Figure 1 is a schematic picture of the somasensory area of the brain that depicts the importance and proportions of brain tissue devoted to the sense of touch. Other areas of the body, like the face or thigh are not able to read objects with the same accuracy or detail identification as the fingers. The amount of brain surface devoted to a body part is proportional to the sensitivity of that body part. Hands also perform fine and gross manipulative tasks such as turning a key, holding a glass, doing fine crafts, writing, using tools, and operating office equipment. Additionally, hands are used in a social role: the shaking, holding, and gesturing of this part of the body signals characteristics such as feelings, emotions, greetings, and enthusiasm. The hands serve a cosmetic function; we paint fingernails, wear rings, and put on decorative gloves. When working with shovels, hammers, or saws, the function of the hand is to grip and hold the equipment; the principal force and motion occurs at the wrist, forearm, elbow, and shoulder. During the assessment of impairment and rehabilitation potential, each of these multi-faceted functions and any associated limitations need assessment (Strickland & Graham, 2005). Practical Anatomy and Physiology of the Hand and Upper Extremity Terms and Hand Function Terms. Ventral (anterior) refers to the front or face side of the body; dorsal (posterior) is the term used when describing the back. Medial and lateral indicate closer to (medial) and farther away (lateral) from the midline of the body. When describing the hand, palmar (instead of ventral) and dorsal (instead of posterior) are the terms used. This begins in the cerebral cortex of the brain at the location of sensory and motor control where afferent nerve fibers conduct impulses to the brain and efferent fibers carry impulses from the brain to the rest of the body. Efferent fibers pass down the brain stem and exit through the nerve roots of the fourth to seventh cervical vertebrae (C4-C7) and from the first thoracic vertebrae (T1). On either side of the cervical spine, in the neck, these nerve roots combine to form the brachial plexus of nerves. From this plexus, three major nerves (the median, ulnar, and radial) reach the forearm and hand (Trumble & Allan, 2000; Weiss & Falkerstein, 2005). This nerve supplies sensation to the palm and palmar aspects of the thumb, index, long, and radial half of the ring finger. It is the most important sensory nerve to the hand and is the motor nerve for most of the muscles of the ventral forearm (forearm flexors), the muscles that bend and flex the wrist and flex or close the fingers and thumb. These median nerve controlled flexors provide power for gripping, lifting, and wrist flexion (Green, Hotchkiss, & Pederson, 2005). Below the wrist, the median nerve supplies motor and muscle innervation to the small, intrinsic muscles of the thumb (the thenar muscles) which aid in rowing the thumb out of the plane of the palm into opposition, and contribute to the power of pinch. Median nerve injuries are classified as either "high" or "low" (Strickland & Graham, 2005). A "high" median nerve injury results in an inability to flex the wrist, fingers, and thumb. This type of injury makes gripping of objects impossible and causes numbness of the thumb, index, center fingers, and half of the ring finger. Contrastingly, a "lower" median nerve injury causes numbness and weakness of the intrinsic muscles of the thumb, preventing actions relying on these muscles, such as pinching, turning a key, or in touching the tip of the thumb to the tip of the little finger. The ulnar nerve passes behind the medial epicondyle (the bony bump on the medial side of the elbow) an area called the cubital tunnel. In the hand, it provides sensation to the little finger, the ulna half of the ring finger, and muscle innervation and control to the small intrinsic muscles of the hand. Intrinsic muscles provide balance to the fingers and fine manipulative control of the hand. Injury to the ulnar nerve principally impairs dexterity and fine manipulation, including functions like pinch and manipulation of small objects, such as screws, coins, and buttons.
In Fanconi anemia, this is usually caused from ineffective blood production, abnormal iron absorption, or receiving a large number of blood transfusions, which boost iron levels. Heterozygous means that one of the copies of a gene is slightly different from the other copy of the gene. Hydronephrosis: Bilateral hydronephrosis is the enlargement (distention) of the pelvis and urine collecting structures of both kidneys which occurs when urine is unable to drain from the kidney down the ureters into the bladder. It is not itself a disease, but rather a physical result of whatever disease is keeping urine from draining out of the kidneys, ureters, and bladder. Fluids are given into a vein to provide most of the necessary nutrients the body needs. In girls, hypogonadism during childhood will result in lack of menstruation and breast development and short height. If hypogonadism occurs after puberty in females, symptoms include loss of menstruation, low libido, hot flashes, and loss of body hair. In boys, hypogonadism in childhood results in lack of muscle and beard development and growth problems. In men the usual complaints are sexual dysfunction, decreased beard and body hair, breast enlargement, and muscle loss. Hypopigmentation: Diminished pigmentation in a body part or tissue (such as the skin). Infants with hypospadias should not be circumcised; the foreskin should be preserved for use in later surgical repair. They attach to foreign substances, such as bacteria, and assist in destroying them. The classes of immunoglobulins are termed Immunoglobulin A (IgA), Immunoglobulin D (IgD), Immunoglobulin E (IgE), Immunoglobulin G (IgG), and Immunoglobulin M (IgM). Or, it may have openings to the urethra, bladder, base of penis or scrotum in boys, or vagina in girls. In girls, it is associated with malformations of the uterus and vagina which can affect sexual function and fertility. A condition of stenosis (narrowing) of the anus or absence of the anus may be present. The most common signs of the disorder are short neck, low hairline at the back of the head, and restricted mobility of the upper spine. It is also used in cancer randomized controlled trials as a measure of quality of life. In the male stimulates the development of interstitial tissue in the testis and the secretion of testosterone. One is Hodgkin lymphoma, which is marked by the presence of a type of cell called the Reed-Sternberg cell. The other category is non-Hodgkin lymphomas, which includes a large, diverse group of cancers of immune system cells; some of these cancers have a slow-growing course and some have a fast-growing course. Both Hodgkin and non-Hodgkin lymphomas can occur in children and adults, and prognosis and treatment depend on the stage and the type of cancer. Metacarpus: the part of the hand (metacarpal) or foot (metatarsal) between the carpus and the phalanges that contains five elongated bones when all the digits are present. Glossary 359 Nasojejunal tube: A soft feeding tube inserted through the nasal passages into the small bowel. Neuroblastoma: Cancer that arises in immature nerve cells and affects mostly infants and children. It resembles alcoholic liver disease, but occurs in people who drink little or no alcohol. Blood samples for fasting glucose and insulin are collected; then the patient drinks a standard amount of a glucose solution to challenge his 360 Fanconi Anemia: Guidelines for Diagnosis and Management or her system. This is followed by one or more additional glucose and insulin tests performed at specific intervals to track glucose and insulin levels over time. A peptic ulcer is erosion in the lining of the stomach or duodenum (the first part of the small intestine). Peritonitis: An inflammation (irritation) of the peritoneum, the tissue that lines the wall of the abdomen and covers the abdominal organs.
Besides mental retardation, it causes a progressive deterioration of nerve tissue and generally results in death at an early age. There are several physical factors other than genetic ones that influence the presence and severity of mental retardation. Fetal exposure to radiation during development can also cause genetic mutations that eventually result in mental retardation. Perinatal Causes During childbirth, several factors can increase the possibility of mental retardation (Ainsworth & Baker, 2004). Other factors include extreme prematurity, accidental physical trauma, asphyxia, hypoglycemia, infection, blood cell or blood type diseases, and Rh factor blood incompatibilities between mother and baby. Postnatal Causes Following birth, several other factors can increase the probability of mental retardation. These include malnutrition, acquired traumatic brain injury, meningitis, encephalitis, other infections, and chemical substances. Additional causes are demyelinating and degenerative disorders, consequences of seizure disorders, toxic-metabolic disorders, and environmental deprivation. Hyperthyroidism, whooping cough, chickenpox, measles, and Hip disease (a bacterial infection) may cause mental retardation if they are not treated adequately. Brain injury can be caused by a blow or a violent shake to the head and result in mental retardation in children. Normalization During the nineteenth and early part of the twentieth centuries, institutions for persons with mental retardation were created. In the last four decades, organized coalitions of parents and the "normalization" 344 Ton et al. In the 1950s, parents of children with mental retardation formed an organization called the National Association for Retarded Children (renamed the National Association for Retarded Citizens). They organized alternative programs and services for children with mental retardation. Until the 1970s, many public schools, along with state and local rehabilitation agencies, excluded individuals with mental retardation. The parents had to raise money independently for their children to receive community services. Services and Support the Principle of Normalization In 1959, the director of the Danish Mental Retardation Service, Bank-Mikkelsen, helped develop Danish law reflecting the principle of "normalization. The first systematic statement of normalization in world literature was published by Nirje (1969). As people with mental retardation move into the community and obtain employment and housing, a reconceptualization of service delivery models has evolved. Instead of social service agency personnel being responsible for supporting a person with mental retardation, the individual takes charge, utilizing support from family, friends, neighbors, and co-workers. Deinstitutionalization the normalization principle has been a strong driving force in establishing the deinstitutionalization movement. This movement involves integrating institutionalized persons with mental retardation into the community. Biklen and Knoll (1987) identified the major problems with institutions and other large congregate facilities, as well as the primary reasons for deinstitutionalizing people with mental retardation: · Institutions are the most expensive way of providing residential or any other services to people with mental retardation. Institutions do not provide opportunities for interaction with members of the community. Institutions do not allow for positive community living experiences or for development of skills needed for community life. Institutions perpetuate and enforce the image that people with mental retardation are oddities. People residing in institutions do not have opportunities to learn adaptive behavior from functioning non-insitutionalized people. Institutionalized people model their behavior after other people living in the institution; these behaviors are often maladaptive. Institutions provide a minimum of social and recreational activities and interaction; when they do, it is often demeaning and age inappropriate. Along with the above drawbacks, institutional living does not offer opportunities for vocational development. Typical jobs are not performed within an institutional environment, and opportunities to learn through observation are absent.
Lesions in healthy individuals are self-limited and may not necessitate treatment. Genital lesions have a potential carcinogenicity, neutropenia and potential permanent as well as nephrotoxicity. Ectoparasitic Infections Pediculosis Pubis Persons with pubic lice usually seek medical attention because of pruritus or because of lice or nits on pubic hair. Etiology: Pubic Lice Preferred Regimen: Permethrin 1% cream rinse applied to affected areas and washed off after 10 minutes B. Persons with scabies should be advised to keep fingernails closely trimmed to reduce injury from excessive scratching. Conventional Treatment Regimen: · Provided to patients who do not qualify for the Shorter Treatment · Treatment duration for 20-24 months. Pregnant patients taking Isoniazid should be given Pyridoxine (Vitamin B6) at 10-25 mg/d. Breastfeeding/Lactating women should be given Pyridoxine (Vitamin B6) at 10-25mg/d. Supplemental Pyridoxine should be given at 5-10 mg/d to the infant who is taking isoniazid or whose breastfeeding mother is taking isoniazid. The more advanced the liver disease, the fewer number of hepatotoxic drugs should be used. Comments: Please refer to the Table below on Dose Adjustments for Patients with Kidney Disease. Adults: Surgical prophylaxis is recommended only when the potential benefits exceed the risks and the anticipated costs. The antibiotic chosen must cover the expected pathogens for the operative site and take into account local resistance patterns. Intravenous antimicrobial must be started within 60 minutes before surgical incision. Exceptions: Vancomycin and fluoroquinolones require 1- to 2-hour infusion times; hence, dose is started 2 hours before surgical incision. Rapid infusion of vancomycin may result in hypotension and other signs and symptoms of histamine release (red man syndrome). A single dose of antimicrobial with a long enough half-life to achieve activity throughout the operation is sufficient for prophylaxis under most circumstances. For procedures lasting more than two half-lives of the prophylactic agent, or when there is excessive blood loss (>1,500 mL), intraoperative supplementary dose(s) may be required. It is also an alternative when patients have a history of an immediate type of allergic reaction to beta-lactams (anaphylaxis, laryngeal edema, bronchospasm, hypotension, local swelling, urticaria or pruritic rash occurring immediately after a beta-lactam dose) or exfoliative dermatitis. When gram-negative bacteria are a concern (as shown by local surveillance data), adding a second agent with appropriate in vitro activity may be necessary. In patients intolerant of or allergic to betalactams, use vancomycin with another gram-negative antibiotic. For patients currently given therapeutic antibiotic(s) for infection remote to surgery site and when the antibiotic regimen is appropriate also for prophylaxis, a dose should be given within an hour prior to incision. The risks of pre-surgical prophylaxis include Clostridium difficile infection and allergic reactions. Improper antimicrobial prophylaxis leads to excessive surgical wound infection rate (up to 52% in most studies), prolonged hospital stay, increased morbidity and mortality, and increased health care cost. Pediatric Patients: the principles mirror those for antibiotic prophylaxis in adults. However, data in the pediatric population are limited and recommendations have largely been extrapolated from studies in adults. Prophylaxis beyond 24 hours is not recommended No prophylaxis is needed for cardiac catheterization, carotid and brachiocephalic procedures without insertion of prosthetic grafts, and intravascular central line insertion (tunneled/untunneled). For prosthetic heart valves, it is recommended to stop prophylaxis either after removal of the retrosternal drainage catheters or just give a 2nd dose after coming off bypass. Ceftriaxone is recommended for centers where there is increasing resistance of Enterobacteriaceae to 1st and 2nd generation cephalosporins.
The pathogenesis of these conditions, which is varied and complex, is becoming better understood. The primary conductor for an orchestra of immunological instruments varies from disease to disease. The ability to tailor treatment to interfere with the major players will help us to reduce the burden of disability and reduce adverse effects. Treatments being made available for our use, often harvested from other specialties, are becoming useful in treating disease more specifically. Where rituximab fails, tyrosine kinase and proteasome inhibitors may be important in depleting the B-cell lineage. This lecture will briefly cover all of these concepts and emphasize the need for collaborative and well-designed trials to prove or disprove efficacy. Business, economies and, by extrapolation, medical activities largely cater to the upper sections of the pyramid. The circumstances at the bottom are unique; and the strategies employed in the apex seldom work for the base. Using illustrative cases, this lecture will present disruptive innovations to improve diagnosis and management of peripheral neuropathy at the base of the pyramid. The theatre is the principle opera house in Genoa and is located on the Piazza De Ferrari. Please make sure to wear your badge, as this will be your ticket into the theatre. We will start the evening with opening remarks and classical music performed by members of the local music conservatory in Genoa. Transportation will be on your own as this is walking distance from the Convention Centre. They also employ brain network analyses and lesion symptom mapping techniques in order to better understand cognitive impact of vascular brain injury. Sponsored by Akcea, this reception will feature guided exhibits, food, and beverages. He has pioneered the use of skin biopsy in peripheral neuropathies and neuropathic pain syndromes, contributed to the discovery of new phenotypes and gene mutations in small fibre neuropathies and participated in setting guidelines for clinical treatment of peripheral neuropathies. Cavalli and her colleagues have identified several key molecular players and their roles in announcing injury, initiating a response and carrying out repair. Cavalli studied the signaling mechanisms regulating membrane trafficking in cells. She continued with postdoctoral training at the University of California, San Diego. Larry Goldstein and studied how vesicular transport impacts signaling along peripheral nerves, and, vice versa, how signaling impacts vesicular transport. In her initial studies, she focused on retrograde injury signaling, or how information about an injury is conveyed from the distantly located lesion site in the axon back to the cell body. She received a post-doctoral fellowship from the Christopher and Dana Reeve Foundation to continue her studies on injury signaling. She then joined the Washington University faculty in 2006 and is now Associate Professor in the Department of Neuroscience. By characterizing informative patients and families affected by mitochondrial impairment, Prof Zeviani identified many disease-related genes and developed the first therapeutic approaches for mitochondrial diseases. His team has created several mouse models for the study of the molecular and cellular mechanisms of mitochondrial disorders, in addition to maintaining a clinical interest in the management and investigation of mitochondrial disease patients. His research has also provided a relevant contribution to the characterization of the role of mitochondrial dysfunction in the pathogenesis of several neurodegenerative conditions, involving the central and peripheral nervous systems. Scherer has sought to understand the causes and treatments of peripheral neuropathies, with a focus on inherited neuropathies in his clinical work and laboratory investigations. Gebhart Peripheral Nerve Society Prize for Excellence in Peripheral Nerve Research. Buses depart from the main entrance of the convention centre and will arrive at the villa every 30 minutes. We are a global healthcare company that produces essential plasma-derived medicines for patients and provides hospitals and healthcare professionals with the tools, information nd services they need to deliver expert medical care.
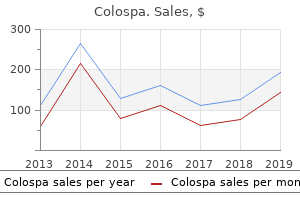
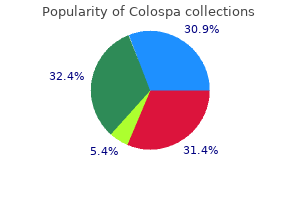
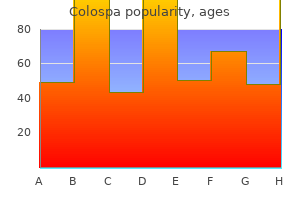
Mountain Hydrangea (Hydrangea). Colospa.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96653
Journal of veterinary internal medicine / American College of Veterinary Internal Medicine 12:349-354. The histologic classification of 602 cases of feline lymphoproliferative disease using the National Cancer Institute working formulation. Characterization of feline immunoglobulin heavy chain variable region genes for the molecular diagnosis of B-cell neoplasia. The relationship of serum cobalamin to methylmalonic acid concentrations and clinical variables in cats. It can be further classified according to its effect on the patient as mild or severe, nonfatal or fatal, and also by the presence of sequela such as abscess formation. Histologically, acute pancreatitis is characterized by findings that range from pancreatic edema to necrosis, variable infiltrates of mononuclear and polymorphonuclear cells, and local changes such as peripancreatic fat necrosis and thrombosis. Acute pancreatitis may resolve or persist and can be complicated by secondary infection and pseudocyst or abscess formation. It is tempting to equate mild acute pancreatitis with pancreatic edema, and severe or fatal pancreatitis with pancreatic necrosis, but this relationship has not been critically examined in patients with naturally occurring pancreatitis. Etiology and Pathogenenesis the etiology and pathogenesis of spontaneous pancreatitis is poorly understood. In the normal pancreas safeguards are present to ensure that harmful pancreatic enzymes are not activated until they reach the intestinal lumen. Vacuole formation is thought to be a consequence of the uncoupling of exocytosis of zymogens and abnormal intracellular trafficking of digestive and lysosomal enzymes. These subcellular alterations are considered to precipitate the intracellular activation of digestive enzymes. Pancreatic hyperstimulation may be of direct relevance to naturally occurring pancreatitis in dogs. It is possible that high fat diets exert their effects via the excessive release of cholecystokinin and that hypercalcemia, organophosphates and high levels of circulating glucocorticoids also facilitate (potentially by changing pancreatic sensitivity to hyperstimulation), or cause pancreatic hyperstimulation; however, this is not proven. This concept of pancreatic down regulation is important when considering nutritional intervention in acute pancreatitis. Often pancreatic inflammation is a self-limiting process, but in some animals reduced pancreatic blood flow and leukocyte and platelet migration into the inflamed pancreas may cause progression to pancreatic necrosis. It is the development of multisystemic abnormalities that separates mild from severe, potentially fatal pancreatitis. Diagnosis There is currently no single specific test for pancreatitis in dogs and diagnosis is based on a combination of compatible clinical, clinicopathological and imaging findings. Surgical biopsy may be required to confirm a diagnosis, and to distinguish inflammation from neoplasia. Clinical findings Signalment and History Midlle aged to old dogs (>5yrs years old) who are overweight appear at higher risk. Miniature Schnauzers, Yorkshire and Silky Terriers, non-sporting breeds and perhaps miniature poodles may be at increased risk of developing pancreatitis. Endocrinopathies such as hypothyroidism, diabetes mellitus and hyperadrenocorticism may also be risk factors. Thirteen percent of 221 dogs with diabetes mellitus had histological evidence of acute pancreatitis. The history may reveal a recent episode of dietary indiscretion, toxin ingestion or drug administration. Common clinical signs include lethargy, anorexia, hunched stance, vomiting (± blood), diarrhea (± blood), increased respiratory rate and enlarged abdomen. Polyuria and polydipsia may be present in dogs with diabetes mellitus and pancreatitis. Physical Examination Physical findings in dogs with acute pancreatitis are variable and range from depression, to mild dehydration with signs of abdominal pain, to acute abdominal crisis with shock (tachycardia, prolonged capillary refill time, tacky mucous membranes, hypothermia), petechiation, icterus and ascites. Diagnostic approach and differential diagnosis the differential diagnosis of acute pancreatitis in dogs is usually centered round the problems of vomiting and abdominal pain. In vomiting dogs the initial approach is to distinguish self-limiting from more severe causes of vomiting on the basis of physical findings and a minimum database. Packed cell volume, total protein, azostick, urinalysis, plasma concentrations of sodium and potassium). Where vomiting is associated with systemic signs of illness, or is persistent, the clinician has to differentiate metabolic, polysystemic infectious, toxic and neurologic causes from intra-abdominal causes. This is usually achieved on the basis of combined historical and clinical findings coupled with a minimum database and the evaluation of hematology and serum chemistry profile, urinalysis and abdominal radiography.
Therefore, the article motivates an agenda for future research that advocates the identification of key factors affecting building energy consumption, from the factors identified through the critical review. These key factors can be used to reduce building energy consumption when designing new buildings and making improvements to existing buildings and hence to alleviate energy poverty in Sri Lanka in future. Developing future hourly weather files for studying the impact of climate change on building energy performance in Hong Kong. Introduction to the special issue on parallel computing in climate and weather modelling. Weather effect on thermal and energy performance of an extensive tropical green roof. Weather data analysis and design implications for different climatic zones in China. Energy Consumption and Management in Public Buildings in China: An Investigation of Chongqing. Effects of shelterbelt trees on reducing heating-energy consumption of office buildings in Scotland. The impact of the projected changes in temperature on heating and cooling requirements in buildings in Dhaka, Bangladesh. Factors influencing energy efficiency investments in existing Swedish residential buildings. Use of model predictive control and weather forecasts for energy efficient building climate control. A computational method to assess the impact of urban climate on buildings using modelled climatic data. Feasibility of energy saving renovation measures in urban buildings the impact of energy prices and the acceptable pay back time criterion. Energy consumption, energy savings, and emission analysis in Malaysian office buildings. Future trends of building heating and cooling loads and energy consumption in different climates. A systematic procedure to study the influence of occupant behaviour on building energy consumption. Behavioural, physical and socio-economic factors in household cooling energy consumption. The optimum usage of labour, material and technology is thus, proposed to eliminate waste during the maintenance process. This paper proposes a maintainability approach to minimise maintenance waste in order to promote lean maintenance concept to the construction industry. The approach has widened the focus of existing lean maintenance concept by moving it boundaries from the maintenance phase to early phases of the development process. Eight challenges of lean maintenance have been established from fifty one maintainability causes of high-rise buildings. Their impact to maintenance cost was evaluated using a case study and found 40% reduction in the maintenance cost as wastage. Keywords: Lean Maintenance, Building Maintainability, Maintenance Cost, High-Rise Buildings. In the construction industry, the concept of maintainability of buildings focus on achieving efficient maintenance by eliminating waste in maintenance cost for rectifying maintenance deficiencies (De Silva, 2012). Thus, in turn this concept of maintainability promotes lean maintenance due to its similar focus on minimising waste. The causes for deficiencies in maintenance can be considered as maintainability risks (Low and Chong, 2004; Wong and Hui, 2005; Flores-Colen et al. These risks are not occurred only during the maintenance phase of a building (De Silva and Ranasinghe, 2010; De Silva, 2012). Poor accessibility for maintenance, inadequate design detailing, poor quality and incompatibility of materials, poor specifications, non availability of spare parts, lack of standard tools and instruments for regular maintenance were some of the highlighted design and construction related risks which incur many wastes in terms of financial losses in maintenance (Shabha, 2003; Chew and De Silva, 2003; Chew et al. In addition, lack of maintenance policies and strategies, budgets, skills, technology are identified as some such risks faced during the maintenance phase of buildings (Shabha, 2003).
Tumor response assessments were conducted every 9 weeks for the first 54 weeks and every 12 weeks thereafter. Thirty-five percent of patients had non-bladder urothelial carcinoma and 66% had visceral metastases. Twenty percent of patients had disease progression following prior platinum-containing neoadjuvant or adjuvant chemotherapy. Twenty-eight percent of patients had non-bladder urothelial carcinoma and 56% had visceral metastases. Thirty-one percent of patients had disease progression following prior platinum-containing neoadjuvant or adjuvant chemotherapy. Both cisplatin-eligible and cisplatin-ineligible patients are included in the study. The demographic information is limited to the 800 patients enrolled in Arms B and C where efficacy has been demonstrated. The majority of patients were White (82%), 13% of patients were Asian, 10% were Hispanic, and 2% of patients were Black. Clinical sites in Asia (enrolling 13% of the study population) received paclitaxel at a dose of 175 mg/m2 while the remaining 87% received paclitaxel at a dose of 200 mg/m2. Approximately 14% of patients had liver metastases at baseline, and most patients were current or previous smokers (80%). Tumor assessments were conducted every 6 weeks for the first 48 weeks, then every 9 weeks thereafter. The majority of patients were white (90%), 2% of patients were Asian, 5% were Hispanic, and 4% were Black. Patients with a history of autoimmune disease, symptomatic or corticosteroid-dependent brain metastases, or requiring systemic immunosuppression within 2 weeks prior to enrollment were ineligible. Tumor assessments were conducted every 6 weeks for the first 36 weeks and every 9 weeks thereafter. The trial excluded patients with a history of autoimmune disease, administration of a live attenuated vaccine within 4 weeks prior to randomization, administration of systemic immunostimulatory agents within 4 weeks or systemic immunosuppressive medications within 2 weeks prior to randomization; or untreated or corticosteroid-dependent brain metastases. Tumor assessments were performed every 8 weeks (± 1 week) for the first 12 months after Cycle 1, day 1 and every 12 weeks (± 1 week) thereafter. The demographic and baseline disease characteristics of the study population were well balanced between the treatment arms. Approximately half the patients had received a taxane (51%) or anthracycline (54%) in the (neo)adjuvant setting. Patients received treatment until radiographic disease progression or unacceptable toxicity. Tumor assessments were conducted every 6 weeks for the first 48 weeks following Cycle 1, Day 1 and then every 9 weeks thereafter. Patients treated beyond disease progression had tumor assessment conducted every 6 weeks until treatment discontinuation. The majority of patients were White (80%); 17% were Asian, 4% were Hispanic and 1% were Black. Patients were required to be evaluated for the presence of varices within 6 months prior to treatment, and were excluded if they had variceal bleeding within 6 months prior to treatment, untreated or incompletely treated varices with bleeding, or high risk of bleeding. Patients with Child-Pugh B or C cirrhosis, moderate or severe ascites; history of hepatic encephalopathy; a history of autoimmune disease; administration of a live, attenuated vaccine within 4 weeks prior to randomization; administration of systemic immunostimulatory agents within 4 weeks or systemic immunosuppressive medications within 2 weeks prior to randomization; or untreated or corticosteroid-dependent brain metastases were excluded. Tumor assessments were performed every 6 weeks for the first 54 weeks and every 9 weeks thereafter. The demographics and baseline disease characteristics of the study population were balanced between the treatment arms. The majority of patients were Asian (57%) or White (35%); 40% were from Asia (excluding Japan). Tumor assessments were performed every 8 weeks (± 1 week) for the first 24 months and every 12 weeks (± 1 week) thereafter. Based on central testing, 74% were identified as having a V600E mutation, 11% as having V600K mutation, and 1% as having V600D or V600R mutations. Store vials under refrigeration at 2°C to 8°C (36°F to 46°F) in original carton to protect from light.
References:




