary hypertension of the newborn is surgical A 2 day old term infant previously thought to be well and about to be discharged from the nursery becomes acutely pale, slightly cyanotic, with weak femoral and brachial pulses. True/False: Because cardiac murmurs are uncommon in the newborn period, echocardiography should be performed on all newborns when a murmur is detected. True/False: Cyanosis of the hands and feet of a newborn may be normal if the mucus membranes are pink. True/False: the level of hypoglycemia resulting in serious sequelae is well defined by scientific studies. The advantage of using formula over 5% dextrose water (oral) to feed a moderately hypoglycemic term infant is: a. One ounce of standard formula is equivalent gm per gm to a 2 ml/kg intravenous bolus of 5% dextrose. What is the formula to calculate the glucose infusion rate and at what level should you start Which of the following infants are at risk for hypoglycemia and should have a screening blood sugar performed in the term nursery Intrapartum medications included 3 doses of butorphanol (narcotic opioid analgesic). She is centrally pink with persistent grunting, shallow respirations, and lethargy. The chest x-ray is rotated with fluid in the right fissure, diffuse streakiness on the left, and a normal cardiac silhouette. Is the volume of blood obtained for the blood culture important to the culture being positive or negative Is there good evidence that treatment of maternal chorioamnionitis prior to delivery significantly reduces the risk of neonatal infection Does prophylaxis for group B strep infection alter the time course of early onset group B streptococcal sepsis if prophylaxis is ineffective What is the incidence of neonatal sepsis and what is the mortality from neonatal sepsis Name some physical findings that can suggest that an infant has a congenital infection How does a congenital infection differ from an infection that is acquired perinatally
What is the most likely age an infant with a large ventricular septal defect will begin manifesting symptoms of congestive heart failure Administration of supplemental oxygen to a child with a large left to right shunt lesion will help improve the degree of congestive heart failure. What is the dominant mechanism with which infants and young children increase their cardiac output True/False: All neurohormonal and sympathetic responses of the body to heart failure are beneficial. True/False: Equal blood pressures in the right arm and left leg rule out the diagnosis of coarctation of the aorta. True/False: the presence of palpable femoral pulses rules out the diagnosis of aortic coarctation. A 2 year old infant is noted to have mild cyanosis who assumes a squatting position during long walking. He is noted to have increasing fussiness followed by increasing cyanosis, limpness and unresponsiveness. An infant with a marked cyanotic congenital heart defect with decreased pulmonary vascularity should be treated with: a. A "tet spell" or "blue" spell of tetralogy of Fallot is treated with all of the following except: a. A 7 year old girl presents with a tender and swollen right knee as well as a more recently appearing swollen left wrist. Does the pediatric case presented at the beginning of this chapter meet the Duke Criteria for Diagnosis of infective endocarditis What type of prophylactic antibiotic against infective endocarditis would you prescribe to a nine-year old female, with a past medical history only remarkable for an allergic reaction to penicillin, scheduled for a tooth extraction the next day What is the most common microorganism that causes pediatric infectious myocarditis in the United States Which of the following answer is the most severe clinical manifestation commonly found in pediatric myocarditis Which of the following is/are treatments options for pediatric postpericardiotomy syndrome True/False: Supraventricular tachycardia is the most common cause of syncope in the pediatric age group. All of the following studies could find evidence to support the diagnosis of a suspected vascular ring except: a. Describe clinical findings signifying the severity of an acute asthma exacerbation. Discuss the approach to an asthmatic in relationship to formulating an acute asthma treatment plan. What questions do you ask, what physical findings do you look for, and what laboratory parameters are measured Describe various triggering factors and mechanisms by which they might exert their action. Describe the immunologic chain of events that ultimately leads to bronchospasm and inflammation. Discuss the pros and cons of corticosteroid use in children and compare them with use in adults. How would you convince parents of asthmatics to use medications when their children are not openly symptomatic Organisms characteristically isolated from the sputum of patients with cystic fibrosis includes all the following except: a. All of the following factors are included in the pathogenesis of chronic lung disease except: a. For adequate growth, infants with chronic lung disease frequently require a caloric intake of: a. True/False: Causes of bronchiectasis in childhood include cystic fibrosis, asthma and immunodeficiency.
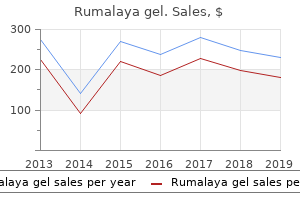
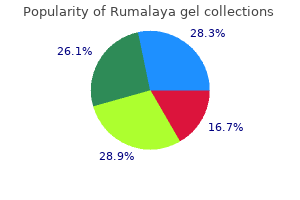
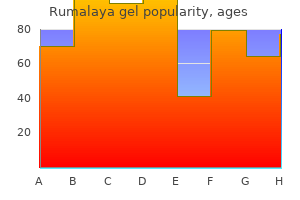
Horseradish. Rumalaya gel.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96281

Two examples of segmental breathing that target the lateral and posterior segments of the lower lobes are described in this section. However, segmental breathing techniques also may need to be directed to the middle and upper lobes if there is accumulation of secretions or insufficient lung expansion in these areas. Lateral Costal Expansion Lateral costal expansion, sometimes called lateral basal expansion, can be carried out unilaterally or bilaterally. As the patient breathes out, place pressure into the ribs with the palms of your hands. Just prior to inspiration, apply a quick downward and inward stretch to the chest. Apply light manual resistance to the lower ribs to increase sensory awareness as the patient breathes in deeply and the chest expands and ribs flare. Then, as the patient breathes out, assist by gently squeezing the rib cage in a downward and inward direction. Teach the patient how to perform the maneuver independently by placing his or her hand(s) over the ribs. Pursed-Lip Breathing Pursed-lip breathing is a strategy that involves lightly pursing the lips together during controlled exhalation. Many therapists believe that gentle pursed-lip breathing and controlled expiration is a useful procedure, particularly to relieve dyspnea if it is performed appropriately. Studies suggest that pursed-lip breathing decreases the respiratory rate and the work of breathing (oxygen consumption), increases the tidal volume, and improves exercise tolerance. Forceful expiration while the lips are pursed can increase the turbulence in the airways and cause further restriction of the small bronchioles. Therefore, if a therapist elects to teach this breathing strategy, it is important to emphasize with the patient that expiration should be performed in a controlled manner but not forced. Procedure Have the patient assume a comfortable position and relax as much as possible. Have the patient breathe in slowly and deeply through the nose and then breathe out gently through lightly pursed lips as if blowing on and bending the flame of a candle but not blowing it out. Posterior Basal Expansion Deep breathing emphasizing posterior basal expansion is important for the postsurgical patient who is confined to bed in a semireclining position for an extended period of time because secretions often accumulate in the posterior segments of the lower lobes. Procedure Have the patient sit and lean forward on a pillow, slightly bending the hips. C H A P T E R 2 5 Management of Pulmonary Conditions 865 the patient that expiration must be relaxed and that contraction of the abdominals must be avoided. It is helpful to teach a patient how to monitor his or her level of shortness of breath and to prevent episodes of dyspnea by controlled breathing techniques, pacing activities, and becoming aware of what activity or situation precipitates a shortness of breath attack. If the patient becomes slightly short of breath, he or she must learn to stop an activity and use controlled, pursed-lip breathing until the dyspnea subsides. A forwardbent position stimulates diaphragmatic breathing (the viscera drop forward and the diaphragm descends more easily). Have the patient gain control of his or her breathing and reduce the respiratory rate by using pursed-lip breathing during expiration. Have the patient focus on the expiratory phase of breathing while being sure to avoid forceful expiration. After each pursed-lip expiration, teach the patient to use diaphragmatic breathing and minimize use of accessory muscles during each inspiration. Have the patient remain in a forward-bent posture and continue to breathe in a slow, controlled manner until the episode of dyspnea subsides. Positive Expiratory Pressure Breathing Positive expiratory pressure breathing is a technique in which resistance to airflow is applied during exhalation, similar to what occurs during pursed-lip breathing, except that the patient breathes through a specially designed mouthpiece or mask that controls resistance to airflow. Positive expiratory pressure breathing provides an alternative or adjunct to postural drainage which a patient can perform independently. Procedure Positive expiratory pressure breathing is performed in an upright position, preferably seated with the elbows resting on a table. A low pressure technique involves tidal inspiration and active, but not forced, expiration through a mouthpiece or mask. The patient inhales, holds the inspiration for 2 to 3 seconds, and then exhales, repeating the sequence for approximately 10 to 15 cycles.

Recognize optic nerve features of disorders that cause visual field loss (eg, optic nerve head drusen, optic neuritis). Describe slit-lamp findings of secondary glaucomas (eg, iridocorneal endothelial syndrome, pigment dispersion syndrome, exfoliation syndrome, angle recession). Interpret visual field results for Goldmann kinetic perimetry and Humphrey or Octopus standard automated perimetry. Recognize ocular emergencies of acute angle closure, and blebitis/endophthalmitis. Know epidemiology of congenital glaucoma, primary open-angle glaucoma, exfoliation syndrome and exfoliative glaucoma, and angle-closure glaucoma. Recognize secondary glaucomas (eg, angle recession, inflammatory, steroid induced, pigmentary, exfoliative, phacolytic, neovascular, postoperative, malignant, lens-particle glaucomas, plateau iris, glaucomatocyclitic crisis, iridocorneal endothelial syndrome) with attention to appropriate pathophysiology. Describe the evaluation and treatment of complex secondary glaucomas (eg, exfoliation, angle recession, inflammatory, steroid induced, pigmentary, phacolytic, neovascular, postoperative, malignant, lens-particle glaucomas; plateau iris; glaucomatocyclitic crisis; iridocorneal endothelial syndromes; aqueous misdirection/ciliary block). Recognize and describe more advanced optic nerve and nerve fiber layer anatomy in glaucoma and typical and atypical features associated with glaucomatous cupping (eg, rim pallor, disc hemorrhage, parapapillary atrophy, rim thinning, notching, circumlinear vessels, central acuity loss, hemianopic or other nonglaucomatous types of visual field loss). Describe and interpret more advanced forms of perimetry (kinetic and automated static), including various perimetry strategies such as threshold testing, suprathreshold testing, and special algorithms. Describe the principles involved in determining glaucomatous progression both clinically and perimetrically. Describe the principles, and more advanced anatomic gonioscopic features of primary and secondary glaucomas (eg, plateau iris, appositional closure). Describe the principles of medical management of more advanced glaucomas (eg, advanced primary open-angle glaucoma, secondary open and closed angle glaucomas, normal tension glaucoma). Describe pitfalls of medical treatment, in particular poor compliance and adherence. Describe and recognize the features of angle-closure glaucomas and aqueous misdirection. Describe the principles, indications, and techniques of various types of laser energy, spot size, and laser wavelengths. Describe the principles, indications, and techniques of trabeculectomy (with or without cataract surgery, with or without antimetabolites), glaucoma drainage devices, and cyclodestructive procedures. Describe the major etiologies of dislocated or subluxated lens associated with glaucoma (eg, trauma, Marfan syndrome, homocystinuria, Weill-Marchesani syndrome, syphilis). Describe the less common causes of lens abnormalities associated with glaucoma (eg, spherophakia, lenticonus, ectopia lentis). Describe diagnostic accuracy, false positive and false negative diagnoses and their significance at individual and societal levels, differences between case-based and community-based screening, including an understanding of sensitivity and specificity, number needed to treat, t tests, life-table analysis, prospective versus retrospective studies, case control and cohort studies. Select appropriate drugs and be able to customize or modify medical treatment for openangle, secondary, and angle-closure glaucomas. Assist with trabeculectomy and glaucoma drainage device surgery in the operating room. Describe the etiology, pathophysiology, and clinical characteristics of the most complex glaucomas (eg, angle recession, multimechanism glaucoma, traumatic glaucoma, neovascular, uveitic glaucoma, iridocorneal endothelial syndrome). Identify the key examination techniques and management of complex medical and surgical problems in glaucoma (eg, complicated or postoperative primary and secondary open-angle and closed-angle glaucoma, uncommon visual field defects). Apply the most advanced knowledge of optic nerve and nerve fiber layer anatomy and describe and interpret techniques, methods, and tools for analyzing the nerve fiber layer. Recognize and evaluate atypical or multifactorial glaucomatous cupping (eg, rim pallor) and when to order additional tests to rule out other pathologies (eg, magnetic resonance imaging, computerized tomography scan, carotid Doppler). Know how to diagnose progression using special software available with optic nerve and retinal measurement technologies and know the errors and limitations of the instruments. Describe, interpret, and apply the results of the most complex and advanced forms of perimetry, including special kinetic and automated static perimetry strategies (eg, special algorithms) in atypical or multifactorial glaucoma. Describe visual field damage, progression, rate of progression, caveats, and their use in glaucoma management. Describe medical management of the most advanced and complex glaucoma (eg, advanced primary open-angle glaucoma previously treated with medicine, laser, or surgery; secondary glaucomas). Describe, recognize, and know how to treat the most advanced cases of primary openangle glaucoma (eg, monocular patients, repeat surgical cases), normal tension glaucoma, and secondary glaucomas (eg, inflammatory glaucoma, angle recession).
Forward motions emphasize spinal flexion and shoulder girdle protraction; backward motions emphasize spinal extension and shoulder girdle retraction. Coach the patient to assume the neutral spinal posture and use the stabilizing muscles prior to and during the use of the ergometer to enhance postural responses. If the machine can be used standing, progression to the standing position stimulates a total body response. Step Aerobics and Aerobic Dancing Stepping is similar to using stairs or a stair machine except for the jumping and bouncing that is usually added to the more advanced step aerobic programs. Dancing moves take on many forms, and classes are taught that address various fitness levels and age groups. If possible, review safe movement patterns and help the patient recognize the safe limits of his or her spinal range and abilities. Stair Climbing Commercial devices that replicate stepping with various grades of resistance are used for strengthening and aerobic conditioning. This activity requires pelvic control of the reciprocating lower extremities because lifting the leg on one side emphasizes spinal flexion while the contralateral lower extremity and spine are extending. Coach the patient to maintain the neutral spine with the stabilizing muscles against the rotational forces. Knowledge and skill in analyzing the biomechanics of the activity and the forces that are imposed through the spine should be used to provide advice about exercise safety. End-of-range postures and high-velocity stresses (such as vigorous kicking and ballistic motions) may be damaging to vulnerable tissues in the spine and should not be attempted by patients recovering from spinal problems. Cross-Country Skiing and Ski Machines Cross-country skiing, whether out in the cold or on a commercial machine, is a high-intensity aerobic activity. The kicking motion that accompanies the backward motion of the leg emphasizes spinal extension. It is important to coach the patient to maintain the neutral spine and contract the stabilizing abdominal muscles. Swimming When swimming, the breaststroke emphasizes extension in the cervical and lumbar spinal regions when taking a breath. Coach the patient to not extend the neck full range but to keep it neutral and lift the head out of the water as a "solid" unit with the thorax just enough to clear the mouth for the breath. The freestyle stroke may exacerbate cervical problems because of the repetitive cervical rotation while taking a breath; this stroke also emphasizes lumbar extension with the flutter kick. N O T E: Achieving the maximum level of independence underlies all the goals of therapeutic exercise. Approach the open car door and seat with the back toward the seat; stabilize the spine in its neutral position with the drawing-in maneuver, then bend at the hips and sit down. Once seated, flex both hips and knees and pivot the whole body around as a unit, maintaining a stable spine. When exiting a car, keep both knees together and pivot the legs and trunk outward as a unit. Once the feet are on the ground, bend at the hips and elevate the trunk as a unit. Remind the patient to use the neutral spine and drawingin maneuvers to stabilize the spine while walking. It is not possible to maintain conscious control for long, so remind the patient to check the spinal posture and reactivate the drawing-in maneuver whenever the symptoms recur. These techniques follow the early kinesthetic training instruction in which the patient learns to find his or her neutral spine and experiences the effect that simple arm and leg motions have on the spine, as well as early muscle performance training in which the patient learns how to activate the core musculature for segmental stabilization. Rolling with a neutral spine requires that the patient first find the neutral spine, perform the drawing-in maneuver, and then roll the trunk as a unit. It may be helpful to suggest that the patient "imagine a solid rod connecting the shoulders and pelvis so as not to twist" or suggest that he or she "roll like a log. Have the patient use the log roll maneuver (as described above) to roll from supine to side-lying while simultaneously flexing the hips and knees and pushing up with the arms. Help the patient focus on stabilizing the trunk with commands such as "push up your trunk as if it is a board; do not allow it to twist or bend. Once down, the patient can roll to supine or prone-lying using the log-roll technique Sit to stand/stand to sit.
He is somewhat fussy and demanding of feedings, and his mother complains of getting no rest as she has to feed him hourly. Recently, her left breast has become quite sore and there is intense pain when he nipples. On examination, the infant is colicky, but there is no abdominal tenderness and his vital signs are also within normal limits with no adjunct signs of intravascular volume depletion. A 14 year old female has yet to show secondary sexual development which you have always attributed to excessive involvement with the school track team. A 3 year old boy presents to the emergency department passing bright red blood per anus. He is diaphoretic and tachycardic (120 supine, 140 upright) and complains of generalized abdominal pain. You are unable to localize tenderness but are comfortable that there is no rebound tenderness and he is not at risk of perforation. By the time you have given enough crystalloid to replete his blood volume, his hemoglobin has dropped to 7 grams. Since his summer physical 2 months ago had included a hemoglobin of 12, you realize he has indeed lost a substantial portion of his blood volume over a short period of time. He is admitted to the hospital, where over the next two days as you wait for the stool culture results. He requires 250 cc transfusions daily to maintain his hemoglobin and you realize that the brisk bleeding continues. Dietary fats, proteins, and carbohydrates are hydrolyzed and stabilized by digestive enzymes and bile in which phase True/False: the symptoms of malabsorption are worse in older children compared to younger children. True/False: Diarrhea is the most common presenting symptom of malabsorption in younger children. True/False: Withdrawal of gluten-containing food from a patient with celiac disease is often enough to reverse the symptoms of malabsorption. What is the purpose of using epinephrine in local infiltration and topical anesthesia What has the best cosmetic result in the repair of lacerations: sutures or tissue adhesives What is the major clinical reason for preferring healing by secondary or tertiary intention (as opposed to primary closure) True/False: Antibiotics have only a modest effect on reducing the rate of wound infections in contaminated wounds. Each testis descends through the inguinal canal into the scrotum within the processus vaginalis. A scrotal hydrocele, or simple hydrocele, is a type of non-communicating hydrocele. True/False: the risk of incarceration and strangulation of an inguinal hernia is highest in the first 12 months of life. Which of the following is not part of the differential diagnosis of an inguinal-scrotal swelling in children Which of the following is not a risk factor for development of an inguinal hernia In cases of right lower quadrant pain and tenderness what is the second most frequent system implicated as its cause Contraindications for non-surgical reduction of an intussusception include all of the following except: a. A pathologic lead point can be identified in approximately what percentage of patients with intussusception All three of the "classical triad" of symptoms is found in what percentage of patients with intussusception Does the term "malrotation" refer to any patient condition, symptom or malformation description that is relevant for clinicians
References:




