Tobler W, Gerszten P, Bradley W, Raley T, Nasca R, Block J: Minimally-invasive Axial Pre-sacral L5-S1 Interbody Fusion: Two Year Clinical and Radiographic Outcomes. Complications and radiographic correction in adult scoliosis following combined transpsoas extreme lateral interbody fusion and posterior pedicle screw instrumentation. An evidencebased clinical guidelines for the diagnosis and treatment of degenerative lumbar spondylolisthesis. Clinical outcomes of the Dynesys dynamic neutralization system: 1-year preliminaryresults. Short-term preoperative smoking cessation and postoperative complications: a systematic review and meta-analysis. Minimal Access Versus Open Transforaminal Lumbar Interbody Fusion: Meta-Analysis of Fusion Rates. Biomechanical evaluation of the Total Facet Arthroplasty System: 3-dimensional kinematics. Treatment of symptomatic adjacentsegment degeneration after lumbar fusion with total disc arthroplasty by using the ProDisc prosthesis: a prospective study with 2-year minimum follow up. Lumbar total disc arthroplasty utilizing the ProDisc prosthesis in smokers versus nonsmokers. The treatment of disabling single-level lumbar discogenic low back pain with total disc arthroplasty utilizing the ProDisc Prosthesis. Artificial interverterbal disc arthroplasty for treatment of degenerative disc disease of the cervical spine. Interventional techniques in the management of chronic spinal pain: evidencebased practice guidelines. Long-term results of one-level lumbar arthroplasty: minimum 10-year followup of the Charite artificial disc in 106 patients. A Comparison of Five Low Back Disability Questionnaires: Reliability and Responsiveness: Phys Ther: 2002; 82: 8-24Di Silvestre M, Bakaloudis G, Lolli F, Vommaro F, Parisini P. Review Article: Posterior Lumbar Fusion: Choice of Approach and Adjunct Techniques. Patient selection for lumbar arthroplasty and arthrodesis: the effect of revision surgery in a controlled, multicenter, randomized study. Total disc replacement in the lumbar spine: a systematic review of the literature. Effect of previous surgery on clinical outcome following 1-level lumbar arthroplasty. Effect of age on clinical and radiographic outcomes and adverse events following 1 level lumbar arthroplasty after a minimum 2 year follow-up. ProDisc-L total disc replacement: a comparison of 1-level versus 2-level arthroplasty patients with a minimum 2-year follow-up. Sensitivity of Magnetic Resonance Imaging in the Diagnosis of Mobile and Non-Mobile L4-5 Degenerative Spondylolisthesis. Comparison of results of total disc replacement in postdiscectomy patients versus patients with no previous lumbar surgery. Revision and Explantation Strategies Involving the Lumbar Artificial Disc Replacement. Influence of Facet and Posterior Muscle Degeneration on Clinical Results of Lumbar Total Disc Replacement: Two-Year Follow-Up. The effect of single-level, total disc arthroplasty on sagittal balance parameters: a prospective study. Subsidence and malplacement with the Oblique Maverick Lumbar Disc Arthroplasty: technical note. Systematic Review of Randomized Trials Comparing Lumbar Fusion Surgery to Nonoperative Care for Treatment of Chronic Back Pain. Clinical Outcome of Lumbar Total Disc Replacement Using ProDisc-L in Degenerative Disc Disease: Minimum 5-year Follow-up Results at a Single Institute. In vivo study of the kinematics in axial rotation of the lumbar spine after total intervertebral disc replacement: long-term results: a 10-22 years follow-up evaluation. Clinical and Radiological Mid-Term Outcomes of Lumbar Single-Level Total Disc Replacement. Analysis of post-operative pain patterns following total lumbar disc replacement: results from fluoroscopically guided spine infiltrations.
These serious health problems may happen if you take Epogen, even if you do not have an increase in your hemoglobin level. Epogen should not be used for treatment of anemia: If you have cancer and you will not be receiving chemotherapy that may cause anemia. It is not known if Epogen is safe and effective in treating anemia in children less than 1 month old who have chronic kidney disease and in children less than 5 years old who have anemia caused by chemotherapy. Do not take Epogen if you: Have cancer and have not been counseled by your healthcare provider about treatment with Epogen. Talk to your healthcare provider about possible pregnancy and birth control choices that are right for you. Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. If you or your caregiver has been trained to give Epogen shots (injections) at home: o Be sure that you read, understand, and follow the "Instructions for Use" that come with Epogen. Do not change the dose of Epogen unless told to do so by your healthcare provider. Epogen may cause serious side effects, including: See "What is the most important information I should know about Epogen High blood pressure is a common side effect of Epogen in people with chronic kidney disease. Your blood pressure may go up or be difficult to control with blood pressure medicine while taking Epogen. If your blood pressure does go up, your healthcare provider may prescribe new or more blood pressure medicine. If you have any seizures while taking Epogen, get medical help right away and tell your healthcare provider. Serious allergic reactions can cause a skin rash, itching, shortness of breath, wheezing, dizziness and fainting because of a drop in blood pressure, swelling around your mouth or eyes, fast pulse, or sweating. If you have a serious allergic reaction, stop using Epogen and call your healthcare provider or get medical help right away. Signs and symptoms of severe skin reactions with Epogen may include: skin rash with itching, blisters, skin sores, peeling, or areas of skin coming off. If you have any signs or symptoms of a severe skin reaction, stop using Epogen and call your healthcare provider or get medical help right away. Dangers of using Epogen from multiple-dose vials in newborns, infants, and pregnant or breastfeeding women. Do not use Epogen from multiple-dose vials in newborns, infants, pregnant or breastfeeding women because the Epogen in these vials contains benzyl alcohol. If you use Epogen from multiple-dose vials you should not breastfeed for at least 2 weeks after the last dose. Throw away multiple-dose vials of Epogen no later than 21 days from the first day that you put a needle into the vial. General information about Epogen Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not give Epogen to other people even if they have the same symptoms that you have. You can ask your healthcare provider or pharmacist for information about Epogen that is written for healthcare professionals. Active ingredient: epoetin alfa Inactive ingredients: Multiple-dose vials contain benzyl alcohol. All vials contain albumin (human), citric acid, sodium chloride, sodium citrate, and Water for Injection. Food and Drug Administration Revised: 9/2017 Instructions for Use Epogen (Ee-po-jen) (epoetin alfa) Use these Instructions for Use if you or your caregiver has been trained to give Epogen injections at home. If you are not sure about giving the injection or you have questions, ask your healthcare provider for help. Before reading these Instructions for Use, read the Medication Guide that comes with Epogen for the most important information you need to know. When you receive your Epogen vial and syringes make sure that: the name Epogen appears on the carton and vial label. The dose strength of the Epogen vial (number of Units per mL on the vial label) is the same as your healthcare provider prescribed.
Diseases
If the patient is not exhibiting other symptoms, such as weakness, fatigue, dizziness, fainting, chest discomfort, palpitations, or respiratory distress, bradycardia is not considered clinically significant. However, if any of these symptoms are present, they may indicate that the heart is not providing sufficient oxygenated blood to the tissues. Bradycardia may be caused by either inherent factors or causes external to the heart. While the condition may be inherited, typically it is acquired in older individuals. Other causes include ischemia to the heart muscle or diseases of the heart vessels or valves. Treatment relies upon establishing the underlying cause of the disorder and may necessitate supplemental oxygen. Tachycardia is not normal in a resting patient but may be detected in pregnant women or individuals experiencing extreme stress. In the latter case, it would likely be triggered by stimulation from the limbic system or disorders of the autonomic nervous system. Some individuals may remain asymptomatic, but when present, symptoms may include dizziness, shortness of breath, lightheadedness, rapid pulse, heart palpations, chest pain, or fainting (syncope). Treatment depends upon the underlying cause but may include medications, implantable cardioverter defibrillators, ablation, or surgery. The cardioaccelerator regions stimulate activity via sympathetic stimulation of the cardioaccelerator nerves, and the cardioinhibitory centers decrease heart activity via parasympathetic stimulation as one component of the vagus nerve, cranial nerve X. During rest, both centers provide slight stimulation to the heart, contributing to autonomic tone. Both sympathetic and parasympathetic stimulations flow through a paired complex network of nerve fibers known as the cardiac plexus near the base of the heart. The ventricles are more richly innervated by sympathetic fibers than parasympathetic fibers. It opens chemical- or ligand-gated sodium and calcium ion channels, allowing an influx of positively charged ions. Overprescription of these drugs may lead to bradycardia and even stoppage of the heart. They innervate the heart via sympathetic cardiac nerves that increase cardiac activity and vagus (parasympathetic) nerves that slow cardiac activity. Parasympathetic stimulation originates from the cardioinhibitory region with impulses traveling via the vagus nerve (cranial nerve X). Input to the Cardiovascular Center the cardiovascular center receives input from a series of visceral receptors with impulses traveling through visceral sensory fibers within the vagus and sympathetic nerves via the cardiac plexus. Among these receptors are various proprioreceptors, baroreceptors, and chemoreceptors, plus stimuli from the limbic system. Collectively, these inputs normally enable the cardiovascular centers to regulate heart function precisely, a process known as cardiac reflexes. Increased physical activity results in increased rates of firing by various proprioreceptors located in muscles, joint capsules, and tendons. Any such increase in physical activity would logically warrant increased blood flow. The cardiac centers monitor these increased rates of firing, and suppress parasympathetic stimulation and increase sympathetic stimulation as needed in order to increase blood flow. Similarly, baroreceptors are stretch receptors located in the aortic sinus, carotid bodies, the venae cavae, and other locations, including pulmonary vessels and the right side of the heart itself. Rates of firing from the baroreceptors represent blood pressure, level of physical activity, and the relative distribution of blood. The cardiac centers monitor baroreceptor firing to maintain cardiac homeostasis, a mechanism called the baroreceptor reflex. With increased pressure and stretch, the rate of baroreceptor firing increases, and the cardiac centers decrease sympathetic stimulation and increase parasympathetic stimulation. As pressure and stretch decrease, the rate of baroreceptor firing decreases, and the cardiac centers increase sympathetic stimulation and decrease parasympathetic stimulation.
Inasmuch as Jezerinac (1983) and Thoma (1982), who are currently investigating the subspecies of Cambarus bartonii, continue to recognize the two non-nominate subspecies, the two taxa are provisionally retained herein. They did not mention the populations in the Kanawha Basin of Virginia and West Virginia that formerly have been assigned to this species. Bartonius ortmanni Williamson, 1907:749 [Bartonius intended as a subgeneric name]. Subgenus Erebicambarus Hobbs, 1969b:99 [Type species, by original designation, Cambarus barloni tenebrosus Hay, 19O2a:232. Until such a study is conducted, I deem it advisable to maintain specific status for it. Jezerinac and Thoma (1984:121) omitted this crayfish in their key to the genera Cambarus and Fallicambarus in Ohio because all of the material that they examined from the state that had been assigned to C. Subgenus Exilicambarus Bouchard and Hobbs Subgenus Exilicambarus Bouchard and Hobbs, 1976:2. Possibly the dominant Hiaticambarus in the upper Coosa Basin in Alabama is referable to this species. Restricted to Doe River, Elizabethton, Carter County, Tennessee, designated by Ortmann, 1931:121. Emended by Hobbs (1967a:129) to Rockfish River, south of Afton, Nelson County, Virginia. This crayfish has also been collected from tributaries of the Little River (Chattooga-Coosa Basin) in the northwestern part of Chattooga County, Georgia. Even in the Santee Cooper Basin (of which the Saluda River is a tributary), South Carolina, more than one rather distinct "variant" is recognizable. Cambarus Cambarus Cambarus Cambarus Cambarus Cambarus Cambarus extraneus Hagen, 1870:73, pi. Its presence in New England east of the Hudson River basin is believed to have resulted from introductions (Douglas G. Cambarus Cambarus Cambarus Cambarus Cambarus bartonii veteranus Faxon 1914:389, pi. Procambarus (Distocambarus) devexus Hobbs, 1981:302, figs, l l j, 105, 115-117,234. Tammany Parish, Louisiana, and Forest, Hancock, Harrison, Jackson, and Pearl River counties in southern Mississippi eastward to Baldwin County, Alabama. A study is needed to ascertain whether or not current records for Missouri, Arkansas, and Oklahoma are based on correct identifications. Type locality, streams from John Ross Spring, near Rossville, Walker County, Georgia. Unfortunately, his samples were quite limited both in quantity and in representing the range of the complex. Probably Hagen erred in recording the specimen from Belleville as having been catalogued under number 1841. Newlon from the type locality and were received from the Kansas Museum of Natural History; presumably they represent a part of the lot that was said by Faxon (1914:420) to have been at Washburn College. Introduced into California (Riegel, 1959:29, 37); Maryland (Meredith and Schwartz, 1960:28); parts of New England (Crocker, 1979:247; D. Smith, 1979:388); Alabama, Tennessee, Mississippi, and West Viginia (Bouchard, 1976a:583); Utah (Johnson, 1986:630); New York (Crocker, 1979:247); Chihuahua, Mexico (Campos and Contreras, 1985:218); and Pennsylvania (specimen in National Museum of Natural History from Adams County). Specimens from Coal County, Oklahoma, were interpreted by Walls (1972) as intergrades between this crayfish and 0. Subgenus Procericambarus Fitzpatrick, 1987a:57 [Type species, by original designation, Cambarus forceps Faxon, 1884:133. Cambarus stygius Joseph, 1881:241 [nomen nudum]; 1882:12 [validation of nomen nudum of 1881, becoming homonym of Cambarus stygius Bundy (= Procambarus acutus acutus (Girard)); see Holthuis, 1964]. Orconectes (Procericambarus) luteus (Creaser) nounitt Faxonius (Faxonius) luteus Creaser, 1933b:7, pi.
Decompression and coflex interlaminar stabilization compared with decompression and instrumented spinal fusion for spinal stenosis and low-grade degenerative spondylolisthesis. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. Morbidity and mortality in the surgical treatment of 10,329 adults with degenerative lumbar stenosis. Evaluation of interspinous spacer outcomes in degenerative lumbar canal stenosis: clinical study. Nonoperative treatment of spondylolysis and grade I spondylolisthesis in children and young adults: a meta-analysis of observational studies. Evidence-based clinical guidlines for multidisciplinary spine care [Internet] North American Spine Society. Role of coflex as an adjunct to decompression for symptomatic lumbar spinal stenosis. Utility of repeat magnetic resonance imaging in surgical patients with lumbar stenosis without disc herniation. Successful outcome after outpatient transforaminal decompression for lumbar foraminal and lateral recess stenosis: the positive predictive value of diagnostic epidural steroid injection. Minimially invasive decompression versus X-Stop in lumbar spinal stensosis: a randomized controlled multicenter study. Interspinous process device versus standard conventional surgical decompression for lumbar spinal stenosis: randomized controlled trial. Evaluation of decompression and interlaminar stabilization compared with decompression and fusion for the treatment of lumbar spinal stenosis: 5year follow-up of a prospective, randomized, controlled trial. The increase in dural sac area is maintained at 2 years after X-stop implantation for the treatment of spinal stenosis with no significant alteration in lumbar spine range of movement. Perioperative outcomes, complications, and costs associated with lumbar spinal fusion in older patients with spinal stenosis and spondylolisthesis. Superion interspinous spacer for treatment of moderate degenerative lumbar spinal stenosis: durable three-year results of a randomized controlled trial. Interspinous device versus laminectomy for lumbar spinal stenosis: a comparative effectiveness study. Minimally invasive discectomy versus microdiscectomy/open discectomy for symptomatic lumbar disc herniation. Two-year follow-up after decompressive surgery with and without implantation of an interspinous device for lumbar spinal stenosis: a prospective controlled study. Superior outcomes of decompression with an interlaminar dynamic device versus decompression alone in patients with lumbar spinal stenosis and back pain: a cross registry study. Morbidity and mortality in the surgical treatment of 10,242 adults with spondylolisthesis. Prospective, randomized, multicenter study with 2-year follow-up to compare the performance of decompression with and without interlaminar stabilization. The positional magnetic resonance imaging changes in the lumbar spine following insertion of a novel interspinous process distraction device. Outcome after less-invasive decompression of lumbar spinal stenosis: a randomized comparison o. Canadian Journal of Anaesthesia 2010;57(7):694-703f unilateral laminotomy, bilateral laminotomy, and laminectomy. An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spondylolisthesis. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. Interspinous spacer versus traditional decompressive surgery for lumbar spinal stenosis: a systematic review and meta-analysis. Surgical versus nonoperative treatment for lumbar spinal stenosis four-year results of the Spine Patient Outcomes Research Trial.
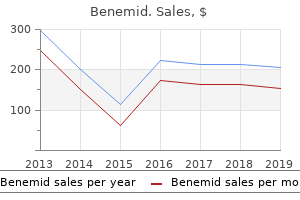
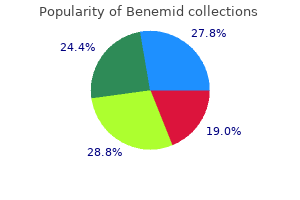
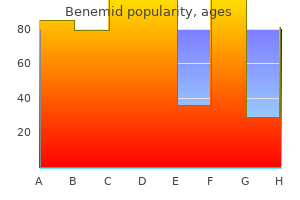
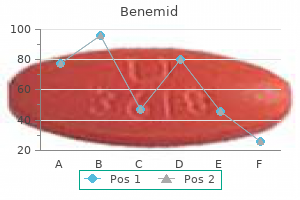
Potentilla erecta (Tormentil). Benemid.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96372
Screens must realize their own personal limitations and seek assistance from the medical officer whenever any doubt exists. It is generally accepted practice during peak periods of sick-call to assign one medic to obtain and record designated vital signs. The medic assigned to take vital signs must be aware of their significance and adhere to the following guidelines. In young pediatric patients, or unconscious adult patients a rectal temperature will be necessary. Clothing that must be rolled up tightly over the arm to allow access to the antecubital space may easily produce false readings and should be removed. If the first measurement is slightly elevated and the patient has just arrived in the clinic, it is suggested that the measurement be repeated after several minutes of rest. Respiratory distress in an adult would be a rate greater that 24 or less than 10 breaths per minute. Some electronic machines will also count the pulse while obtaining a blood pressure. Every patient reporting for treatment must be questioned concerning past allergic reactions to medications and the information documented. Failure to adequately establish and document a history of an allergic condition may result in the patient suffering a severe allergic reaction or a potentially fatal anaphylactic reaction. It is extremely important to establish and document what medication(s) a patient is currently using. It is best to obtain and document current medications at the same time as the history of allergies. A proper history of current medications includes not only prescription drugs such as blood pressure mediations or antibiotics but must include all over-the-counter type remedies as will. Medics unfamiliar with standard pharmacy abbreviations should describe the dosage and schedule in longhand. In general, any patient with a history of chronic disease or illness should be referred to a medical officer. It should be noted that this portion of the patient interview is the most significant contribution in providing quality patient care. The existence of certain complaints, circumstances, or methods of injury can often lead the medic to concentrate on a specific part of the physical examination, and may greatly influence the final assessment and treatment plan. You should ask about alcohol consumption and document what kind of alcohol, how much is consumed and when. You can calculate pack years by multiplying the number of cigarette packs smoked per day times the number of years the patient is smoking. For example, a 30 year old female smokes 2 packs of cigarettes a day for 20 years, she would have a 40 pack year smoking history! An example of a good subject history for a 21 year old male who injured his right ankle would be S 21 y/o male presents c/o of a sprained right ankle x 24 hours. Patient injured ankle yesterday by stepping into a hole while running Patient heard a "snap" and can only ambulate with assistance Patient returned to his barracks hoping to "sleep it off" but decided to come in after his ankle swelled and turned blue. An appropriate objective note will demonstrate that the care provider has performed at least those parts of the physical examination which are relevant to the chief complaint, and should adhere to the guidelines listed under each complaint in this manual. The assessment should reflect your findings during the history and your examination. It is assumed that the art of arriving at more specific diagnoses will develop with experience. It should be remembered that the foundation of quality medical care rests on a complete history and physical exam, and is only supported by laboratory results. If a patient presents with a condition significant enough to warrant an x-ray, the medic should at a minimum, consult with the medical officer prior to ordering the study. Antacids (Maalox, Maalox plus) Antihistamines (25mg Benadryl/Actifed tablets) Aspirin Analgesic balm (Ben Gay) Anesthetic ointment (Nupercainal ointment Antidandruff shampoo (Sebutone, Coal Tar) Antifungal foot ointment, powder, or solution (Desenex products, Lotrimin solution/cream) 8. Tyenol If at any time you have a question about a medication, always ask a medical officer. Profiles should be written in not-medical language and should be specific concerning physical limitations. Profiles which contain such terms as (X 14 hrs) or (X 3 days) may be misunderstood particularly if the patient was seen in the afternoon or on a Friday.
Given the importance of oxytocin and prostaglandins to the initiation and maintenance of labor, it is not surprising that, when a pregnancy is not progressing to labor and needs to be induced, a pharmaceutical version of these compounds (called pitocin) is administered by intravenous drip. Finally, stretching of the myometrium and cervix by a full-term fetus in the vertex (head-down) position is regarded as a stimulant to uterine contractions. The sum of these changes initiates the regular contractions known as true labor, which become more powerful and more frequent with time. The pain of labor is attributed to myometrial hypoxia during uterine contractions. Stages of Childbirth the process of childbirth can be divided into three stages: cervical dilation, expulsion of the newborn, and afterbirth (Figure 28. However, it varies widely and may take minutes, hours, or days, depending in part on whether the mother has given birth before; in each subsequent labor, this stage tends to be shorter. Cervical stretching induces reflexive uterine contractions that dilate and efface the cervix further. In addition, cervical dilation boosts oxytocin secretion from the pituitary, which in turn triggers more powerful uterine contractions. For this reason, it is critical that a period of relaxation occur after each contraction. Fetal distress, measured as a sustained decrease or increase in the fetal heart rate, can result from severe contractions that are too powerful or lengthy for oxygenated blood to be restored to the fetus. Such a situation can be cause for an emergency birth with vacuum, forceps, or surgically by Caesarian section. The amniotic membranes rupture before the onset of labor in about 12 percent of women; they typically rupture at the end of the dilation stage in response to excessive pressure from the fetal head entering the birth canal. It typically takes up to 2 hours, but it can last longer or be completed in minutes, depending in part on the orientation of the fetus. The vertex presentation known as the occiput anterior vertex is the most common presentation and is associated with the greatest ease of vaginal birth. The fetus faces the maternal spinal cord and the smallest part of the head (the posterior aspect called the occiput) exits the birth canal first. In fewer than 5 percent of births, the infant is oriented in the breech presentation, or buttocks down. Before the 1960s, it was common for breech presentations to be delivered vaginally. Vaginal birth is associated with significant stretching of the vaginal canal, the cervix, and the perineum. Until recent decades, it was routine procedure for an obstetrician to numb the perineum and perform an episiotomy, an incision in the posterior vaginal wall and perineum. Both an episiotomy and a perineal tear need to be sutured shortly after birth to ensure optimal healing. Although suturing the jagged edges of a perineal tear may be more difficult than suturing an episiotomy, tears heal more quickly, are less painful, and are associated with less damage to the muscles around the vagina and rectum. Afterbirth the delivery of the placenta and associated membranes, commonly referred to as the afterbirth, marks the final stage of childbirth. Continued uterine contractions then reduce blood loss from the site of the placenta. If the placenta does not birth spontaneously within approximately 30 minutes, it is considered retained, and the obstetrician may attempt manual removal. It is important that the obstetrician examines the expelled placenta and fetal membranes to ensure that they are intact. If fragments of the placenta remain in the uterus, they can cause postpartum hemorrhage. Although postpartum uterine contractions limit blood loss from the detachment of the placenta, the mother does experience a postpartum vaginal discharge called lochia. This is made up of uterine lining cells, erythrocytes, leukocytes, and other debris.
The femoral artery also gives rise to the genicular artery, which provides blood to the region of the knee. As the femoral artery passes posterior to the knee near the popliteal fossa, it is called the popliteal artery. The anterior tibial artery is located between the tibia and fibula, and supplies blood to the muscles and integument of the anterior tibial region. Upon reaching the tarsal region, it becomes the dorsalis pedis artery, which branches repeatedly and provides blood to the tarsal and dorsal regions of the foot. The posterior tibial artery provides blood to the muscles and integument on the posterior surface of the tibial region. It bifurcates and becomes the medial plantar artery and lateral plantar artery, providing blood to the plantar surfaces. There is an anastomosis with the dorsalis pedis artery, and the medial and lateral plantar arteries form two arches called the dorsal arch (also called the arcuate arch) and the plantar arch, which provide blood to the remainder of the foot and toes. Arteries Serving the Lower Limbs Vessel Femoral artery Deep femoral artery Lateral circumflex artery Description Continuation of the external iliac artery after it passes through the body cavity; divides into several smaller branches, the lateral deep femoral artery, and the genicular artery; becomes the popliteal artery as it passes posterior to the knee Branch of the femoral artery; gives rise to the lateral circumflex arteries Branch of the deep femoral artery; supplies blood to the deep muscles of the thigh and the ventral and lateral regions of the integument Genicular artery Branch of the femoral artery; supplies blood to the region of the knee Popliteal artery Anterior tibial artery Table 20. Since the blood has already passed through the systemic capillaries, it will be relatively low in oxygen concentration. In many cases, there will be veins draining organs and regions of the body with the same name as the arteries that supplied these regions and the two often parallel one another. However, there is a great deal more variability in the venous circulation than normally occurs in the arteries. For the sake of brevity and clarity, this text will discuss only the most commonly encountered patterns. However, keep this variation in mind when you move from the classroom to clinical practice. In both the neck and limb regions, there are often both superficial and deeper levels of veins. The superficial veins do not normally have direct arterial counterparts, but in addition to returning blood, they also make contributions to the maintenance of body temperature. When the ambient temperature is warm, more blood is diverted to the superficial veins where heat can be more easily dissipated to the environment. In colder weather, there is more constriction of the superficial veins and blood is diverted deeper where the body can retain more of the heat. The "Voyage of Discovery" analogy and stick drawings mentioned earlier remain valid techniques for the study of systemic veins, but veins present a more difficult challenge because there are numerous anastomoses and multiple branches. It is like following a river with many tributaries and channels, several of which interconnect. Tracing blood flow through arteries follows the current in the direction of blood flow, so that we move from the heart through the large arteries and into the smaller arteries to the capillaries. From the capillaries, we move into the smallest veins and follow the direction of blood flow into larger veins and back to the heart. If you draw an imaginary line at the level of the diaphragm, systemic venous circulation from above that line will generally flow into the superior vena cava; this includes blood from the head, neck, chest, shoulders, and upper limbs. The exception to this is that most venous blood flow from the coronary veins flows directly into the coronary sinus and from there directly into the right atrium. Beneath the diaphragm, systemic venous flow enters the inferior vena cava, that is, blood from the abdominal and pelvic regions and the lower limbs. The Superior Vena Cava the superior vena cava drains most of the body superior to the diaphragm (Figure 20. On both the left and right sides, the subclavian vein forms when the axillary vein passes through the body wall from the axillary region. It fuses with the external and internal jugular veins from the head and neck to form the brachiocephalic vein. Each vertebral vein also flows into the brachiocephalic vein close to this fusion. These veins arise from the base of the brain and the cervical region this content is available for free at cnx. Each internal thoracic vein, also known as an internal mammary vein, drains the anterior surface of the chest wall and flows into the brachiocephalic vein. Each intercostal vein drains muscles of the thoracic wall, each esophageal vein delivers blood from the inferior portions of the esophagus, each bronchial vein drains the systemic circulation from the lungs, and several smaller veins drain the mediastinal region. Bronchial veins carry approximately 13 percent of the blood that flows into the bronchial arteries; the remainder intermingles with the pulmonary circulation and returns to the heart via the pulmonary veins.
The liver function tests of raised bilirubin and alkaline phosphatase with normal transaminases and albumin suggest obstruction with normal cellular and synthetic function. It confirms moderate intrahepatic biliary duct dilatation and also demonstrates a focal tapered stenosis at the level of the common hepatic duct. The appearances suggest a stricture of the common hepatic duct which may be ischaemic, post inflammatory or neoplastic in nature. The dilated ducts of the left system were punctured under ultrasound guidance, and a guidewire was then manipulated across the hilar stricture and down into the duodenum. A sheath (8F) was inserted to stabilize the position, and contrast was injected through this to perform the cholangiogram. A stent can be passed over the wire and placed across the stenosis to relieve the obstruction and improve patient symptoms. Interventional radiology consultants can use the veins, arteries and biliary ducts to access deep or distal lesions, vessels or organs, often leaving only a pinhole size scar at the site of puncture (often the groin) as a sign of recent treatment. This allows tissue conservation, reduced morbidity and faster recovery for patients. Stenoses and occlusions can be characterized and an expandable balloon is used to improve blood flow. Hickman line, portacath) to avoid the discomfort of recurrent peripheral cannulation and thrombophlebitis. An adjunct to this is chemoembolization, where a chemotherapy agent is instilled directly to a tumour and then the blood vessel is embolized to cause tumour infarction. You expedite the hip ultrasound that has already been arranged due to the risk factors (Figure 15. Screening is done on infants with risk factors that include family history, breech presentation, foot deformities or neuromuscular disorders. Examination features that raise suspicion for hip abnormality include asymmetric groin creases, a click on movement and a click or subluxation on provocation tests. As with all ultrasound, gel is used to couple the ultrasound beam into the soft tissue and allow movement of the probe without loss of image. The baby is placed in the lateral position with the hip flexed and the probe is placed parallel to the ilium (bright line on the left of the image) and the orientation optimized to produce a horizontal image like a golf ball (stippled cartilage of the femoral head) on a tee (cup is the acetebulum, stalk is the ilium). If the golf ball appears to be falling off the tee (upwards on the image), then the femoral head is subluxed and the acetabular cup is shallow. The alpha angle measures the acetabular roof angle with the ilium and normally measures over 60 degrees. The beta angle assesses the prominence of the labrum (cartilaginous flange around the acetabulum). The ultrasound shows a lot of soft tissue detail, including the unossified cartilage as well as the bone, although the anterior bone edge blocks the beam and no deeper structure is seen. Plain radiographs complement this view by demonstrating the bone structure but with very poor soft tissue detail. Ultrasound is the investigation of choice in infants with unossified femoral heads but as the ossification centre develops and blocks the ultrasound from about 6 months onwards, radiographs are more useful. The aim is to diagnose a hip abnormality as soon as possible to minimize the degree of intervention required to fix the problem. Treatment ranges from observing (if very mild and picked up on a neonatal scan) to braces or surgical intervention. Her wrist appears deformed, but she tells you that although it hurts, the wrist has had that appearance for a long time and that it was investigated at another hospital many years ago. She gives a family history of bone problems but is otherwise well with no medical problems. Examination On the volar aspect of the right forearm just proximal to the wrist there is a firm swelling that extends laterally. Given the history you also briefly examine the arms and spine that appear normal and the legs. The bone around the knees is prominent, with an asymptomatic bony nodule over the lateral aspect of the proximal right tibia. The bone is well delineated with a narrow zone of transition, an appearance suggesting the lesion is benign.
A basophil has large granules that stain dark blue to purple and a two-lobed nucleus. They are called neutrophils because their granules show up most clearly with stains that are chemically neutral (neither acidic nor basic). The nucleus has a distinct lobed appearance and may have two to five lobes, the number increasing with the age of the cell. Older neutrophils have increasing numbers of lobes and are often referred to as polymorphonuclear (a nucleus with many forms), or simply "polys. Their granules include lysozyme, an enzyme capable of lysing, or breaking down, bacterial cell walls; oxidants such as hydrogen peroxide; and defensins, proteins that bind to and puncture bacterial and fungal plasma membranes, so that the cell contents leak out. Abnormally high counts of neutrophils indicate infection and/or inflammation, particularly triggered by bacteria, but are also found in burn patients and others experiencing unusual stress. A burn injury increases the proliferation of neutrophils in order to fight off infection that can result from the destruction of the barrier of the skin. The nucleus of the eosinophil will typically have two to three lobes and, if stained properly, the granules will have a distinct red to orange color. The granules of eosinophils include antihistamine molecules, which counteract the activities of histamines, inflammatory chemicals produced by basophils and mast cells. Some eosinophil granules contain molecules toxic to parasitic worms, which can enter the body through the integument, or when an individual consumes raw or undercooked fish or meat. Eosinophils are also capable of phagocytosis and are particularly effective when antibodies bind to the target and form an antigen-antibody complex. High counts of eosinophils are typical of patients experiencing allergies, parasitic worm infestations, and some autoimmune diseases. Basophils are the least common leukocytes, typically comprising less than one percent of the total leukocyte count. Basophils contain large granules that pick up a dark blue stain and are so common they may make it difficult to see the two-lobed nucleus. In the past, mast cells were considered to be basophils that left the circulation. However, this appears not to be the case, as the two cell types develop from different lineages. The granules of basophils release histamines, which contribute to inflammation, and heparin, which opposes blood clotting. High counts of basophils are associated with allergies, parasitic infections, and hypothyroidism. The nucleus is simple in shape, sometimes with an indentation but without distinct lobes. There are two major types of agranulocytes: lymphocytes and monocytes (see Figure 18. Lymphocytes are the only formed element of blood that arises from lymphoid stem cells. Although they form initially in the bone marrow, much of their subsequent development and reproduction occurs in the lymphatic tissues. The size range of lymphocytes is quite extensive, with some authorities recognizing two size classes and others three. The three major groups of lymphocytes include natural killer cells, B cells, and T cells. These "nonself" cells include cancer cells, cells infected with a virus, and other cells with atypical surface proteins. B cells and T cells, also called B lymphocytes and T lymphocytes, play prominent roles in defending the body against specific pathogens (disease-causing microorganisms) and are involved in specific immunity. One form of B cells (plasma cells) produces the antibodies or immunoglobulins that bind to specific foreign or abnormal components of plasma membranes.
References:




