Head up tilt-table testing may reveal neurocardiogenic syncope or orthostatic hypotension. Often attacks of unconsciousness remain unexplained and possibly have a psychological basis. Such attacks are often mistaken for a seizure and are referred to as pseudo-seizures or non-epileptic attacks (see page 99). Most patients are easily distracted, have slowed thought processes and a limited concentration span. Perceptual disorders (illusions and hallucinations) may accompany the confused state delirium. This is often associated with withdrawal and lack of awareness or with restlessness and hyperactivity. Primary neurological disorders contribute to only 10% of those patients presenting with an acute confusional state. In the elderly, postoperative disorientation is particularly common and multiple factors probably apply; in these patients the prognosis is good. The clinical manifestations range from a major motor convulsion to a brief period of lack of awareness. The prodrome refers to mood or behavioural changes which may precede the attack by some hours. The aura refers to the symptom immediately before a seizure and will localise the attack to its point of origin within the nervous system. The postictal period refers to the time immediately after the ictus during which the patient may be confused, disorientated and demonstrate automatic behaviours. The stereotyped and uncontrollable nature of the attack is characteristic of epilepsy. It is important to remember that epilepsy is not a single condition; epilepsy can be the symptom of other disorders and there are numerous different epilepsy syndromes. Recent studies in animal models of focal epilepsy suggest a central role for the excitatory neurotransmitter glutamate. This produces a depolarisation shift by activating receptors which in turn facilitate cellular influx of Na+, K+ and Ca2+. Epilepsies have complex inheritance; molecular genetics studies in rarer syndromes with autosomal dominant features have identified genes that code for ion channel subunits, either ligand or voltage gated (Channelopathies). Incidence and course Epilepsy presents most commonly in childhood and adolescence or in those over 65, but may occur for the first time at any age. Supplementary motor area seizures can result in more complicated stereotyped movements often arising from sleep for example cycling movement. Motor symptoms occur concurrently the limb appears weak without involuntary movement. Coronal section through the pons showing medial aspect of the temporal lobe and hippocampus the nature of the attack the content of attacks may vary in an individual patient. Commonly encountered symptoms include: Visceral disturbance: Gustatory (taste) and olfactory (smell) hallucinations, lip smacking, epigastric fullness, choking sensation, nausea, pallor, pupillary changes (dilatation), tachycardia. Motor disturbance: Fumbling movement, rubbing, chewing, semi-purposeful limb movements. A constellation of these symptoms associated with subtle clouding of consciousness characterises a temporal lobe onset seizure. The whole episode may last for seconds but occasionally may be prolonged and a rapid succession or cluster of attacks may occur. Lesions in the hippocampus occur as a result of anoxia or from the convulsion itself and act as a source of further epilepsy. Typically there is an elementary visual hallucination a line or flash prior to a tonic-clonic seizure. When spread occurs to the subcortical structures (thalamus and upper reticular formation) their excitation releases a discharge which spreads back to the cerebral cortex of both hemispheres, resulting in a tonic/clonic seizure. The symptoms before the tonic/clonic convulsion give a clue to the site of the initial discharge (simple partial or complex partial).
These patients have no symptomatic relief while on tetracycline, as opposed to the more common scenario of reduced symptomatology while on tetracycline, with symptoms recurring when tetracycline is stopped. Patients who get no relief while on tetracycline should be treated with erythromycin. Rarely, Trichomonas vaginalis, a common cause of vaginal infections, may be the etiologic agent. If repeated courses of antibiotics fail, consider trying metronidazole (Flagyl), 2 grams p. Warn patient not to drink anything alcoholic for two days afterwards, to avoid a possible Antabuse-like reaction. Usually there are characteristic external lesions to help identify the agent (although dual infections occur), and the severity of dysuria is out of proportion to the usually mild, often mucoid, discharge. This should be done as soon as possible after the onset of symptoms, since viral shedding may only last a few days. It is very doubtful that these agents actually produce symptomatic urethritis in men, although they do occur in transient carrier state. Follow-up and Long-Term Treatment Because potentially serious pathogens are rarely isolated after an initial course of tetracycline, long-term follow-up and management are unclear. It is debatable whether patients who remain asymptomatic after an initial course of treatment require any follow-up. Patients who do not respond to this regimen should have urethral herpes cultures (when symptomatic) and a systematic evaluation for prostatic infection, using the three bottle technique of Meares and Stamey (1968). Such patients should be considered for urologic referral to rule out possible strictures, foreign bodies, or intraurethral lesions. Unless significant lesions are found, it is probably better to simply observe the patient rather than blindly treating with antibiotics. In some patients there comes a time when it is necessary to be reassuring and supportive, but to play down the workup and treatment aspects of the disease. These patients have, perhaps, developed a "genital neurosis" and are focusing on minor nonspecific signs and symptoms. Excessive "milking" of the penis may prolong the symptoms due to mechanical trauma. Chlamydial epididymitis should be treated with the same dose of tetracycline or doxycycline, however treatment should be extended for a total of 10 days. However this can develop in at least three other ways: (1) Oral sex when the oral partner has oral herpetic lesions. There is a prodrome of about four days of dysuria, itching, paresthesias, pain, and in women, a variable vaginal discharge. Symptoms then increase, and small papules briefly appear almost anywhere in the genital area. Within 24 to 48 hours these become pustular, then form ulcerative lesions, which last four to 15 days. Tender inguinal adenopathy appears during the second and third week, which may be prolonged, and may even outlast the ulcers. Individual lesions are usually 2 to 5 mm, shallow, flat, painful, without induration. Fever, headache, malaise, and myalgias are seen in 39 percent of men and 68 percent of women. They peak within the first four days after lesion onset, then resolve over the remainder of the first week. In some cases, hospitalization with supportive treatment for aseptic meningitis is required. Sacral paresthesias, constipation, and urinary retention requiring catheterization occur rarely. Conflicting studies show both a 50 percent reduction in recurrence rates after four to five years, and no reduction.
Diseases
The picture of the typical cell viewed with the electron microscope still shows most of the structures described by light microscopy but in much greater detail. The typical cell seen in light microscopy consists of a nucleus and cytoplasm surrounded by the cell membrane. The nucleus contains a nucleolus and chromatin material, which forms into chromosomes during cell division. The cytoplasm contains a number of structures, or organelles, including the endoplasmic reticulum, Golgi apparatus, mitochondria, and inclusions. According to the fluid mosaic model, the phospholipids are arranged with their polar (hydrophilic) ends facing the protein layers, while their nonpolar (hydrophobic) ends face each other in the center of the membrane. This barrier protects the cell by preventing the simple diffusion of water and water-soluble particles. Plasma membranes contain varying amounts of cholesterol, which is found between the phospholipid molecules and adjusts the fluidity and flexibility of the membrane. The protein composition of the outer cell membrane is extremely variable among different types of cells, and this variation has a great deal of influence on functional differences between cells. Some membrane proteins are firmly inserted into the membrane among the phospholipids. These are integral proteins; they may be arranged so that they extend completely across the membrane. Fluid mosaic model of the cell membrane and proteins associated with the membrane. Intracellular Channel Peripheral Protein Phospholipids the cell and the extracellular fluid surrounding the cell are transmembrane proteins. Many transmembrane proteins are involved in transport processes to move substances across the cell membrane. In Figure 2-8 a transmembrane protein forms a channel to permit passage across the cell membrane. Proteins may also be found bound to the surface of the membrane, and such proteins are classified as peripheral proteins. Most of these are on the cytosolic surface of the membrane, and they are often found bound to an integral protein. The functions of cell membrane proteins include (1) transport of substances across the membrane; (2) provision of a site of binding for substances found in extracellular fluid, such as hormones; (3) contribution to the formation of cell-to-cell junctions; (4) provision of enzymes with active sites facing either the cytosol or the extracellular fluid; and (5) identification or recognition of cell type or cell origin by other cells. Structural modifications of the cell membrane occur largely on the free surface of cells (a surface not adjacent to any other cells). These modifications usually increase the cell surface and presumably function in absorption or secretion. The striated or brush border seen in light microscopy appears in electron micrographs to consist of uniform fingerlike projections called microvilli. Less regular projections, called stereocilia, are irregular branched extensions of the cell cytoplasm that are not motile. Motile cilia (kinocilia) are complex elongated, fingerlike projections from cell surfaces found in areas where material is moved past the surface, as in the linings of the trachea and the uterine tubes. Each cilium is associated with a basal body that resembles a centriole normally seen in the cytoplasm of all cells. Intercellular Contact and Adhesion All vertebrates develop from division of a single cell, the fertilized egg. When the parent cell of a unicellular animal divides, the resulting daughter cells each go their own separate way, but the daughter cells of the fertilized ovum of a multicellular animal stay together and eventually differentiate into cells making up different tissues. The ability of multiple individual cells to remain together and function as a tissue or organ depends on local modifications of the outer cell membrane. In other cases, these modifications connect cells and form a passageway for exchanges between them. The areas of cell membranes involved in intercellular contact and adhesion were named when they were initially examined by light and electron microscopy. In electron micrographs, desmosomes appear as local thickenings of adjacent plasma membranes, with tiny fibrils radiating from the thickening into the cytoplasm of the cell. Desmosomes tightly bind adjacent cells by the interactions between membrane proteins extending out from the surface of the cell membranes.
Each hemipelvis (half a pelvis) comprises three bones, which are fused to form the os coxae, or pelvic bone (Figure 4-11). These two ossa coxarum are firmly attached to one another at the pelvic symphysis ventrally and are joined to the sacrum of the axial skeleton by two strong sacroiliac joints. The three bones entering into the formation of each ox coxae are the ilium, the ischium, and the pubis. All three of these participate in the formation of the acetabulum of the hip joint. It is irregularly triangular, with the apex at the acetabulum and the base projecting craniodorsad. The medial angle, the tuber sacrale, is close to the sacroiliac joint near the midline. The lateral angle, the tuber coxae, is known as the point of the hip (often called the hook bone by cattlemen). A fracture of the tuber coxae in the horse results in obvious asymmetry in the two points of the hips, as viewed from behind. The broad, flat portion between the tuber coxae and tuber sacrale is the wing of the ilium, and the dorsal margin is the iliac crest. The body of the ilium projects ventrad and caudad between the wing and acetabulum and helps form the lateral wall of the pelvic cavity. The ischium projects backward and ventrad from the acetabulum, forming much of the floor of the pelvic cavity. The ischium has a large roughened caudal prominence, the tuber ischiadicum (also ischial tuber), commonly called the pin bone in cattle. The pubis, the smallest of the three pelvic bones, forms the cranial part of the floor of the pelvic cavity. The pubis also enters into the formation of the acetabulum and meets the pubis of the opposite side at the symphysis. The femur (thigh bone) extends from the coxofemoral (hip) joint to the stifle (the joint corresponding to the human knee). The proximal end of the femur has a nearly spherical head that articulates with the acetabulum of the os coxae to form the hip joint. There are also several roughened prominences, the trochanters, for the attachment of heavy thigh and hip muscles. The shaft of the femur is nearly circular on cross-section and has considerable length. The distal end has two condyles for articulation with the tibia and a trochlea for articulation with the patella, a sesamoid bone embedded in the tendon of insertion of the large quadriceps muscle. The tibia and fibula are the bones of the true leg (crus), the portion of the pelvic limb between stifle and hock. The tibia, the larger of the two, A A B B C C D D E E F F G G B C D E H F G I H I I Ox Pig A H Horse Figure 4-10. A, Pelvis; B, coxofemoral (hip) joint; C, femur; D, patella; E, stifle (knee) joint; F, crus (tibia & fibula); G, tarsus (hock); H, metatarsus; I, digit (phalanges). The distal end of the tibia has two concave depressions that form the hinge joint of the hock with the talus (tibiotarsal bone). In the dog, pig, and humans, the fibula is a long, thin bone extending from the proximal end of the tibia to the lateral aspect of the hock. The horse has both the proximal end and a portion of the shaft, whereas only a vestige of the proximal end of the fibula is present in domestic ruminants. All domestic species have the distal extremity of the fibula, forming the prominent lateral malleolus of the hock. The lateral malleolus is fused to the tibia in the horse but is a separate small bone articulating with distal tibia and tarsal bones in ruminants. The tarsus (hock), like the carpus in the thoracic limb is composed of multiple small bones; it corresponds to the human ankle. The calcaneus, which corresponds to the human heel, acts as a lever for the muscles extending the hock. In the horse, the central row of tarsal bones is reduced to a single central tarsal bone. The bones of the distal row are numbered 1 to 4 from medial to lateral, with tarsal bones 1 and 2 fused into a single bone. The metatarsus and digits of the pelvic limb are similar to the metacarpus and digits of the thoracic limb.
The interface between epidermal pegs and dermal papillae provides increased surface area for formation of a strong junction between these two layers. A blister is a local disruption of this association between layers, usually due to repeated trauma or thermal injury. Arteries, veins, capillaries, and lymphatics of the skin are contained in the dermis. Sensory nerve fibers, in addition to supplying the dermis, may extend a short distance into the epidermis. Sympathetic nerves provide motor innervation to blood vessels, glands, and arrector pili muscles of hair follicles in the dermis. These cells in the stratum basale produce the pigment, melanin, which is brown, yellowish-brown, or black. Packets of melanin pigment are manufactured by the melanocytes and transferred to surrounding cells of the epidermis; the same process incorporates pigment into cells that cornify into hairs. The expression of different colors in skin and hair comes primarily from the relative amount of melanin produced in the melanocytes rather than from differences in numbers of melanocytes or presence of other pigments. Absence of pigment in the skin (albinism), which may be partial or total, arises from a genetic inability of melanocytes to manufacture pigment. Lack of pigment can render the skin and surface mucous membranes more susceptible to actinic damage. Cancer eye, or squamous cell carcinoma of the conjunctiva of the eye, is common in white-faced cattle. There are three main types of hair on domestic mammals: (1) guard hairs, which form the smooth outer coat; (2) wool hairs, also called the undercoat, which are fine and often curly; and (3) tactile hairs, long stiff hairs with specialized innervation that renders them effective as organs of touch. An individual hair arises from a modification of the epidermis, the hair follicle. The follicle invaginates from the surface of the skin as a double-layered root sheath that surrounds the hair and terminates in a hair bulb of epidermal origin. The internal epithelial root sheath intimately covers the root of the hair and is continuous with the epithelial cells covering the dermal papilla. The external epithelial root sheath surrounds the internal root sheath, is continuous with the epidermis, and gives rise to the sebaceous glands that are associated with hair follicles. The division of the epithelial cells covering the dermal papilla generates the hair itself. Growth and multiplication of these cells extrude the hair from the follicle, causing it to grow. An individual hair has a medulla at its center, surrounded by a scaly cortex, outside of which is a thin cuticle. The bulk of the hair comprises the cortex, which consists of several layers of cornified cells. The amount and type of melanin in cortical cells determine whether the hair will be black, brown, or red. The cuticle is a single layer of thin, clear cells covering the surface of the cortex. The medulla may contain pigment, which has little effect on hair color, but air spaces between medullary cells are believed to Hypodermis In nearly all areas of the body, a layer of loose connective tissue separates the dermis from underlying structures. This areolar connective tissue, known variously as the superficial fascia, subcutis, or hypodermis, permits movement of the skin without tearing. Where the skin is tightly attached to underlying bone or muscle, a dimple on the body surface may be seen. This is a "tie," as is seen where the dermis is attached to the spinous processes of vertebrae. Variable amounts of fat, the panniculus adiposus, are present in the hypodermis, with species-dependent distribution and relative abundance. Epidermal cells adjacent to the dermal papilla give rise to the keratin of the hair. Wool hairs lack a medulla or have only a very small one, accounting for their fine, flexible nature. Tactile hairs, used as probes or feelers, are also called sinus hairs because a large bloodfilled sinus surrounds the deep portions of the follicle. These hairs are thicker and usually longer than guard hairs and are most commonly found on the face, around lips and eyes.
As in the second trimester, hyperechogenic kidneys can be a transient finding, but may also be a marker for renal abnormalities. Detailed sonographic evaluation of the fetus and follow-up examinations are recommended when hyperechogenic kidneys are noted in the first trimester of pregnancy. Increased echogenicity of fetal kidneys in the first trimester can be a sign of associated renal dysplasia, aneuploidy, or cystic renal disease. A and B: Hyperechogenic kidneys (arrows) in the first trimester in association with posterior urethral valves. C and D: Hyperechogenic kidneys (arrows) in the first trimester in association with trisomy 13. Facial dysmorphism, cardiac anomaly, and other abnormalities were also seen on ultrasound (not shown). Note in B, the presence of hyperechogenic kidneys, a common finding in trisomy 13. Note the presence of bilaterally enlarged polycystic kidneys, seen transabdominally in A and C and transvaginally in B. D: An axial plane of the lower pelvis in color Doppler shows the two umbilical arteries with no bladder seen in between. Amniotic fluid is still normal at this gestation and typically disappears around 16 weeks. This pregnancy was the result of consanguineous couple with recurrence risk of 25%. Note in A the presence of an occipital encephalocele and in B the presence of bilateral polycystic kidneys (arrows). B: A coronal plane of the abdomen in the next pregnancy at 12 weeks of gestation, showing normal size kidneys (one shown-arrow) with mild hyperechogenicity: within the echogenicity range of normal kidneys in early gestation (compare with. Ultrasound Findings Ideally, the kidneys should be visualized in a sagittal or coronal view in order to demonstrate large segments of renal parenchyma and enable a comparison with the surrounding lung, liver, and bowel. Enlarged hyperechogenic kidneys in the first trimester are particularly concerning because of the possibility of polycystic kidney disease or the association with aneuploidies. Out of the ciliopathies group is MeckelGruber syndrome, with the triad of polycystic kidneys, encephalocele, and polydactyly. When normal or mildly hyperechogenic kidneys are noted in the first trimester in at-risk families, follow-up ultrasound examinations into the second and third trimester is important because progression of ultrasound findings tend to occur after mid-gestation. The presence of enlarged hyperechogenic kidneys can occasionally be seen in early gestation, typically in the presence of a family history. The presence in the first trimester of an absent bladder on repeated examinations is also possible, given the lack of renal function. Bilateral Renal Agenesis Definition Bilateral renal agenesis is defined by the congenital absence of both kidneys and ureters, and results from a developmental failure of the ureteric bud and/or the metanephric mesenchyme. Bilateral renal agenesis has a prevalence of 1:4,000 to 1:7,000 pregnancies at the routine obstetric ultrasound examination. Anhydramnios leads to Potter sequence, which is a constellation of findings including pulmonary hypoplasia, facial abnormalities, and deformities of extremities. Bilateral renal agenesis is more common in males and is a uniformly lethal malformation. Ultrasound Findings the prenatal diagnosis of bilateral renal agenesis is a straightforward diagnosis after 16 weeks, because of associated oligohydramnios, as a leading ultrasound clue. The onset of oligo- or anhydramnios starts between 15 and 16 weeks of gestation when amniotic fluid production is primarily renal in origin. Therefore, the suspicion of bilateral renal agenesis in the first trimester is a challenge and primarily relies on the identification of an absent bladder and kidneys. Absent bladder in the pelvis on repeated ultrasound examinations may alert the examiner to the presence of bilateral renal agenesis in the first trimester. On rare occasions, a small "bladder" maybe visible in the pelvis in early gestation despite the presence of bilateral renal agenesis. Although the exact etiology of this finding is currently unclear, possibilities include retrograde filling of the bladder or the presence of a midline urachal cyst mimicking the bladder. The "lying down" or "flat" adrenal sign, an important second trimester sign showing the flattened adrenal gland on the psoas muscle, is not easily seen in the first trimester. When bilateral renal agenesis is suspected in the first trimester, follow-up ultrasound in the early second trimester is recommended to confirm the diagnosis by the onset of anhydramnios.
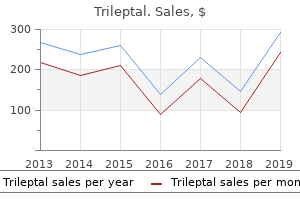
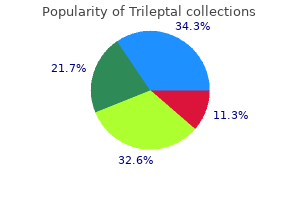
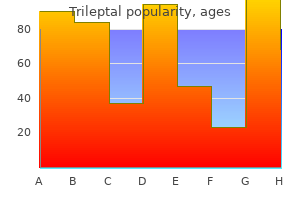
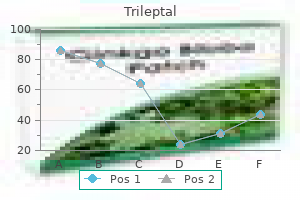
Romarin Sauvage (Marsh Tea). Trileptal.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96156
Members who use these products and services as a result of these gifts, rather than simply for the betterment of their patients and the improvement of the care rendered in their practices, shall be considered to have acted in an unethical manner. A physician shall not intentionally misrepresent himself/herself or his/her research work in any way. When participating in research, a physician shall follow the current laws, regulations and standards of the United States or, if the research is conducted outside the United States, the laws, regulations and standards applicable to research in the nation where the research is conducted. This standard shall apply for physician involvement in research at any level and degree of responsibility, including, but not limited to , research, design, funding, participation either as examining and/or treating provider, supervision of other staff in their research, analysis of data and publication of results in any form for any purpose. P a g e 46 Clinical Education Faculty Development Curriculum Overview Mentorship is one of the most important roles medical professionals can serve. While students do learn from classroom experiences and written resources, nothing can substitute for the opportunity to train under the supervision of an experienced clinician in a patient care setting. Sir William Osler, the renowned Canadian physician, once said, "To study the phenomenon of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all. Reasonable Expectations From Early Third Year Medical Students Students just starting the third year are prepared but insecure. They have been instructed on the clinical basics: formal presentations, H&P format, P. They are new to the clinical environment and clinical language (abbreviations etc. The student should be given a copy of their assessment, and a copy also needs to be sent to the Clinical Education Department via fax, email, online form, or regular mail. Each of the 7 core clinical competencies is evaluated on the performance assessment form and has been applied to the Clinical Education course objectives. Each competency section should be addressed and an overall recommendation for pass or fail for the rotation should be indicated. Faculty should add narrative comment to give the most specific guidance possible to the student. P a g e 47 It is important to note that students are evaluated against the standard of what should be reasonably expected from a medical student at the same point in training. The clinical clerkship program provides students with education and training in the areas of family medicine, internal medicine, obstetrics & gynecology, pediatrics, psychiatry, and surgery; as well as exposure to additional specialty areas such as critical care, anesthesiology, emergency medicine, geriatrics, pathology, and radiology. Rotations take place at a variety of clinical sites ranging from private, public and university-based hospitals to private and community-based clinics. In order to give students the opportunity to pursue individual interests, and to make decisions about options for residency training, flexibility is provided in both the third and fourth year schedules. Students are expected to follow the didactic complementary materials while serving in patient care rotations. In addition, students who embrace this primary care focused training will have an excellent foundation for specialty training, if that is what they choose. At Touro University College of Osteopathic Medicine, therefore, we focus our training on primary care, while recognizing that some students will choose other specialties. As such, our goals and objectives are designed to guide students to learn, through competency-based clinical education, the myriad dimensions of primary care. This includes recognition of their role as team leaders in providing comprehensive health care to the individual, to the family, and to the community. Throughout their training, students will develop an understanding of the role of the primary care physician while recognizing the need for consultation with other medical specialists when appropriate. Deepen their understanding of Osteopathic Principles and their application to enriching the health of their patients 3. Foster analytic and problem-solving skills necessary for physicians involved in disease prevention, diagnosis, and treatment of individual patients, families, and communities. Demonstrate the ability to integrate behavioral, emotional, social and environmental factors of families in promoting health and managing disease. Cultivate compassionate, ethical, and respectful, physician-patient relationships. Appreciate the differences in patient and physician backgrounds, ethnicity, beliefs and expectations. Critically evaluate current and relevant research and apply the results to medical practice.
An enlarged node may indicate infected or cancerous tissue in the region of the body draining to the node and necessitate condemnation of all or part of the carcass. Hemal nodes are small dark red or black nodes in cattle and sheep, usually in the dorsal parts of abdominal and thoracic cavities. Selected Lymph Nodes (Lymphocenters) of Cattle Name of Node Mandibular Parotid Retropharyngeal Deep cervical Superficial cervical (formerly prescapular) Axillary Mediastinal Intercostal Sternal Bronchial Lumbar Iliosacral Celiac Cranial mesenteric Subiliac (formerly prefemoral) Superficial inguinal (scrotal or mammary) Ischiatic Popliteal Location Intermandibular space Rostroventral to external meatus of ear Dorsal to pharynx Dorsolateral to trachea, divided into cranial, middle, & caudal groups Cranial to shoulder joint On medial aspect of shoulder near brachial plexus Within the mediastinum, divided into cranial, middle, and caudal groups Between ribs near thoracic vertebrae Deep surface of sternum Associated with major bronchi Group of nodes around aorta at level of last thoracic and first few lumbar vertebrae Group of nodes around terminus of abdominal aorta Group of nodes around origin of celiac a. Cranial to thigh in flank region Bulls, cranial to external inguinal ring; cows, dorsocaudal part of udder Group of nodes lateral to sacrotuberous ligament Caudal to stifle joint course of small blood vessels and have blood within their sinuses. It is attached to the stomach either directly by connective tissue, as in the ruminants, where it adheres closely to the rumen, or by the gastrosplenic ligament. Extensions of the capsule, trabeculae, penetrate into the interior of the organ, forming a connective tissue framework. The shape of the spleen varies considerably from one species to another, being long and thin in the pig, oblong in cattle, and sickle-shaped in the horse. The parenchyma (substance) of the spleen consists of red pulp and white pulp. The white pulp is lighter colored, as it is composed largely of lymphatic nodules, which are constructed much like the follicles of lymph nodes. The association of blood capillaries with the white pulp ensures that blood will be exposed to populations of immune cells. In addition to important immunologic functions, the spleen functions as a storage area for red blood cells, so the size of the spleen varies from time to time even within a given individual, as well as from species to species, depending on the number of red blood cells in the spleen at a given time. The spleen is also an important site where senescent (old and wornout) red blood cells are removed from the circulation, broken down, and their iron stored. These blood-related functions are associated with the red pulp of the splenic parenchyma. The spleen can be removed (splenectomy) without significant impairment to a mature animal. Tonsils In the most traditional sense, a tonsil is an unencapsulated aggregate of lymphatic nodules associated with the pharyngeal mucosa. These aggregates lack afferent lymphatic vessels, instead relying on their proximity to the epithelial surface to make contact with antigens. Many tonsils are characterized by deep invaginations on their epithelial surfaces called crypts, which presumably increase the surface area for contact with lymphatic tissue. Although the word tonsil is usually reserved for the lymphatic organs associated with the pharynx, identical histological elements are found in the mucous membranes of the prepuce and vagina and in the submucosa of the intestinal tract. Thymus the thymus is an organ of immature animals, undergoing involution at puberty, although never completely disappearing. It lies cranial to the heart, with portions extending along the trachea craniad into the ventral neck. The connective tissue components of the thymus form a loose areolar network that divides the organ into grossly visible lobules. Whether or not the blood is oxygenated, vessels that carry blood away from the heart are called arteries, and vessels that carry blood toward the heart are called veins. Circulation to the lungs (pulmonary circulation) is functionally and anatomically separate from circulation to the rest of the body (systemic circulation). Conceptually, it is therefore useful to regard the heart as two separate pumps housed within the same organ; one is a low-pressure pump that directs blood returning from the body to the lungs. The base is directed dorsad or craniodorsad and is attached to other thoracic structures by large arteries, veins, and the pericardial sac. The apex of the heart is directed ventrad and is entirely free within the pericardial sac. The surface of the heart is covered with visceral pericardium, which the pericardial space separates from the parietal pericardium. The parietal pericardium is attached by fibrous tissue to overlying pericardial pleura (not shown).
Presents with abdominal distension and diarrhea upon consumption of milk products; undigested lactose is osmotically active. Deficiency may be congenital (rare autosomal recessive disorder) or acquired (often develops in late childhood); temporary deficiency is seen after small bowel infection (lactase is highly susceptible to injury). Children classically present with abdominal distension, diarrhea, and failure to thrive. Due to IgA deposition at the tips of dermal papillae; resolves with gluten-free diet D. Duodenal biopsy reveals flattening of villi, hyperplasia of crypts, and increased intraepitheliallymphocytes. Small bowel carcinoma and T-celllymphoma are late complications that present as refractory disease despite good dietary control. Damage to small bowel villi due to an unknown organism resulting in malabsorption B. Damage is most prominent in jejunum and ileum (secondary vitamin B12 or folate deficiency may ensue); duodenum is less commonly involved. Metastasis of carcinoid tumor to the liver allows serotonin to bypass liver metabolism. Serotonin is released into the hepatic vein and leaks into systemic circulation via hepato -systemic shunts, resulting in carcinoid syndrome and carcinoid heart disease. Carcinoid syndrome is characterized by bronchospasm, diarrhea, and flushing of skin; symptoms can be triggered by alcohol or emotional stress, which stimulate serotonin release from the tumor. Carcinoid heart disease is characterized by right-sided valvular fibrosis (increased collagen) leading to tricuspid regurgitation and pulmonary valve stenosis; left-sided valvular lesions are not seen due to presence of monoamine oxidase (metabolizes serotonin) in the lung. Related to obstruction of the appendix by lymphoid hyperplasia (children) or a fecalith (adults) C. Periumbilical pain, fever, and nausea; pain eventually localizes to right lower quadrant (McBurney point). Rupture results in peritonitis that presents with guarding and rebound tenderness. Classically presents in young women (teens to 30s) as recurrent bouts of bloody diarrhea and abdominal pain l. More prevalent in the West, particularly in Caucasians and Eastern European Jews D. Due to congenital failure of ganglion cells (neural crest-derived) to descend into myenteric and submucosal plexus l. Myenteric (Auerbach) plexus is located between the inner circular and outer longitudinal muscle layers of the muscularis propria and regulates motility. Submucosal (Meissner) plexus is located in the submucosa and regulates blood flow, secretions, and absorption. Massive dilatation (megacolon) of bowel proximal to obstruction with risk for rupture D. Treatment involves resection of the involved bowel; ganglion cells are present in the bowel proximal to the diseased segment. Left lower quadrant pain (rectum) with bloody diarrhea Crypt abscesses with neutrophils. Right lower quadrant pain (ileum) with nonbloody diarrhea Lymphoid aggregates with granulomas (40% of cases) Cobblestone mucosa. Associated with constipation, straining, and low-fiber diet; commonly seen in older adults (risk increases with age) 2. Arise where the vasa recta traverse the muscularis propria (weak point in colonic wall); sigmoid colon is the most common location. Diverticulitis-due to obstructing fecal material; presents with appendicitis-like symptoms in the left lower quadrant 3. Presents with postprandial pain and weight loss; infarction results in pain and bloody diarrhea. Relapsing abdominal pain with bloating, flatulence, and change in bowel habits (diarrhea or constipation) that improves with defecation; classically seen in middleaged females B. Benign, but premalignant; may progress to adenocarcinoma via the adenoma-carcinoma sequence 3. Adenoma-carcinoma sequence describes the molecular progression from normal colonic mucosa to adenomatous polyp to carcinoma. Screening for polyps is performed by colonoscopy and testing for fecal occult blood; polyps are usually clinically silent, but can bleed.
In addition to these carpal extensors, the extensor muscles of the digits whose tendons pass over the dorsal surface of the carpus may act secondarily as extensors of the carpus. It takes origin from the medial epicondyle of the humerus and inserts on the palmar aspect of the proximal end of the metacarpus (medial side). These muscles are, of course, primarily flexors of the carpus, but they may act slightly in extension of the elbow. Its tendinous insertion is on the extensor process of the distal phalanx and on the proximal ends of the middle and proximal phalanges. The tendon is single in the horse; double in the cow, sheep, and goat; and split into four separate tendons in the pig and carnivores, in which species it inserts on the second through the fifth digits. It may also assist in extending the carpus and even in flexing the elbow (owing to its origin on the humerus). In ruminants, one of these heads gives rise to its own tendon that inserts on the third digit (the medial toe). The insertion varies according to the number of digits present, and there are interspecific differences regarding to which phalanx the tendon attaches. In pigs it inserts on the fourth and fifth digits; in ruminants, on the middle phalanx of the fourth digit; and in the horse, on the proximal phalanx of the third (and only) digit. In all animals the principal digital flexors are the superficial and the deep digital flexor muscles. Its long, stout tendon extends distad through the carpal canal, then along the palmar side of the metacarpus to insert on the palmar surface of the distal phalanges. As with the common digital extensor tendon, the number of insertions depends on the number of digits, with the main tendon dividing into individual slips, one per digit, just proximal to the fetlock. The deep digital flexor is the only muscle that flexes the distal interphalangeal joint. In the horse, the superficial digital flexor tendon inserts on the palmar aspects of the proximal end of the middle phalanx and the distal end of the proximal phalanx. The expression bowed tendons describes a traumatic condition of horses involving tendonitis of one or both of these tendons in the cannon region. Note swelling on the palmar aspect above the fetlock in the area of the flexor tendons. They take origin from the palmar aspect of the proximal metacarpus and insert on the proximal sesamoid bones. The suspensory ligaments are part of the passive support of the metacarpophalangeal joint. Muscles of the Pelvic Limb the hip is a ball-and-socket joint and as such can move in nearly any direction. Adduction and abduction are also fairly common movements, and some rotation is possible. Gastrocnemius Craniolateral aspect proximal tibia Extensor fossa of distolateral femur Tibial n. The chief extensors of the hip are the so-called hamstring muscles, which pass caudal to the hip from the tuber ischiadicum to the proximal end of the tibia, fibula, or calcaneus of the tarsus. The divisions between these muscles can be seen as vertical grooves in animals that are not very fat. In most other animals, the hamstring muscles originate almost exclusively from the tuber ischiadicum. It originates from the wing of the ilium and inserts on the greater trochanter of the femur, a lever projecting above the hip. Abductors of the hip extend laterally over the hip joint so as to move the limb away from the median plane. In addition to abducting the hip joint, this muscle flexes the hip joint and extends the stifle. They are all on the medial aspect of the thigh, extending from the pelvis to either the femur or the tibia. It extends from the ventral aspect of the pelvis to the medial side of the femur and tibia. Several other small muscles in this deep layer of hip musculature extending from the area of the obturator foramen are outward rotators of the thigh.
References:




