Reflecting on the earlier work of Cannon, Bard, and others, American neurologist James Papez proposed that there is an "emotion system," lying on the medial wall of the brain that links the cortex with the hypothalamus. Papez believed, as do many scientists today, that the cortex is critically involved in the experience of emotion. Papez believed that the experience of emotion was determined by activity in the cingulate cortex and, less directly, other cortical areas. The cingulate cortex projects to the hippocampus, and the hippocampus projects to the hypothalamus by way of the bundle of axons called the fornix. Hypothalamic effects reach the cortex via a relay in the anterior thalamic nuclei. Also, tumors located near the cingulate cortex are associated with certain emotional disturbances, including fear, irritability, and depression. Papez proposed that activity evoked in other neocortical areas by projections from the cingulate cortex adds "emotional coloring" to our experiences. In the Papez circuit, the hypothalamus governs the behavioral expression of emotion. The hypothalamus and neocortex are arranged so that each can influence the other, thus linking the expression and experience of emotion. In the circuit, the cingulate cortex affects the hypothalamus via the hippocampus and fornix (the large bundle of axons leaving the hippocampus), whereas the hypothalamus affects the cingulate cortex via the anterior thalamus. While anatomical studies demonstrated that the components of the Papez circuit were interconnected as Papez had indicated, there was only suggestive evidence that each was involved in emotion. One reason Papez thought the hippocampus is involved in emotion is that it is affected by the virus responsible for rabies. An indication of rabies infection, and an aid in its diagnosis, is the presence of abnormal cytoplasmic bodies in neurons, especially in the hippocampus. Because rabies is characterized by hyperemotional responses such as exaggerated fear and aggressiveness, Papez reasoned that the hippocampus must be involved in normal emotional experience. Although little evidence related to the role of the anterior thalamus, other clinical reports at the time stated that lesions in this area led to apparent emotional disturbances, such as spontaneous laughing and crying. On September 13, 1848, while tamping explosive powder into a hole to prepare for blasting at a railroad construction site in Vermont, Phineas made the mistake of looking away from what he was doing. Incredibly, after being carried to an ox cart, Gage sat upright on the ride to a nearby hotel and walked up a long flight of stairs to go inside. When Harlow first saw Gage at the hotel, he commented that "the picture presented was, to one unaccustomed to military surgery, truly terrific" (p. As you might imagine, the projectile destroyed a considerable portion of the skull and left frontal lobe, and Gage lost a great deal of blood. Over the following Figure A Phineas Gage and the rod that passed through his brain. According to MacLean, the evolution of a limbic system enabled animals to experience and express emotions and freed them from the stereotypical behavior dictated by their brain stem. Difficulties with the Concept of a Single System for Emotions We have defined a group of interconnected anatomical structures roughly encircling the brain stem as a limbic system. On the other hand, some of the components of the Papez circuit are no longer thought to be important for the expression of emotion, such as the hippocampus. The critical point seems to be conceptual, concerning the definition of an emotion system. After Gage recovered from his wounds, he was apparently normal except for one thing: His personality was drastically and permanently changed. According to Harlow, before the accident Gage was considered "the most efficient and capable foreman. He possessed a well-balanced mind, and was looked upon by those who knew him as a shrewd, smart business man, very persistent in executing all his plans of operation" (pp. After the accident, Harlow described him as follows: the equilibrium or balance, so to speak, between his intellectual faculties and animal propensities, seems to have been destroyed. He is fitful, irreverent, indulging at times in the grossest profanity (which was not previously his custom), manifesting but little deference for his fellows, impatient of restraint or advice when it conflicts with his desires, at times pertinaciously obstinate, yet capricious and vacillating, devising many plans of future operation, which are no sooner arranged than they are abandoned in turn for others appearing more feasible. His mind was radically changed, so decidedly that his friends and acquaintances said he was "no longer Gage.
This, in turn, stretches, bends, or flattens the nearby nerve endings, which then increase or decrease their action potential firing frequency. The mechanoreceptors of hair follicles may be either slowly adapting or rapidly adapting. The different mechanical sensitivities of mechanoreceptors mediate different sensations. Place your hand against a speaker while playing your favorite music loudly; you "feel" the music largely with your Pacinian corpuscles. The selectivity of a mechanoreceptive axon depends primarily on the structure of its special ending. When the capsule is compressed, energy is transferred to the nerve terminal, its membrane is deformed, and mechanosensitive channels open. Current flowing through the channels generates a receptor potential, which is depolarizing (Figure 12. The skin was indented with a pressure probe, at various frequencies, while recording from the nerve. The amplitude of the stimulus was increased until it generated action potentials; threshold was measured as the amount of skin indentation in micrometers (m). A single Pacinian corpuscle was isolated and stimulated by a probe that indented it briefly. When indented by the probe, a receptor potential was again generated, showing the capsule is not necessary for mechanoreception. But while the normal corpuscle responded only to the onset or offset of a long indentation, the stripped version gave a much more prolonged response; its adaptation rate was slowed. Apparently it is the capsule that makes the corpuscle insensitive to low-frequency stimuli. If the stimulus pressure is maintained, the layers slip past one another and transfer the stimulus energy in such a way that the axon terminal is no longer deformed, and the receptor potential dissipates. When pressure is released, the events reverse themselves; the terminal depolarizes again and may fire another action potential. In the 1960s, Werner Loewenstein and his colleagues, working at Columbia University, stripped away the capsule from single corpuscles and found that the naked nerve terminal became much less sensitive to vibrating stimuli and much more sensitive to steady pressure (Figure 12. Clearly, it is the layered capsule (and not some property of the nerve ending itself) that makes the Pacinian corpuscle exquisitely sensitive to vibrating, high-frequency stimuli and almost unresponsive to steady pressure (see Figure 12. The mechanoreceptors of the skin all have unmyelinated axon terminals, and the membranes of these axons have mechanosensitive ion channels that convert mechanical force into a change of ionic current. Forces applied to these channels alter their gating and either enhance or decrease channel opening. Force can be applied to a channel by the membrane itself when it is stretched or bent, or force may be applied through connections between the channels and extracellular proteins or intracellular cytoskeletal components. Alternatively, mechanical stimuli may somehow trigger the release of second messengers. A variety of ion channel types have been implicated in mechanosensation, but the specific types of channels in most of the somatic sensory receptors are still unidentified. The epithelium-like Merkel cells make synapses onto nerve terminals, and it seems that both the Merkel cell and the axon terminal are mechanically sensitive. The Merkel cell has a mechanosensitive channel called Piezo2 that opens in response to pressure and depolarizes the cell. Depolarization triggers synaptic release of an unknown transmitter from the cell, which in turn excites the nearby nerve ending. Surprisingly, the nerve ending is also mechanically sensitive because of a second (unknown) ion channel in its own membranes. Our ability to discriminate the detailed features of a stimulus varies tremendously across the body. Start with the ends about an inch apart, and touch them to the tip of a finger; you should have no problem telling that there are two separate points touching your finger. Then bend the wire to bring the points closer together, and touch them to your fingertip again.
Conditioning involves pairing parallel fiber stimulation with climbing fiber stimulation. On the other hand, when the postsynaptic neuron is strongly depolarized, the Mg2 block is displaced entirely, and Ca2 floods into the postsynaptic neuron. These different types of Ca2 response selectively activate different types of enzymes. Instead of the kinases that are activated by high [Ca2]i, modest and prolonged elevations in [Ca2]i activate protein phosphatases, enzymes that pluck phosphate groups off proteins. However, despite this remarkable turnover, synaptic transmission will remain stable as long as one receptor is added whenever one receptor is removed. The capacity of the postsynaptic membrane is determined by the size of a scaffold of what has been termed slot proteins. Imagine the scaffold is like an egg carton, and the slot proteins form each of the egg cups. But because the size of the carton is increased, there continues to be a net increase in the number of eggs. Slices of human temporal cortex, removed during the course of surgery to gain access to deeper structures, were maintained in vitro. It appears that plasticity at many synapses in the cerebral cortex may be governed by similar rules and might use similar mechanisms. One approach has been to insert stimulating and recording electrodes in the hippocampus and use these to monitor the state of synaptic transmission during learning. Because of the distributed nature of memory, success with this approach required the use of a particularly robust type of learning called inhibitory avoidance. In this experiment, a rat learns to associate a place (the dark side of a box) with an aversive experience (a foot shock) (Figure 25. Animals of all types (from flies to humans) will learn to avoid the place they received the shock after only one trial (depending, of course, on the strength of the shock). This type of learning is not subtle, and neither are the patterns of hippocampal activation it produces. To test for the creation of a memory trace, one can measure the time it takes for the rat to re-enter the dark side at various time points after the initial experience. Unlike normal animals, these rats failed to learn the rules of the game or the location of the escape platform. Tonegawa, who switched to neuroscience after winning the 1987 Nobel Prize for his research in immunology, recognized that molecules and behavior could be connected by manipulating the genes of experimental animals. This approach had already been tried with success in simple organisms like fruit flies (Box 25. Moreover, since the protein is missing in all cells that normally express it, pinpointing where and how a molecule contributes to learning can be difficult. For these reasons, researchers have attempted to devise ways to restrict their genetic manipulations to specific times and specific locations. It is even possible that some proteins are uniquely involved in learning and memory. Needless to say, we could gain considerable insight about the molecular basis of learning and learning disorders if such hypothetical "memory molecules" could be identified. One way to identify a "memory protein" is to delete genes one at a time and see if specific learning deficits result. This is precisely the strategy that Seymour Benzer, Yadin Dudai, and their colleagues at the California Institute of Technology tried using the fruit fly Drosophila melanogaster. Drosophila has long been a favorite species of geneticists, but one might reasonably question to what extent a fruit fly learns. Fortunately, Drosophila can perform the same tricks that other invertebrate species like Aplysia have mastered. They demonstrate this memory after training by flying away when the odor is presented.
If there is leak from a component, take steps to ensure the liquid does not come into contact with skin or eyes. Proceed with caution if you are prone to internal bleeding; for example, after an injury or a fracture. If such material has entered into the units, it must be immediately checked by a service technician, before it can be reused. Never connect the stimulation cables to an external power supply, as there is a risk of electrocution. S a F e t y i N F O r M at i O N - Do not apply stimulation near the area of an implant, such as cochlear implants, pacemakers, skeletal anchorage or electric implants. Equipment malfunction - this warnings can cause equipment mailfunctions that result in patient hazards - Magnetic and electrical fields are capable of interfering with the proper performance of the unit. If you are in any doubt as to the use of the stimulator in close proximity to another medical device, seek advice from the manufacturer of the latter or from your doctor. Persons are authorized after training by a specialist trained and commissioned by the manufacturer. Damaged and worn parts must be immediately replaced with original spare parts by authorized staff. Patient hazard - these cautions need to be observed to avoid the risk of electrical shock or other negative effects to the patient. Remove jewellery, piercings, belt buckles or any other metallic product or device in the area of stimulation. The first five minutes of stimulation must always be performed on a person who is sitting or lying down. In rare instances, people of a nervous disposition may experience a vasovagal reaction. This is of psychological origin and is connected with a fear of the muscle stimulation as well as surprise at seeing one of their muscles contract without having intentionally contracted it themselves. A vasovagal reaction causes heart to slow down and blood pressure to drop, which produces a feeling weakness and a tendency towards fainting. If this does occur, all that is required is to stop the stimulation and for the person to lie down with the legs raised until the feeling of weakness disappears (5 to 10 minutes) - Never allow muscular contraction during a stimulation session to result in movement. You should always stimulate isometrically; this means that the extremities of the limb in which a muscle is being stimulated must be firmly fixed, so as to prevent any movement that results from contraction. Generally, this redness is completely harmless and usually disappears after 10 to 20 minutes. Never start another stimulation session in the same area, however, if the redness is still visible. Equipment damage - Check that the voltage and frequency ratings of your local power line are those indicated on the type plate of the power supply. However, make sure that these sources do not contaminate the physiotherapy unit and keep them away from it. Other electrodes and motor point pens may have electrical properties that are unsuitable for or may damage the Rehab/Theta/Physio. Some people, with very sensitive skin, may experience redness under the electrodes after a session. Generally, this redness is totally harmless and usually disappears after 10 to 20 minutes. However, never start another stimulation session on the same area if the redness is still visible - Instructions for electrodes. S a F e t y i N F O r M at i O N Note - For best results, wash and clean the skin of any oil and dry it before attaching the electrodes. Note Biocompatibility Those parts of the Rehab/Theta/Physio unit that come into contact with the patient when used as intended, are designed to fulfil the biocompatibility requirements of the applicable standards. C - +/- buttons for 4 stimulation channels D - Sockets for 4 stimulation cables E - Battery charger socket F - Stimulation cables Channel 1 = blue Channel 2 = green Channel 3 = yellow Channel 4 = red G - Stimulation cable fitted with pin connector H - Rechargeable battery compartment I - Belt clip socket Note emergency stop function: By pressing the On/Off button during stimulation, the device pauses. Both the +/- buttons and the cables are colour-coded to simplify use and facilitate identification of the different channels.
There is frequently a painful, hyperalgesic, or allodynic response to focal areas of scar palpation. Treatment involves desensitization therapy, diagnostic nerve blocks, scar injections, anti-neuropathic pain medications, and referral to peripheral nerve surgeons for consideration of scar revision, nerve graft, or nerve release. It is important to realize that not all neuropathies are painful, as is the case with most of the inherited neuropathies. Some patients with neuropathy have chronic pain due to other conditions, and their pain should not be immediately attributed to the concomitant nonpainful neuropathy. Polyneuropathy usually is symmetric and starts in a distalto-proximal gradient in a "glove and stocking" distribution. Mononeuropathy multiplex affects multiple peripheral nerves arbitrarily and sometimes can be difficult to differentiate from polyneuropathy. Neuropathies may result from injury to the axons (axonal neuropathies), to myelin (demyelinating neuropathies), or mixed lesions. Thalamic pain (Dejerine-Roussy syndrome) is the prototype of central pain, but lesions in the brainstem and other sites also can produce central pain. Strokes are the most common cause, with pain reported to occur in 8% of poststroke patients. The most common level of injury associated with pain is cauda equina followed by the central cord injuries. Syringomyelia and syringobulbia can occur as delayed consequences of trauma or congenital malformations and produce neuropathic pain of segmental pattern. The clinical presentation of central pain varies widely depending on the etiology and patient. Whereas the most common descriptors are adjectives such as "burning," "lancinating," and "aching"; others describe their pain more like "throbbing," "pulling," or "icy. Symptoms of sympathetically mediated pain include burning or stabbing pain, allodynia and/or trophic disorders. Naltrexone hydrochloride, an opioid antagonist, has more recently has been used as a treatment for fibromyalgia. This drug has been found to reduce proinflammatory cytokines and neurotoxic superoxides in the central nervous system microglia cells. In recent studies, naltrexone has show great promise in treating fibromyalgia symptoms with minimal side effects. Another advantage of these treatments is that they can lead to sustained (eg, >1 year) improvements. As in other disorders, there are relatively few controlled trials to advocate their general use. Trigger-point injections, chiropractic manipulation, tai chi, yoga, acupuncture, and myofascial release therapy all have some evidence of efficacy and are among the more commonly used modalities. As a result, nociceptors are activated by release of norepinephrine by sympathetic postganglionic fibers. Release of certain mediators, such as prostaglandins, by sympathetic fibers can further sensitize the nociceptive afferents. If the injury results in myelin loss of the fibers, artificial synapses develop between the affected sensory afferents and sympathetic efferents, a process called ephaptic transmission. The dorsal root ganglion is thought to be another site for ephaptic transmission resulting from sprouting of sympathetic postganglionic fibers around sensory neurons. At the level of the dorsal horn of the spinal cord, the wide dynamic range neurons, which are second-order neurons, are activated and sensitized by the active injured C fibers. Sensitized wide dynamic range cells are thought to be activated by other stimuli, such as light touch, explaining the phenomenon of allodynia. At the level of the brain, there is altered sensorimotor processing and increased hyperexcitability. Central changes are reflected as alterations in somatic sensation (including pain), the motor system, and the peripheral autonomically regulated effector systems (vasculature, sweat glands, inflammatory cells). Blood tests, including erythrocyte sedimentation rate, blood cell count, and rheumatologic testing, may be necessary to help rule out infection or a rheumatologic condition. Several factors may account for stump pain and should be evaluated, including surgical trauma, ischemia, local infection, ill-fitting prostheses, or a painful neuroma formation. Treatment of painful neuromas ranges from simple injections to surgical interventions, with varying degrees of success.
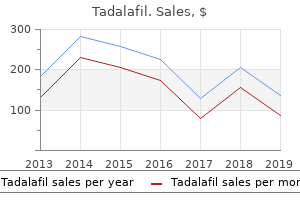
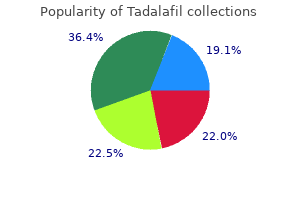
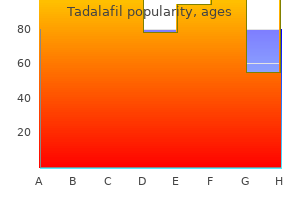
Indischer Wassernabel (Gotu Kola). Tadalafil.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96735
Thus, cortisol is a lipophilic ("fat-loving") molecule, which dissolves easily in lipid membranes and readily crosses the blood-brain barrier. Physicians need to be mindful of this feedback regulation when they prescribe prednisone, a synthetic form of cortisol. Cortisol can act directly on hypothalamic neurons, as well as on other neurons elsewhere in the brain. Abrupt discontinuation of prednisone treatment does not give the adrenal cortex enough time to ramp up cortisol production and can thus result in what is called adrenal insufficiency. Among the symptoms of adrenal insufficiency are severe abdominal pain and diarrhea, extremely low blood pressure, and changes in mood and personality. Addison recognized that one cause of this constellation of symptoms is degeneration of the adrenal gland. Kennedy required a daily regimen of hormone replacement therapy to compensate for the loss of cortisol, a fact that was concealed during his presidency to protect his youthful and vigorous image. The symptoms include rapid weight gain, immune suppression, sleeplessness, memory impairment, and irritability. The physiological responses associated with stress help protect the body and the brain from the dangers that triggered the stress in the first place. Neuroscientists have only begun to understand the relationship between stress, the brain, and brain damage. Stress leads to the release of the steroid hormone cortisol from the adrenal cortex. Cortisol travels to the brain through the bloodstream and binds to receptors in the cytoplasm of many neurons. The activated receptors travel to the cell nucleus, where they stimulate gene transcription and ultimately protein synthesis. Whatever the mechanism, presumably in the short term cortisol makes the brain better able to cope with the stress-perhaps by helping it figure out a way to avoid it! Bruce McEwen and his colleagues at Rockefeller University, and Robert Sapolsky and his colleagues at Stanford University, have studied this question in the rat brain. They found that daily injections of corticosterone (rat cortisol) for several weeks caused dendrites to wither in many neurons with corticosterone receptors. A similar result was found when, instead of daily hormone injections, the rats were stressed every day. Baboons in the wild maintain a complex social hierarchy, and subordinate males steer clear of dominant males when they can. During one year when the baboon population boomed, local villagers caged many of the animals to prevent them from destroying their crops. Unable to escape the "top baboons" in the cages, many of the subordinate males subsequently died-not from wounds or malnutrition but apparently from severe and sustained stress-induced effects. They had gastric ulcers, colitis, enlarged adrenal glands, and extensive degeneration of neurons in their hippocampus. Subsequent studies suggest that it is the direct effect of cortisol that damages the hippocampus. Indeed, research has clearly shown that chronic stress causes premature aging of the brain. In humans, exposure to the horrors of combat, sexual abuse, and other types of extreme violence can lead to posttraumatic stress disorder, with symptoms of heightened anxiety, memory disturbances, and intrusive thoughts. Imaging studies have consistently found degenerative changes in the brains of victims, particularly in the hippocampus. Thus, we see that the release of hypophysiotropic hormones by cells in the secretory hypothalamus can produce widespread alterations in the physiology of both the body and the brain (Box 15. From the Greek autonomia (roughly meaning "independence"), autonomic functions are usually carried out automatically, without conscious, voluntary control. You are faced with a classic fight-or-flight situation, and your body reacts accordingly, even as your conscious mind frantically considers whether to blunder through it or beg off in humiliation. Within a few minutes, your sympathetic responses decrease to low levels, and the functions of your parasympathetic division crank up again: Your heart rate slows and blood pressure drops, digestive functions work harder on breakfast, and you stop sweating.
Syndromes
The basic template of the diagnosis-based grid is common to each organ system and chapter; therefore although there is variation in the ancillary factors used to develop the impairment rating (depending on the body part), there is greater internal consistency between chapters than was seen formerly. This uniform diagnosis-based approach is a significant change from the anatomical approach that was the primary approach with many previous musculoskeletal assessments. However, there are similarities to other approaches used in the Fourth and Fifth Editions. For example, as mentioned previously, spinal impairment assessments have typically been based on the Diagnosis-Related Estimates Method, with specific findings or diagnoses used to assign the patient to a category. In the Fifth Edition the patient is assigned to one of five categories, with the first category having no ratable impairment and the other four categories having four possible impairment values. Likewise, although lower extremity impairments had been based on thirteen possible approaches in the Fifth Edition, the most commonly used approach is the Diagnosis-Based Estimates where specific impairment values are provided for diagnoses. For example, a patient with a partial medial meniscectomy is assigned 1% whole person permanent impairment. Rating systems previously used for the lower extremity likewise did not provide for adjustments based on functional difficulties, physical examination findings, or the results of clinical studies. The Preface to the Sixth Edition states that the features of the new edition include 22: A standardized approach across organ systems and chapters. The latest scientific research and evolving medical opinions provided by nationally and internationally recognized experts. Unified methodology that helps physicians calculate impairment ratings through a grid construct and promotes consistent scoring of impairment ratings. Precise documentation of functional outcomes, physical findings, and clinical test results, as modifiers of impairment severity. The Sixth Edition reflects movement toward these features; however such change will not be immediately achieved. Thus it should be considered a step in the evolution of the Guides rather than as an end point in and of itself. The process was guided by an Editorial Panel and an Advisory Committee, and features an open, well-defined, and tiered, peer review process. The editorial process used an evidence-based foundation when possible, primarily as the basis for determining diagnostic criteria, and a Delphi panel approach to consensus building regarding the impairment ratings themselves. When there was not a compelling rationale to alter impairment ratings from what they had -7- The Section Editors led a group of 53 specialty-specific, expert contributors in developing the chapters and in conjunction with the Senior Contributing Editor wrote considerable portions of the revised chapters. The review process involved over 140 physicians, attorneys and other professionals. An Advisory Committee was developed to provide ongoing discussion of items of mutual concern and current issues in impairment and disability. Provide documentation to staff and the Editorial Panel regarding the medical appropriateness of changes under consideration for inclusion in the Guides. Assist in the review and further development of relevant impairment issues and in the preparation of technical education material and articles pertaining to the Guides. Sixth Edition Structure the Sixth Edition is 634 pages in length and is comprised of 17 chapters; it is similar in length to the Fifth Edition (613 pages) and has one less chapter since the Cardiovascular System is now a single chapter. Chapter 1, Conceptual Foundations and Philosophy and Chapter 2, Practical Applications of the Guides define the overall approaches to assessing impairment. Most impairment ratings are performed for musculoskeletal painful conditions; therefore the most commonly used chapters will be Chapter 15, the Upper Extremities, Chapter 16, the Lower Extremities, and Chapter 17, the Spine and Pelvis. Chapter 3, Pain-Related Impairment, Chapter 13, the Central and Peripheral Nervous System and Chapter 14, Mental and Behavioral Disorders will also be frequently referenced. To appreciate the overall impact of the Sixth Edition it is helpful to summarize the chapters most often referenced, the first two chapters, the musculoskeletal chapters, and the chapters on the nervous system and mental and behavioral disorders. Impairment Rating Values the Sixth Edition reflects very substantial change, a change more significant than any prior Edition change. With the Sixth Edition the impairment values for the most frequently used impairments and diagnoses are similar to the Fifth. However, some adjustments were required, with certain ratings being lower and others higher. There are conditions that did not receive ratable impairment in the past (such as lateral epicondylitis and non-specific spinal pain) which in certain circumstances may now be ratable as Class 1 (mild) impairments. Sixth Edition ratings are based more on the end-result and the impact on the patient, rather than what types of treatments or surgeries have been performed.
Severe loss (up to 5% annually) is observed in parietal, motor and anterior temporal cortex. The mesocorticolimbic dopamine system, which arises in the ventral tegmental area, has been implicated in the cause of schizophrenia. A second dopaminergic system arising from the substantia nigra is involved in the control of voluntary movement by the striatum. Indeed, these same drugs are effective in the treatment of amphetamine and cocaine psychoses. According to the dopamine hypothesis of schizophrenia, psychotic episodes in schizophrenia are triggered specifically by the activation of dopamine receptors. The neuroleptic dosages effective in controlling schizophrenia correlate well with the binding affinities of the drugs for D2 receptors. The units on the Y axis are the molar concentrations of drug that inhibit half of the D2 receptors in the brain. One indication is that newly developed antipsychotic drugs, like clozapine, have little effect on D2 receptors. These drugs are called atypical neuroleptics, indicating that they act in a novel way. The mechanism by which these compounds exert their neuroleptic effect has not been established with certainty, but an interaction with serotonin receptors is suspected. However, many patients experienced adverse side effects, sometimes lasting for days, which included hallucinations and paranoia. However, neither drug has an effect on dopaminergic transmission; they affect synapses that use glutamate as a neurotransmitter. In order to study the neurobiology of schizophrenia, neuroscientists have attempted to establish animal models of the disorder. The photographs were taken 30 minutes apart over 2 hours to monitor social behavior. But it is significant that the observable behavioral abnormalities can be lessened by treating the mice with either conventional or atypical neuroleptic drugs. Notably, postmortem examination of the brains of individuals with schizophrenia has found the cortex to be deficient in many interneurons. As mentioned earlier, the conventional neuroleptics, such as chlorpromazine and haloperidol, act at D2 receptors. These drugs reduce the positive symptoms of schizophrenia in the majority of patients. Unfortunately, the drugs also have numerous side effects related to their actions on the dopaminergic input to the striatum that arises from the substantia nigra (see Chapter 14). Chronic treatment with conventional neuroleptics also can result in the emergence of tardive dyskinesia, which is characterized by involuntary movements of the lips and jaw. Many of these side effects are avoided by using atypical neuroleptics, such as clozapine and risperidone, because they do not act directly on the dopamine receptors in the striatum. These medications are also more effective against the negative symptoms of schizophrenia. Mental illness is now recognized as the consequence of pathologic modifications of the brain, and psychiatric treatments today are focused on correcting these changes. Just as importantly, neuroscience has changed how society views people who suffer from mental illness. Mental illnesses today are recognized as diseases of the body, just like hypertension or diabetes. Despite remarkable progress in treating psychiatric disorders, we have a very incomplete understanding of how current treatments work their magic on the brain. In the case of drug therapy, we know with great precision about how chemical synaptic transmission is affected. But we do not know why, in many cases, the therapeutic effect of a drug takes weeks to emerge. In general, the answer seems to lie in adaptive changes that occur in the brain in response to treatment. Environmental stresses before birth may contribute to schizophrenia, and those after birth may precipitate depression.
To understand laparoscopic and laparoscopically assisted vascular techniques for both arterial, venous and adjunctive vascular procedures. To understand the role of brachytherapy in preventing intimal hyperplasia, both as an independent modality or in combination with metallic devices. To understand and have a working knowledge of endovascular and interventional techniques utilizing percutaneous and surgical access for the diagnosis, management and treatment of traumatic arterial and venous injuries. To understand and have a working knowledge of endovascular and interventional techniques utilizing percutaneous and surgical access for the diagnosis, management and treatment of arterial occlusive disease. To understand and have a working knowledge of endovascular and interventional techniques utilizing percutaneous and surgical access for the diagnosis, management and treatment of aneurysmal disease. To understand and have a working knowledge of endovascular and interventional techniques utilizing percutaneous and surgical access for the diagnosis, management and treatment of cerebrovascular disease. To understand and have a working knowledge of endovascular and interventional techniques utilizing percutaneous and surgical access for the diagnosis, management and treatment of venous disease including arteriovenous malformations. To understand the pathophysiology and management of intimal hyperplasia and recurrent disease after endovascular intervention, endovascular graft placement and insertion of an implantable device. To understand the treatment of acute and chronic complications of endovascular techniques and devices. To understand the pathophysiology and management of arterial injuries, endoleaks, migration, embolization, delivery system failures and attachment device failures. To have a working knowledge of recovery, retrieval and " out" bail procedures for endovascular procedures. Graduate Medical Education Directory 1993-1994, ed 79, Chicago, 1993, American Medical Association. Recognize the frequent association of coronary artery and peripheral vascular disease. Understand the risk factors predictiveof perioperative myocardial infarction or cardiac death. Be familiar with the early and late cardiac mortality figures following major vascular surgery. Understand the clinical significance of chronic stable angina, unstable angina, recent and remote myocardial infarction and congestive heart failure 3. Understand how an imbalance of myocardial oxygen supply and demand may lead to myocardial ischemia 4. Describe those factors that may lead to an increased demand for myocardial oxygen, and/or a decreased supply that will contribute to myocardial ischemia. Understand the clinical and histological difference between a subendocardial and transmural infarction. Understand the effects of general and regional anesthesia on myocardial oxygen demand and myocardial ischemia. Understand the most important factors present intraoperatively and in the post-operative period that contribute to myocardial ischemia. Understand the signs and symptoms of chronic stable angina, unstable angina, myocardial infarction and congestive heart failure. Know the risks of operation in a patient with a recent myocardial infarction, unstable angina, or poorly compensated congestive heart failure. Be familiar with the currently used methods for screening for coronary artery disease, and their limitations. Dipyridamole thallium scanning, Exercise testing, Dobutamine stress echo, ambulatory Holter monitoring) 4. Know which patients should undergo a preoperative test for coronary artery disease 5. Understand that the magnitude of the operation should be tailored to the severity of the patients cardiac risk. Know when to employ an extra anatomic, or limited procedure instead of an intra-abdominal operation. Understand the reasons for controlling myocardial ischemia intraoperatively, and during recovery from a major vascular operation 62 5.
References:




