Therefore, we suggest that such plots be used only as indicators of potential problems. The final judgment on model adequacy should be based on appropriate statistical tests. A more general procedure for determining whether the straight-line model adequately fits the data tests the null hypothesis H0: E(y) = 0 + 1 x against the alternative Ha: E(y) = 0 + 1 x. You can see that this test, called a test for lack of fit, does not restrict the alternative hypothesis to second-order models. Recall that a manufacturer of a new tire tested the tire for wear at different pressures with the results shown in the table. The elastic properties of the material were investigated in the Journal of Applied Physics (September 1993). A diamond anvil cell was used to compress a mixture of moissanite, sodium chloride, and gold in a ratio of 33:99:1 by volume. Recall that the researchers want to predict failure time (y) based on solder temperature (x). Fit the straight-line model, E(y) = 0 + 1 x, to the data and plot the residuals against solder temperature. In theory, then, the demand for the gem would increase as the price increases, decreasing at low prices, leveling off at moderate prices, and increasing at high prices, because obtaining the gem at a high price confers high status on the owner. Although a quadratic model would seem to match the theory, the model proposed to explain the demand for the gem by its price is the first-order model y = 0 + 1 x + where y is the demand (in thousands) and x is the retail price per carat (dollars). Refer to the National Semiconductor study on using tinlead solder bumps to manufacture silicon wafer integrated circuit chips, Exercise 4. Recall that the data on 35 boilers were used to fit the model E(y) = 0 + 1 x1 + 2 x2 + 3 x3 + 4 x4 where y = Man-hours x1 = Boiler capacity (lb/hr) x2 = Design pressure (psi) x3 = x4 = 1 0 1 0 if industry erected if not if steam drum if mud drum Source: Gee, S. Unequal variances for different settings of the independent variable(s) are said to be heteroscedastic. However, plots of the residuals will frequently reveal the presence of heteroscedasticity. In this section we show how residual plots can be used to detect departures Detecting Unequal Variances 399 from the assumption of equal variances, and then give a simple test for heteroscedasticity. In addition, we suggest some modifications to the model that may remedy the situation. When data fail to be homoscedastic, the reason is often that the variance of the response y is a function of its mean E(y). If the response y is a count that has a Poisson distribution, the variance will be equal to the mean E(y). For example, the number of sick days per month for an employee would very likely be a Poisson random variable. If the variance of a response is proportional to E(y), the regression residuals produce a pattern about y, the ^ least squares estimate of E(y), like that shown in Figure 8. Many responses are proportions (or percentages) generated by binomial experiments. For instance, the proportion of a random sample of 100 convicted felons who are repeat offenders is an example of a binomial response. Binomial proportions have variances that are functions of both the true proportion (the mean) ^ and the sample size. In fact, if the observed proportion yi = pi is generated by a binomial distribution with sample size ni and true probability pi, the variance of yi is pi (1 - pi) E(yi)[1 - E(yi)] = Var(yi) = ni ni Residuals for binomial data produce a pattern about y like that shown in ^ Figure 8. The random error component has been assumed to be additive in all the models we have constructed. An additive error is one for which the response is equal to the mean E(y) plus random error, y = E(y) + Another useful type of model, especially for business and economic data, is the multiplicative model. In this model, the response is written as the product of its mean and the random error component, that is, y = [E(y)] the variance of this response will grow proportionally to the square of the mean, that is, Var(y) = [E(y)]2 2 where 2 is the variance of. Data subject to multiplicative errors produce a pattern of residuals about y like that shown in Figure 8. For example, if the response y is a count that follows a Poisson distribution, the square root transform y can be shown to have approximately constant variance. Consequently, if the response is a Poisson random variable, we would let y = y and fit the model y = 0 + 1 x1 + · · · + k xk + this model will satisfy approximately the least squares assumption of homoscedasticity.
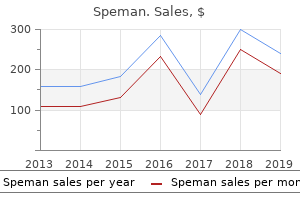
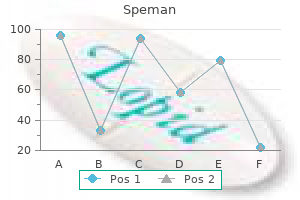
Life Expectancy at Birth, 20052010 To understand health statistics, it is important to define a few epidemiological terms. Incidence is defined as the number of new cases of an illness per population at risk in a given amount of time; for example, the number of new cases of lung cancer per 1000 at-risk people per year. Prevalence is a measure of the number of cases of an illness overall-whether new or chronic-per population in a given amount of time; for example, the number of people with new or chronic lung cancer per 1000 people per year. Morbidity is the burden or degree of illness associated with a given disease, while mortality refers to deaths caused by a given disease. This was first demonstrated in the nineteenth century through public health efforts. Health is dependent not only on geography, but also on social and economic factors. After a time, socioeconomic improvements lead to greater general health in the population, and the best health outcomes are generally seen in egalitarian societies. However, despite the ambitions of the modern welfare state, the Black Report of 1980 showed that class differences in health still exist, with professional groups having longer life expectancies than working-class people. Howard Waitzkin described this outcome as the second sickness, which is an exacerbation of health outcomes caused by social injustice. Poverty, in combination with a culture of inequality, leads to worse health outcomes, and this effect runs across gender, age, and racial and ethnic boundaries. For example, low-income women are more likely to deliver babies with low birth rates, thereby placing them at risk for numerous physical and cognitive problems in life. Members of the lower class, overall, are four times more likely to view themselves in worse health compared with affluent groups. Low-income groups are much more likely to develop life-shortening diseases such as lung cancer, diabetes, heart disease, and other degenerative illnesses. They are also more likely to commit suicide and die from homicide in comparison to wealthier adults. The infant mortality rate among the poor is also much higher; in some populations of the United States, the infant mortality rate can approximate that of developing countries. However, because of the correlation between poverty and racial and ethnic minorities, many of these characteristics apply to particular ethnic groups more than others. When it comes to health and illness among racial and ethnic minorities, Asian-Americans and Pacific Islanders have some of the best health profiles. Reports illustrate that, in comparison to white Americans, this group has a lower rate of death associated with cancer, heart disease, diabetes, and infant mortality. Specifically, African-American males have the lowest life expectancy of any racial or gender category. Hispanics also have a high mortality rate from influenza, pneumonia, and accidents. Native Americans also show some of the highest rates of death by suicide in comparison to the general population. This group also has some of the highest mortality rates linked to diabetes compared to any racial category. When it comes to gender-related health disparities, most statistical information shows that females have better health profiles than males. Female life expectancy has been consistently higher than male life expectancy since records began. While the gap in life expectancy is beginning to narrow in the United States, most countries still have higher life expectancies for female citizens than male citizens, as shown in Figure 12. Male and Female Life Expectancies by Region and Country Note that female life expectancies are almost universally higher than male life expectancies. Mortality rates from heart disease, cancer, chronic lower respiratory diseases, diabetes, and accidents are higher for males than females. Men are also three times more likely than women to die from accidents, suicide, and homicide. Men, especially those raised to have hypermasculine behaviors, may try to "tough it out" rather than go to a doctor.
Allying himself with the analytic intelligence of Aristotle, the author of the Sacred Wood battles against critics who "substitute emotion for thoughts. And like Bradley in his censure of Mill, Eliot focuses on a loose definition of poetry: the sentence ["poetry is the most highly organized form of intellectual activity"]. The inventor of poetry as the most highly organized form of intellectual activity was not engaged in perceiving when he composed this definition; he had nothing to be aware of except his own emotion about "poetry. But as a point of Aristotelian anthropology, all feeling is not in perception: feeling, by virtue of its interpersonal character, by its very depth, precedes the self. Hazlitt says of Shakespeare and Milton: "They owe their power over the human mind to their having had a deeper sense than others of what was grand in the objects of nature, or affecting in the events of human life. And this change is accompanied by an almost imperceptible revision of the Posterior Analytics. Aristotle had said: "All instruction given or received by way of argument proceeds from pre-existent knowledge" (71a1). In his theory of aesthetic judgment, Kant had opened the possibility, which he himself did not endorse, of a full-fledged departure T. Bernard Bosanquet offers a precedent for Eliot in his well-known work A History of Aesthetic: From the Greeks to the Twentieth Century, especially the section "Aristotle on Tragedy," which speaks eloquently of the religion of art. Writes James: "In the aesthetic emotions the bodily reverberation and the feeling may both be faint. A connoisseur is apt to judge a work of art dryly and intellectually, and with no bodily thrill. On the other hand, works of art may arouse intense emotion; and whenever they do so, the experience is completely covered by the terms of our theory. Despite the work of James, Eliot restores the barrier and protects the nineteenth-century religion of art. Instead of refining ordinary human emotion (and I do not mean tepid human emotion, but human however intense in the crude living state) he aims direct at emotions of art. Are lordships sold to maintain ladyships For the poor benefit of a bewildering minute? To recall James, one may conclude that Eliot falls, along with his impeccable taste, into the category of "a connoisseur. It will be remembered that Arnold was concerned with "primary affections" and "elementary feelings," not with "art emotions" that sharply divide the aesthetic from the ethical. The classical hero is a paragon for Arnold, because classical authors appeal to the "permanent elements" of our nature. In Homer, for instance, the Greek mind discerns a difference between heroic excellence (virtue in the earliest sense) and social justice. Eliot: the modernist Aristotle 53 chosen to enter the world of action, Achilles inhabits the mean between extreme self-consciousness and complete unselfconsciousness. Prufrock and Gerontion at one extreme, and Sweeney at the other, are like the damned, dwelling outside any living tradition of moral life. In "What the Thunder Said," the poet undergoes a trial of mystical heroism, a quest for perfection that can be achieved only through selfless dedication to God. The poet-priest, through his apocalyptic struggle, tries to revive a dead world; in his Notes to the Waste Land, Eliot documents some examples of this attempt in myth and religion. He sacrifices the ego by estranging the normal life of emotion from aesthetic feelings (art emotions). Eclipsing the ego, he creates a lyric halo or corona around the culture of the West. The myriad voices of the Waste Land admit of many readings, but the egocentric feeling of lyric control is never absent. It shows its social nature in the nervous system and the blood stream, when it affects the feelings of the author and the reader. Through the presence or absence of this link, the artist declares himself to be either a literary citizen or a literary exile. Either he locates himself in the giving and receiving of a community, or he enters into different exilic modes, be it the barbarism of Sweeney, or the skeptical self-consciousness of Prufrock, or the mystical questing of the Waste Land. Eliot prepared his Clark Lectures by studying neo-Thomism, which spoke to problems of social order that had "preoccupied him since his first acquaintance with the work of Babbitt and Maurras. And in this material I include the emotions and feelings of the writer himself, which, for that writer, are simply material which he must accept not virtues to be enlarged or vices to be diminished.
They may remember the vision they have had, but they cease to regret it, Maintain themselves by the common routine, Learn to avoid excessive expectation, Become tolerant of themselves and others, Giving and taking, in the usual actions What there is to give and take. They do not repine; Are contented with the morning that separates And with the evening that brings together For casual talk before the fire Two people who know they do not understand each other, Breeding children whom they do not understand And who will never understand them. But you will want nothing else, And the other life will be only like a book You have read once, and lost. With the reiteration of "understand," a conduplicatio that hollows out the word like a chime, Eliot teases us into sensing the limits of our usual round of thoughts and phrases. Eliot upholds the ethical integrity of persons in the community of "giving and taking" that is the source, in Aristotelian terms, of our shared life of feeling. People become "tolerant," the increase of tolerance being for Eliot a benefit of humanism in a religious society. In the speech, "casual" harbors an etymological play on a Latin word for "fall," and "breeding" recalls the opening lines of the Waste Land. His exilic mode enacts what he lamented as a 64 the Ethics of Modernism Cartesian distance between the self and its emotions. From start to finish, Eliot applies an art of interruption, of fragmented action, not only for certain comic effects, but to disrupt our emotional investment in the characters, so that we cannot escape our spiritual burden. I come back to Bradley in order to affirm the moral coherence of the Cocktail Party, such as it is. As in Ethical Studies, self-consciousness ultimately transcends the mutual consciousness of friendship, and directs the self on its lonely journey to God. As in Ethical Studies, the community has a moral basis, though a higher, religious morality exists for a select few. It is arduously difficult, with little reward for the effort, to fathom both these viewpoints within a single consciousness. More, we express our dual nature, which is sometimes in our deepest experience contradictory, in a host of ways. Likewise, we may observe the duality of human perspective in yet another Eliotic tension, between the private covenant of grace (a compact between God and the individual saint) and the public covenant of the people to build a city of God. The comedy of the Cocktail Party is metaphysical: it is the theoretical resolution of ethical and spiritual problems that, on the stage of life, challenge our sanity and our civilization. Socrates, he says, used skepticism and irony in a dialectic that pointed beyond Socrates: "What Socrates opposes to convention is his universal self. It is, however, reasonable to defend romantic irony as healthy skepticism toward moral authority. It lends itself to good government, and enriches what the nineteenth-century French historian Francois Guizot called the "diversity" ё of European culture. He is skeptical and impious and a myth-maker who, like Socrates, gives a saving form to fate. In 1903, he praised Ibsen for assisting "the breaking-up of tradition, which is the work of the modern era. In A Portrait of the Artist as a Young Man, we enter a world of teachers, who possess knowledge that is wide and varied, but cut off, like church Latin, from the fresh turnings of experience. As we read the book, the Jesuit hierarchy gives way to a new arrangement, where Stephen is to the Jesuits as the Jesuits are to the Christian Brothers. By mastering his experience through the English language, Stephen claims artistic and spiritual superiority. The stages of his growth, from early consciousness to refined self-consciousness and creative power, establish for author and reader alike an authentic mode of selfhood a convincing union of life and art. It was Pater who gave the idea of authenticity its most perfect expression: "The theory or idea or system which requires of us the sacrifice of any part of. Stephen tells Cranly, in their last conversation before the diary: "I will not serve that in which I no longer believe whether it call itself my home, my fatherland or my church. This dissolution did not happen in Stephen Hero, to judge from the manuscript that survives.
More recent treatments evaluated by double-blind comparisons include clonazepam (Thaker et al. Quite often, however, it will be found that no available therapy ameliorates the condition and one must merely hope for spontaneous resolution. The temptation to control the dyskinesia by reintroducing neuroleptics at increased dosage is strictly to be avoided, except in those rare cases where life is threatened by the severity of the involuntary movements. While it may be highly efficacious in producing short-term relief, this merely postpones the problem by reinstating the original pathogenesis and can be expected to worsen the ultimate disability. Tardive dystonia Tardive dystonia presents equally severe management problems and the results of treatment are often disappointing. The first step should be to taper or discontinue the causative drugs or change to alternative therapy. Anticholinergic drugs such as trihexyphenidyl (benzhexol) can help, though at the expense of worsening any coincident tardive dyskinesia. Reserpine or tetrabenazine were associated with improvement in two-thirds of patients (Kang et al. Clozapine holds special promise and has been reported to help after fruitless attempts with other drugs, leading to slow improvement over several months (Lamberti & Bellnier 1993). It would certainly appear to be the drug of choice in patients whose psychosis requires the continuation of neuroleptics (Friedman 1994; Van Harten et al. The combination of clozapine and clonazepam has sometimes proved to be particularly effective (Shapleske et al. If the dystonia is localised, for example in the cervical region, botulinum toxin might be used (Brashear et al. Tardive akathisia Treatment of tardive akathisia can be particularly difficult, not least because discontinuation of neuroleptics may lead to transient worsening. This should nevertheless be attempted, even though few cases will benefit substantially. Anticholinergics and beta-blockers were without effect, although lorazepam improved occasional patients markedly. Sometimes the reintroduction of neuroleptics at higher dosage may ultimately need to be tried. A large number of other associated features are also characteristic as described below. By far the commonest form is idiopathic parkinsonism or paralysis agitans, as described by James Parkinson in 1817. This owes its origin to a specific degeneration of pigmented cells in the brainstem, particularly those of the substantia nigra. Substantial changes in our understanding of the genetic aspects of the disease have occurred in the last decade. In most cases the genes and loci have been identified in very rare families showing a simple mendelian pattern of disease inheritance, but some of these findings are now being Table 12. Three autosomal dominantly inherited point mutations in this gene have been described, including the original Greek family, other southern Mediterranean families and a single German family. A family with triplication of a large region that included the -synuclein gene has also been reported. In contrast, many different mutations have been described in the parkin gene on chromosome 6. The identification of -synuclein in particular, but also that of parkin and some of the other genes, have disclosed an important pathogenic role for the ubiquitinproteosome system, a cytoplasmic complex that breaks down aggregates of misfolded, unassembled or damaged protein. Aggregates of -synuclein are a substrate for breakdown by the ubiquitinproteosome system. Mutant -synuclein protein is associated with excess aggregate formation, as are a variety of environmental factors including oxidative stress, heavy metals and pesticides. Although such aggregation may represent a protective mechanism, it appears that when aggregate formation exceeds the capacity of the proteosome system, it accumulates (as Levy bodies) and is associated with cell death (apoptosis). Novel therapeutic possibilities include neuroprotective strategies targeting proteins in the proteosome system, aiming to inhibit aggregate formation or enhance protein degradation. There has been considerable interest in the possibility of genetic testing but because the genes identified so far are relatively rare and in many cases of uncertain penetrance, there is no agreed protocol for genetic testing or counselling.
Using similar survey methods, the same investigators have reported higher rates of bipolar symptoms (as distinct from bipolar disorder) in people with epilepsy compared with various medical control groups (Ettinger et al. Although half of those with bipolar symptoms reported being given a past diagnosis of bipolar disorder, it is possible that these findings reflect atypical forms of depression that some authorities have said are common. It has been suggested that 30 70% of patients with epilepsy and depression have these atypical features. The syndrome is said to respond to antidepressant treatment perhaps in combination with low-dose neuroleptics (Blumer et al. Most clinicians will recall patients who seem to fit these descriptions but much work needs to be done to establish the validity of the concept. In particular, phenomenological comparisons with the spectrum of affective presentations in people without epilepsy are required to establish whether the syndrome is truly specific to epilepsy. The atypical nature of these presentations is cited as one reason why depression in epilepsy often goes unrecognised and untreated. Controlled trials demonstrating that such symptoms respond to treatment would help support the assertion that patients with atypical presentations represent a significant unmet need. Clinical presentation of depression in epilepsy the possibility that depression in epilepsy may take atypical forms has attracted considerable interest. Several investigators have been struck by the fact that depressive symptoms in people with epilepsy often fall short of standard diagnostic criteria and yet are associated with significant morbidity (Mendez et al. Essentially, the clinical picture is one of chronic dysthymia which is interrupted at frequent intervals by brief periods of normal mood. Affective symptoms are pleomorphic, with prominent irritability and endogenous somatic symptoms. Patients would meet standard diagnostic criteria for chronic dysthymia were it not for the intermittent course of the disorder (Kanner 2003). Blumer (1991) has described a more elaborate complex of symptoms including labile depressive symptoms (depressed Risk factors for depression A relationship between depression and poorly controlled epilepsy was most clearly demonstrated in the communitybased study by Jacoby et al. Information on 696 patients was collected from general practice records and by postal questionnaires. Around half of the patients had been free of seizures for over a year, 27% were experiencing one or less seizures per month and 20% had more frequent seizures. Among seizure-free patients, 4% were found to have significant depression scores on the Hospital Anxiety and Depression Scale. The figure rose to 10% in those experiencing less than one seizure per month and to 21% in those with more frequent seizures. Studies based in tertiary referral centres are naturally biased in favour of patients with poorly controlled epilepsy. In these settings, a relationship with seizure frequency is generally not found (Mendez et al. However, when such patients undergo temporal lobectomy, becoming seizure-free is associated with an improvement in depressive symptoms (Reuber et al. This view has found some support from direct comparisons between epilepsy syndromes. A larger study comparing 150 patients with localisation-related epilepsy and 70 with idiopathic generalised epilepsy found higher measures of depression 342 Chapter 6 and anxiety in the former group (Piazzini & Canger 2001). However, the mean seizure frequency in those with generalised epilepsy was less than one per year, while those with partial seizures averaged six per month. This was not controlled for in the analyses and may well have confounded the results. In contrast, a number of recent studies have found similar rates of depression across epilepsy syndromes (Manchanda et al. Underlining the fact that patients with generalised epilepsy are at risk of depression, Cutting et al. Overall, outcome was favourable, with seizures completely controlled in two-thirds and 90% in full employment.
One study has looked at the value of a specialist liaison nurse on the neurosurgical unit (Pritchard et al. The nurse was a senior neurosurgical ward nurse whose role was to support and counsel patients with subarachnoid haemorrhage and their families. Once the liaison nurse was in place, the progress of a cohort of patients admitted over a 2-year period was compared with a cohort of patients admitted over the previous 18 months. At 6 months after discharge the patients who had access to the specialist liaison nurse showed better emotional adjustment and confidence, and greater satisfaction with their inpatient treatment. In the early days after subarachnoid haemorrhage, once the diagnosis has been established, there are three main considerations: (i) minimise the risk of rebleeding, (ii) try to prevent delayed cerebral ischaemia, and (iii) manage any hydrocephalus. Rebleeding is the major cause of poor outcome; without intervention more than one-third of patients will rebleed within the first few weeks. This risk can be reduced by surgical intervention, but in the past this necessarily involved a craniotomy and surgical clipping of the aneurysm and the threat of aggravating cerebral ischaemia. Over the last few years clipping has largely been replaced by coiling of the aneurysm using an intra-arterial catheter. Once the end of the catheter is in place in the aneurysm, small platinum coils are detached to rest in the aneurysm which then becomes occluded by reactive thrombosis. There is a chance of the aneurysm subsequently reopening and some clinicians regard long-term follow-up angiography as mandatory (Feigin & Findlay 2006). The advantage of coiling, in terms of survival, was maintained at 7-year follow-up (Molyneux et al. However, some aneurysms will be unsuitable for coiling because of their anatomical configuration. Cerebral ischaemia, sometimes involving vessels at a distance from the aneurysm, is a considerable problem for many patients over the hours and days after subarachnoid haemorrhage, reaching a peak after 12 weeks. Infarcts, usually involving the cortex, may be found in almost 40% of patients (Rabinstein et al. In some they are single infarcts often near the aneurysm but in others multiple infarcts at a distance from the site of rupture are seen. Patients with a large amount of subarachnoid blood or with loss of consciousness are at increased risk. Vasospasm may be partly to blame, but global ischaemia and hypotension are contributory factors. Treatment with calcium antagonists, in particular nimodipine for 3 weeks, reduces the risk of poor outcome (Rinkel et al. Shunting should be restricted to those with good clinical evidence of need and be for as short as possible, because of the risk of ventriculitis. Nevertheless, the clinician needs to remember that hydrocephalus may be a cause of deterioration in mental state, months or years after haemorrhage. In the long term perhaps 23% of patients will rebleed over the 10 years after surgical clipping for subarachnoid haemorrhage (Wermer et al. With modern management some two-thirds of patients may be expected to survive a first bleed, although one-third of survivors will be left with major neurological disability. In patients with no aneurysm demonstrable on angiography the mortality and morbidity rates are considerably lower. High levels of pituitary deficiency have been found after subarachnoid haemorrhage and it has been suggested that this may contribute to chronic symptoms in a proportion of cases (KreitschmannAndermahr et al. Psychiatric sequelae of subarachnoid haemorrhage Severe, but usually transient, confusion and states of akinetic mutism can be seen in the early stages of recovery. The later sequelae, after 211 years, were described by Walton (1952, 1956) among 120 survivors. Important residua included persistent headache in 23%, organic mental symptoms in 9% and anxiety symptoms in 27%. The anxiety was occasionally severely disabling, resulting in chronic psychiatric invalidism.
More recently, standardised diagnostic assessments have ascertained the frequency of Axis 1 mental disorders after closed head injury. High rates of depression and anxiety disorders were identified in patients with a head injury attending a brain injury rehabilitation outpatient clinic; 26% had a major depressive disorder and 24% generalised anxiety disorder (Fann et al. Comorbidity is common; in one study half of patients with major depression also had generalised anxiety disorder (van Reekum et al. It was not possible to say if these disorders antedated or postdated the head injury. What is perhaps surprising from these studies is the relative lack of reporting of post-traumatic stress disorder. Cognitive impairment More severe head injuries are likely to be followed by persisting cognitive impairment of a degree proportional to the amount of brain damage incurred. In these cases concussion and amnesia may then be brief or absent, yet focal cognitive defects can be severe, especially if haemorrhage or infection have occurred. Damage to the dominant hemisphere will generally produce more severe effects on intellectual function than damage to the non-dominant hemisphere (Teuber 1959, 1962; Piercy 1964). As in almost all cases of diffuse brain damage, the hallmarks of the cognitive impairment of closed head injury are psychomotor slowing, difficulties with attention and concentration and memory, and impairment of executive function. In cases where the only finding was diffuse axonal injury the most frequent impairments were in memory and executive function, but no cognitive domain was consistently spared (Scheid et al. Impairments of speed of information processing, capacity for information processing, attention and executive function go hand in hand and many of the common cognitive symptoms of closed head injury can be understood as arising from their selective vulnerability. The result is slowness over tasks, inattention due to overload, and distractibility due to lack of spare capacity for the monitoring of irrelevant stimuli; working memory is impaired (McDowell et al. These symptoms overlap with those described as part of the dysexecutive syndrome: lack of fluency and problems with dual-task processing and multi-tasking, organising, planning and prioritising, switching from one task to another, inhibiting behaviour and adapting to novel situations, abstract reasoning and judgment, and with monitoring. Dissecting out the contribution of the psychological processes underlying these various symptoms is not easy. For example, the attentional problems that follow brain injury are multifaceted and overlapping. They include alterations in alertness, psychomotor slowing, distractibility, impaired sustained attention and difficulties switching attention (van Zomeren et al. The degree to which these various facets of attention share common processing impairments is uncertain. It seems likely that while slowed speed of information processing is central to many attentional problems (Ponsford & Kinsella 1992), it cannot account for all (Whyte et al. So, for example, impairments of those aspects of attention related to executive function (Spikman et al. Simple reaction times are not a good indicator of injury severity and more complex tasks are more likely to show evidence of psychomotor slowing. It has been suggested that delayed processing speed is particularly likely when interhemispheric information procession is required (Mathias et al. Head Injury 203 Likewise dual-task processing impairments may be particularly vulnerable to diffuse brain injury (Vilkki et al. No one single measure of executive function seems adequate to capture the various impairments and behaviours that may be described as being part of the dysexecutive syndrome (Bamdad et al. Some patients with good evidence in day-to-day life of disorganised thinking due to brain injury will nevertheless perform well on standard frontal executive tests. Impairments may only be evident for tests which replicate the unstructured demands of everyday life (Shallice & Burgess 1991); tests of shopping performance seem to be particularly telling (Alderman et al. The growing literature on the cognitive processes, located particularly in medial orbitofrontal lobe, involved in decision-making in relation to goal-directed behaviour (Kringelbach & Rolls 2004) helps explain how impairments of cognition overlap with changes in behaviour and personality (Damasio 1996). For example, central executive deficits measured using dual-task processing may be related to . Patients are given the task of buying items in a certain order, with additional rules that they have to follow. Abnormal performance on a gambling test may be associated with personality change (Levine et al. Memory is also disproportionately affected in relation to intellectual function (Levin et al. Several problems are characteristic of the memory impairment of closed head injury (Baddeley et al. Inaccurate recall of memories is probably partly related to problems with source memory, in other words identifying the context in which a memory is embedded.
References:




