The resistance to flow through the pulmonary artery decreases, while that of the systemic circulation increases. This results in a decrease in pressure in the right atrium, with an increase in the pressure within the left atrium. The resulting pressure changes in the two atria bring the septum primum and septum secundum into apposition and effectively close off the foramen ovale. At the same time, active contraction of the muscular wall of the ductus arteriosus as a result of the 90 the Heart Brachiocephalic A. Congenital abnormalities of the heart and great vessels the complex development of the heart and major arteries accounts for the multitude of congenital abnormalities that may affect these structures, either alone or in combination. Developmental Anatomy 91 Dextro-position of the heart means that this organ and its emerging vessels lie as a mirror-image to the normal anatomy; it may be associated with reversal of all the intra-abdominal organs (situs inversus). Septal defects include a patent foramen ovale (which occurs in some 10% of subjects) and atrial or ventricular septal defects. An ostium secundum defect lies high up in the atrial wall and is relatively easy to close surgically. An ostium primum defect lies immediately above the atrioventricular boundary and may be associated with a defect of the pars membranacea septi of the ventricular septum; it thus presents a more serious surgical problem. Occasionally, the ventricular septal defect is so huge that the ventricles form a single cavity, giving a trilocular heart. Congenital pulmonary stenosis may affect the trunk of the pulmonary artery, its valve or the infundibulum of the right ventricle. If stenosis occurs in conjunction with a septal defect, the compensatory hypertrophy of the right ventricle (developed to force blood through the pulmonary obstruction) produces a sufficiently high pressure to shunt blood through the defect into the left heart; this mixing of the deoxygenated right heart blood with the oxygenated left-sided blood results in the child being cyanosed at birth. This results from unequal division of the truncus arteriosus by the spiral septum, resulting in a stenosed pulmonary trunk and a 1 Pulmonary stenosis 2 Septal defect + 3 Overriding aorta 4 R. The displaced septum is unable to close the interventricular septum, which results in a ventricular septal defect. Right ventricular hypertrophy develops as a consequence of the pulmonary stenosis. Cyanosis results from the shunting of large amounts of desaturated blood from the right ventricle through the ventricular septal defect into the left ventricle and also directly into the aorta. If left uncorrected, it causes progressive hypertrophy of the left heart and pulmonary hypertension. There may Developmental Anatomy 93 be an extensive obstruction of the aorta from the left subclavian artery to the ductus, which is widely patent and maintains the circulation to the lower part of the body; often there are multiple other defects and frequently infants so afflicted die at an early age. More commonly, there is a short segment involved in the region of the ligamentum arteriosum or still-patent ductus. In these cases, circulation to the lower limb is maintained via collateral arteries around the scapula anastomosing with the intercostal arteries, and via the link up between the internal thoracic and inferior epigastric arteries. Clinically, this circulation may be manifest by enlarged vessels which may be palpable around the scapular margins; radiologically, hypertrophy of the engorged intercostal arteries results in notching of the inferior borders of the ribs. Abnormal development of the primitive aortic arches may result in the aortic arch being on the right, or actually being double. An abnormal right subclavian artery may arise from the dorsal aorta and pass behind the oesophagus aa rare cause of difficulty in swallowing (dysphagia lusoria). Rarely, the division of the truncus into aorta and pulmonary artery is incomplete, leaving an aortopulmonary window, the most unusual congenital fistula between the two sides of the heart. This page intentionally left blank Part 3 the Vertebral Canal and its Contents this page intentionally left blank the Vertebrae and Sacrum the bones of the vertebral canal are landmarks, identified both by the palpating fingers and the exploring needle, by which the anaesthetist performs spinal and epidural blocks. As well as being able to recognize these landmarks, it is essential to be familiar with the feel of the intervertebral ligaments as they yield to the advancing needle, and to have an intimate knowledge of the relationship of nervous tissue and the dural sheath to the bony structures. The adult spine presents four curvatures: those of the cervical and lumbar zones are convex forwards (lordosis), those of the thoracic and sacral regions are concave (kyphosis).
Ultimately, children who have undergone aortic valvotomy may require a prosthesis or homograft in adulthood if the valve becomes calcified or rigid, or sooner, if the valve develops important regurgitation. No currently available replacement valve is perfect: mechanical prostheses are long lived but thrombogenic, so anticoagulation is required; homograft valves, although free from thrombogenic complications, are often shorter lived because of destruction by calcification at an unpredictable rate. A homograft valve is placed in the pulmonary position, where performing balloon dilation or future surgical revision is less risky because of its more accessible anterior location and presence on the pulmonary side of the circulation. Summary In aortic valvar stenosis, a suprasternal notch thrill is present, associated with a systolic ejection murmur in the aortic area and with an aortic systolic ejection click. The electrocardiogram may show left ventricular hypertrophy and repolarization abnormalities. The echocardiogram is the most crucial laboratory examination for following the course of the patient. The echocardiographic estimate of the degree of obstruction or symptoms, such as chest pain or syncope, alerts the provider that further diagnostic studies and intervention are warranted. Relief of the obstruction by valvotomy or valvuloplasty can be done at low risk in children with moderate or severe stenosis. Discrete membranous subaortic stenosis this is the second most common form of left ventricular outflow obstruction but much less frequent than aortic valvar stenosis. This obstruction is a fibromuscular membrane with a small central orifice located in the left ventricle, usually within 1 cm of the aortic valve (Figure 5. Because the jet strikes the aortic valve, the energy 5 Conditions obstructing blood flow in children 169 of the jet is dissipated so that poststenotic dilation of the ascending aorta rarely occurs; however, problems with aortic valve regurgitation frequently result from alterations in the aortic valve. The symptoms of chest pain and syncope may occur in patients with severe obstruction, but most patients are asymptomatic. Physical examination the prominent physical finding is an aortic systolic ejection murmur heard best along the left sternal border, often lower than in patients with valvar aortic stenosis. Systolic ejection clicks rarely occur because the ascending aorta is usually normal in size. An aortic early diastolic murmur of aortic regurgitation is present in about 70% of the patients. Natural history Discrete membranous subaortic stenosis progresses, not usually because of increasing subaortic stenosis but because of aortic valvar regurgitation. The aortic regurgitation develops and progresses from trauma of the jet on the aortic valve. Echocardiogram A discrete subaortic ridge can usually be seen projecting from the septum into the left ventricular outflow tract. In contrast to valvar aortic stenosis, the disturbed color Doppler signals indicating turbulent flow begin at the site of the membrane, proximal to the valve itself. The maximum velocity of flow through the outflow tract is used to estimate the gradient. Some patients with a relatively unimportant gradient, less than 40 mmHg, have important aortic valvar regurgitation. A systolic pressure gradient is found below the level of the aortic valve within the left ventricle (Figure 5. Aortic regurgitation, if severe, causes a wide aortic pulse pressure and an elevated left ventricular end-diastolic pressure. Left ventriculography may identify the location of the membrane but is less helpful than echocardiography. Operative considerations Excision of the membrane is indicated in most patients, unless the gradient is small. Balloon dilation of subaortic membrane has been unsuccessful in reducing the gradient. The purposes of operation are relief of the elevated left ventricular systolic pressure and reduction of the aortic valve trauma. The operative risk, which is minimal, approaches that of operation for valvar aortic stenosis. The major hazard of the operation is damage to the septal leaflet of the mitral valve, since the membrane is often attached to this leaflet.
Syndromes
Thus, each lung has three lobes (like a right lung); the spleen, a left-sided structure, is absent; and the liver is symmetrical. Cardiac anomalies are complex, including atrial and ventricular septal defects, often in the form of atrioventricular septal defect, severe pulmonary stenosis or atresia, transposition of the great arteries, and, in about 75% of instances, total anomalous pulmonary venous connection. This combination of anomalies leads to clinical and roentgenographic features that resemble severe tetralogy of Fallot. Because of the symmetry of the liver, malrotation of the bowel, and midline position of the inferior vena cava, the important anatomic relationships that allow the definition of situs are disrupted, so classifying the type of cardiac malposition in patients with asplenia is difficult. Polysplenia syndrome (bilateral left-sidedness, left atrial isomerism, left atrial appendage isomerism) In this syndrome, as in asplenia, the heart may be located in either the left or right side of the chest. A tendency for symmetrical organ development also exists, in this case bilateral left-sidedness, in which both lungs appear as the left lung, the gallbladder may be absent, and there are multiple spleens. Cardiac anomalies include atrial and/or ventricular septal defect, partial anomalous pulmonary venous connection, and interrupted inferior vena cava with azygous continuation. As in asplenia, difficulty is encountered in determining situs because of the malrotation of the bowel and the fact that in about two-thirds of patients the inferior vena cava is interrupted at the level of the diaphragm. Radiographic 7 Unusual forms of congenital heart disease in children 241 barium swallow and echocardiography are the most useful noninvasive means of confirming the diagnosis. An understanding of the anatomic variations of vascular ring is gained by studying the development of the fourth and sixth aortic arches (Figure 7. Early in embryonic development, the ascending aorta gives rise to both a right and a left fourth aortic arch. These paired arches encircle the trachea and the esophagus and join to form the descending aorta. In addition, both a left and a right ductus arteriosus (sixth aortic arches) are found. In the normal development of the fourth arch, the right arch is interrupted beyond the right subclavian artery, and the right ductus arteriosus regresses. The proximal portion of the primitive right arch becomes the innominate artery, which in turn gives rise to the right carotid and right subclavian arteries. The left sixth arch persists as the left ductus arteriosus and connects the left pulmonary artery to the proximal descending aorta beyond the left subclavian artery. Right aortic arch If the left aortic arch is interrupted beyond the left subclavian artery, a right aortic arch with mirror-image branching is formed (Figure 7. The ascending aorta arises; the first branch is an innominate artery representing the proximal portion of the left aortic arch. The aortic arch passes towards the right and gives rise to the right carotid and right subclavian arteries. The aorta descends in the thorax and crosses into the abdomen to the left of the spine. Double aortic arch Rarely, neither aortic arch is interrupted during embryonic development. One of the aortic arches passes anteriorly to the trachea and the other passes posteriorly to the esophagus. They join to form the descending aorta that then courses in either the left or right side of the thorax. Thus, the trachea and esophagus are encircled by vascular structures and can be compressed, leading to respiratory symptoms and difficulty in swallowing. Aberrant subclavian artery If the right aortic arch is interrupted between the right carotid and right subclavian arteries instead of the usual location, the aortic arch is left-sided, but the right subclavian artery arises aberrantly. The remaining arch vessels are, respectively, the left carotid artery, the left subclavian artery, and finally, the right subclavian artery. The right subclavian artery arises from the descending aorta and passes behind the esophagus to the right arm. The opposite situation develops if the left aortic arch is interrupted between the left subclavian and left carotid arteries. The vascular ring is often completed by a ductus arteriosus, either ligamentous or patent, that passes from the aberrant subclavian artery to the ipsilateral pulmonary artery. These vascular rings formed by an aberrant subclavian artery can also cause symptoms that are usually relieved by dividing the ductus arteriosus, which is usually ligamentous.
The right phrenic nerve pierces the central tendon to the lateral side of the inferior vena cava (some fibres may actually accompany the vein through its foramen). The left nerve pierces the muscle about 1 cm lateral to the attachment of the pericardium. The diaphragm as a muscle of respiration the apex of the dome of the diaphragm reaches the level of the 5th rib in the mid-clavicular line, i. The 308 Zones of Anaesthetic Interest right hemidiaphragm is rather higher than the left, and both domes rise somewhat in the horizontal position. When the subject lies on his/her side, the upper cupola sinks to a lower level than its partner and its movements are relatively diminished. The level of the diaphragm is elevated in late pregnancy, gross ascites or obesity, in pneumoperitoneum and in patients with large abdominal tumours; such subjects all have some degree of respiratory limitation. In inspiration, the diaphragm moves vertically downwards (the domes considerably more than the central tendon) and this has a piston-like action in enlarging the thoracic cavity. A subsidiary effect is that the lower costal margin is raised and everted with consequent expansion of the base of the thorax. In expiration, the diaphragm relaxes; in forced expiration, it is actually pushed upwards by the increased intra-abdominal pressure effected by contraction of the muscles of the anterior abdominal wall. It is therefore interesting that bilateral phrenic interruption with complete diaphragmatic paralysis may cause little respiratory difficulty providing the lungs are relatively normal. In spite of extensive investigations, the exact nature of this sphincter is not understood. It is probably a complex affair made up of: 1 a physiological muscular sphincter at the lower end of the oesophagus; 2 a plug-like action of the mucosal folds at the cardia; 3 a valve-like effect of the obliquity of the oesophago-gastric angle; 4 a diaphragmatic sling which maintains the normal position of the cardia and has a pinch-cock action on the lower oesophagus; the Diaphragm 309 5 the positive intra-abdominal pressure which tends to squeeze the walls of the intra-abdominal portion of the oesophagus together. Reinforcing the sphincter are the mucosal folds of the cardia, which act as a plug wedged within the muscular ring. The crural sling of the diaphragm around the lower oesophagus is important in maintaining the normal position of the cardio-oesophageal junction below the diaphragm. There also appears to be a definite pinch-cock mechanism on the oesophagus when the diaphragm contracts in full inspiration; a phase at which intrathoracic pressure is lowest, intra-abdominal pressure highest and conditions most favourable for fluids to be forced at high pressure upwards through the cardiac orifice. The diaphragm is an important but not essential part of the cardiac sphincter mechanism, since a sliding hiatus hernia is not necessarily accompanied by regurgitation providing the physiological sphincter is competent. Similarly, free regurgitation occurs in some subjects with an apparently normal oesophageal hiatus, presumably because of some defect in the function of the physiological sphincter. The septum transversum is the mesoderm which, in early development, lies in front of the head end of the embryo. With the folding off of the head, this mesodermal mass is carried ventrally and caudally, to lie in its definitive position at the anterior part of the diaphragm. During this migration, the cervical myotomes and nerves contribute muscle and nerve supply, respectively, thus accounting for the long course of the phrenic nerve from the neck to the diaphragm. In spite of such a complex story, congenital abnormalities of the diaphragm are unusual. However, a number of defects may occur, giving rise to a variety of congenital herniae through the diaphragm. These may be: 310 Zones of Anaesthetic Interest Spinal cord Vertebra Rib Aorta Left pleuroperitoneal membrane Mesentery of oesophagus Right pleuro-peritoneal membrane Inferior vena cava Contribution from body wall Oesophagus Septum transversum. Far more common are the acquired hiatus herniae, divided into sliding and rolling hernia. These occur in patients usually of middle age, where weakening and widening of the oesophageal hiatus has occurred. In the sliding hernia, the upper stomach and lower oesophagus slide upwards into the chest through the lax hiatus when the patient lies down or bends over. In the rolling hernia (which is far less common) the cardia remains in its normal position and the cardio-oesophageal junction is intact, but the fundus of the stomach rolls up through the hiatus in front of the oesophagus, hence the alternative term of para-oesophageal hernia. The Intercostal Spaces the intercostal spaces are closed by thin but strong muscles and aponeuroses between which course the nerves, blood vessels and lymphatics of the chest wall. The intercostal muscles the muscles of the intercostal spaces are disposed in three layers corresponding to the three layers of the lateral abdominal wall. The external intercostals pass downwards and forwards from the lower border of one rib to the upper border of the rib below, and extend from the tubercle of the rib posteriorly to the neighbourhood of the costochondral junction in front. Anteriorly, each is continued as the tough anterior intercostal membrane to the side of the sternum.
Therefore, postganglionic fibres have only a short and direct course to their effector cells, and there is thus the anatomical pathway of a local discrete response to parasympathetic stimulation. The functions of this group of nerves can be summarized thus: 1 Pupilsaconstrictor to pupil, motor to ciliary muscle (accommodation); 2 Salivary glandsasecretomotor; 3 Lacrimal glandsasecretomotor; 4 Heartainhibitor of cardiac conduction, contraction, excitability and impulse formation (with consequent slowing of heart and decrease in force of contraction); 5 Lungsabronchoconstrictor, secretomotor to mucous glands (perhaps vasodilator to blood vessels); 230 the Autonomic Nervous System 6 Alimentary canalamotor to the gut muscles as far as the region of the splenic flexure; inhibitor to the pyloric sphincter. These ganglia also transmit (without synapse and therefore without functional connection) sympathetic and sensory fibres, which have similar peripheral distribution. It is responsible for all the functions of the cranial outflow of this system enumerated above apart from the innervation of the eye and the secretomotor supply to the salivary and lacrimal glands. The efferent fibres are derived from the dorsal nucleus of X, which lies in the central grey matter of the lower medulla, and are distributed widely in the cardiac, pulmonary and alimentary plexuses already described. Postganglionic fibres are relayed from tiny ganglia which lie in the walls of the viscera concerned; in the gut these constitute the submucosal plexus of Meissner and the myenteric plexus of Auerbach. The sacral outflow the anterior primary rami of S2 and 3, and occasionally S4, give off nerve fibres termed the pelvic splanchnic nerves or nervi erigentes, which join the sympathetic pelvic plexuses for distribution to the pelvic organs. It supplies visceromotor fibres to the muscles of the rectum (and perhaps the lower colon) and inhibitor fibres to the internal (involuntary) anal sphincter, motor fibres to the bladder wall and inhibitor fibres to the internal vesical sphincter. In addition, vasodilator fibres supply the erectile cavernous sinuses of the penis and clitoris. The Parasympathetic System 231 Afferent parasympathetic fibres Visceral afferent fibres from the heart, lung and the alimentary tract are conveyed in the vagus nerve, pass to the ganglion cells in the ganglion nodosum and thence pass to the dorsal nucleus of the vagus. Sacral afferents are conveyed in the pelvic splanchnic nerves S2, 3 and 4 and are responsible for visceral pain experienced in bladder, prostate, rectum and uterus. The reference of pain from these structures to the sacral area, buttocks and posterior aspect of the thighs is explained by the similar segmental supply to the sacral dermatomes. They merely use the autonomic nerves as a convenient anatomical conveyor system from the periphery to the brain. The remaining 10 pairs of nerves have a general plan of organization and it will simplify a complex subject if this is first considered. Here some embryology must be interposed; the primitive tubular hind-brain resembles the spinal cord in cross-section, in being divided into a dorsal (alar) lamina and a ventral (basal) lamina, separated by the sulcus limitans, which defines the boundary between the dorsal afferent and ventral efferent components. In the region of the future pons, the hind-brain becomes kinked (the pontine flexure), so that its roof becomes stretched and its cavity flattened to form the 4th ventricle. However, the alar and basal laminae can still be identified and maintain their functional integrity. It is comparable with the lateral grey column of the spinal cord and, like it, is concerned with visceral autonomic innervation. In the alar lamina, four cell groups that receive afferent fibres can be distinguished. It is the relay station for the two special receptor organs of the earathe cochlea and the vestibular apparatus. Introduction 237 Alar lamina Sulcus limitans Basal lamina A b Alar lamina Sulcus limitans Basal lamina f g e d c a B. The central processes of the olfactory receptors pass upwards from the olfactory mucosa in the upper part of the superior nasal concha and septum in (a) Mitral cell Receptor cell station Olfactory mucosa (b) Cell station in ganglion Receptor. The cell station of the olfactory nerve is the receptor cell in the olfactory mucous membrane; the cell station of the typical sensory cranial nerve lies in its ganglion. The mitral cells in turn send their axons back in the olfactory tract to terminate in the cortex of the uncus and the region of the anterior perforated space. The sense of smell is not highly developed in humans and is easily disturbed by conditions affecting the nasal mucosa generally. However, unilateral anosmia may be an important sign in the diagnosis of frontal lobe tumours. Tumours in the region of the uncus may give rise to the so-called uncinate type of fit, characterized by olfactory hallucinations associated with impairment of consciousness and involuntary chewing movements. Bilateral anosmia due to interruption of the 1st nerve is common after head injuries, particularly in association with anterior cranial fossa fractures. As the bundles of the olfactory nerve pierce the cribriform plate, they receive a sheath of the meninges which blends with the extracranial neurilemma; this constitutes an important pathway of infection from the nasal cavity to the subarachnoid space. It is not a true cranial nerve but should be thought of as a brain tract which has been drawn out from the cerebrum; embryologically it is developed, together with the retina, as a lateral diverticulum of the fore-brain. Devoid of neurilemmal sheaths, its fibres, like other brain tissues, are incapable of regeneration after division.
Vente M, Hobbelink M, van het Schip A et al (2007) Radionuclide liver cancer therapies: from concept to current clinical status. Bierman H, Byron R, Kelley K et al (1951) Studies on the blood supply of tumors in man. Gulec S, Fong Y (2007) Yttrium 90 microsphere selective internal radiation treatment of hepatic colorectal metastases. Murthy R, Kamat P, Nunez R et al (2008) Yttrium-90 microsphere radioembolotherapy of hepatic metastatic neuroendocrine carcinomas after hepatic arterial embolization. Sato K, Lewandowski R, Mulcahy M et al (2008) Unresectable chemorefractory liver metastases: radioembolization with 90Y microspheres-safety, efficacy, and survival. Andrews J, Walker S, Ackermann R et al (1994) Hepatic radioembolization with yttrium-90 containing glass microspheres: preliminary results and clinical follow-up. Hamza T, Van Houwelingen H, Stijnen T (2008) the binomial distribution of meta-analysis was preferred to model within-study variability. Gray B, Anderson J, Burton M et al (1992) Regression of liver metastases following treatment with yttrium-90 microspheres. Stubbs R, Cannan R, Mitchell A (2001) Selective internal radiation therapy with 90yttrium microspheres for extensive colorectal liver metastases. Murthy R, Xiong H, Nunez R et al (2005) Yttrium 90 resin microspheres for the treatment of unresectable colorectal hepatic metastases after failure of multiple chemotherapy regimens: preliminary results. Lim L, Gibbs P, Yip D et al (2005) Prospective study of treatment with selective internal radiation therapy spheres in patients with unresectable primary or secondary hepatic malignancies. Sharma R, Van Hazel G, Morgan B et al (2007) Radioembolization of liver metastases from colorectal cancer using yttrium-90 microspheres with concomitant systemic oxaliplatin, fluorouracil, and leucovorin chemotherapy. Anderson J, Goldberg J, Bessent R et al (1992) Glass yttrium-90 microspheres for patients with colorectal liver metastases. Geschwind J, Salem R, Carr B et al (2004) Yttrium-90 microspheres for the treatment of hepatocellular carcinoma. Lau W, Ho S, Leung T et al (1998) Selective internal radiation therapy for nonresectable hepatocellular carcinoma with intraarterial infusion of 90yttrium microspheres. Sangro B, Bilbao J, Boan J et al (2006) Radioembolization using 90Y-resin microspheres for patients with advanced hepatocellular carcinoma. Houle S, Yip T, Sheperd F et al (1989) Hepatocellular carcinoma: pilot trial of treatment with Y-90 microspheres. Dancey J, Shepherd F, Paul K et al (2000) Treatment of nonresectable hepatocellular carcinoma with intrahepatic 90Y-microspheres. Carr B (2004) Hepatic arterial 90yttrium glass microspheres (Therasphere) for unresectable hepatocellular carcinoma: interim safety and survival data on 65 patients. Liu M, Uaje M, Al Ghazi M et al (2004) Use of yttrium-90 TheraSphere for the treatment of unresectable hepatocellular carcinoma. Salem R, Lewandowski R, Atassi B et al (2005) Treatment of unresectable hepatocellular carcinoma with use of 90Y microspheres (TheraSphere): safety, tumor response, and survival. Sato K, Lewandowski R, Bui J et al (2006) Treatment of unresectable primary and metastatic liver cancer with yttrium-90 microspheres (TheraSphere): assessment of hepatic arterial embolization. Therasse P, Arbuck S, Eisenhauer E et al (2000) New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. Murthy R, Nunez R, Szklaruk J et al (2005) Yttrium-90 microsphere therapy for hepatic malignancy: devices, indications, technical considerations, and potential complications. Saar B, Kellner-Weldon F (2008) Radiological diagnosis of hepatocellular carcinoma. Salem R, Thurston K (2006) Radioembolization with 90yttrium microspheres: a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies part 2: special topics.
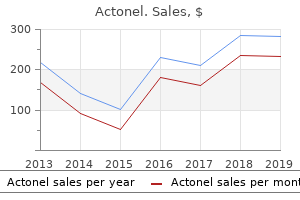
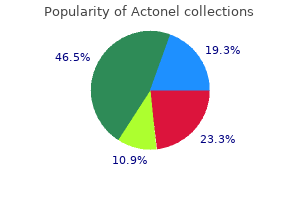
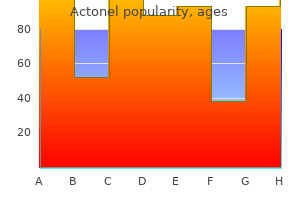
Reishi Antler Mushroom (Reishi Mushroom). Actonel.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96871
Objectives To identify whether the use of surgery or sclerotherapy should be recommended for the management of primary varicose veins. Search strategy Thirteen electronic bibliographic databases were searched covering biomedical, science, social science, health economic and grey literature (including current research). In addition, the reference lists of relevant articles were checked and various health services research-related resources were consulted via the internet. Selection criteria All studies that were described as randomised controlled trials comparing surgery with sclerotherapy for the treatment of primary varicose veins were identified. Data collection and analysis Two authors independently extracted and summarised data from the eligible studies using a data extraction sheet for consistency. Main results A total of 2306 references were found from our searches, 61 of which were identified as potential trials comparing surgery and sclerotherapy. However, only nine randomised trials, described in a total of 14 separate papers, fulfilled the inclusion criteria. Fifty trials were excluded and one trial is ongoing and is due for completion in 2004. The trials used a variety of outcome measures and classification systems which made direct comparison between trials difficult. However, the trend was for sclerotherapy to be evaluated as significantly better than surgery at one year; after one year (sclerotherapy resulted in worse outcomes) the benefits with sclerotherapy were less, and by three to five years surgery had better outcomes. There needs to be more research that specifically examines both costs and outcomes for surgery and sclerotherapy. Both involve removal of the vein either by stripping it out (surgery) or by injecting it with a solution that causes it to collapse and be absorbed into the surrounding tissues (sclerotherapy). This review found that sclerotherapy was better than surgery in terms of treatment success, complication rate and cost at one year, but surgery was better after five years. People can experience a wide range of symptoms associated with their varicose veins that may not be directly attributable to the veins themselves (Bradbury 1999). The extent of the visible veins does not correlate with the severity or number of symptoms experienced (Goldman 1994; Isaacs 1995). There also appears to be a complex interaction between cosmetic dislike and perception of symptoms (Robbins 1994). The literature divides the symptoms people experience into subjective and objective physical symptoms. Subjective symptoms can include heaviness, aching, itching and cosmetic appearance. Objective physical changes can include varicose eczema, pigmentation, bleeding, and varicose ulcers. The patient can experience, to a greater or lesser degree, all of these symptoms or none at all. Treatment of primary (simple) varicose veins is considered appropriate by the majority of vascular surgeons if the veins are symptomatic (Lees 1999). Common symptoms attributable to varicose veins include poor cosmesis (cosmetic appearance), ache and itching. Less common problems include haemorrhage (bleeding) and thrombophlebitis (inflammation of the vein wall with associated blood clot). There are currently three distinct treatment options available for varicose veins. Conservative treatment consists of lifestyle advice and the use of compression hosiery (graduated elasticated stockings). Many surgical treatments are practiced; these may involve ligation of the affected stem vein (long or short saphenous veins), stripping of the affected stem veins, and avulsions (tearing away) of the varicosities. Subfascial ligation is a procedure that involves cutting through the skin and deep fascia (a sheet of connective tissue) and ligating (tying off) the incompetent perforating veins that link the veins in the skin to the deep veins in the muscle.
Gestational age and cognitive ability in early childhood: a population-based cohort study. Variation in child cognitive ability by week of gestation among healthy term births. Long-term cognitive and health outcomes of school-aged children who were born late-term vs full-term. Dietary lipids are differentially associated with hippocampal-dependent relational memory in prepubescent children. The early development of brain white matter: a review of imaging studies in fetuses, newborns and infants. White matter integrity and cognitive performance in school-age children: a population-based neuroimaging study. Consistent anterior-posterior segregation of the insula during the first 2 years of life. Gestational age and neonatal brain microstructure in term born infants: a birth cohort study. Increased dorsolateral prefrontal cortex activation in obese children during observation of food stimuli. Tract-based spatial statistics: voxelwise analysis of multi-subject diffusion data. Threshold-free cluster enhancement: addressing problems of smoothing, threshold dependence and localisation in cluster inference. Development of the human fetal corpus callosum: a high-resolution, cross-sectional sonographic study. Grey and white matter distribution in very preterm adolescents mediates neurodevelopmental outcome. Decreased regional brain volume and cognitive impairment in preterm children at low risk. The current literature on basion-dens interval in children is sparse and based on bony measurements with variable values. Each of the 3 attending neuroradiologists and 2 residents reviewed images in 50 different patients (n 250), and each of the 2 other residents reviewed images in 25 different patients (n 50). The patients were divided Received May 25, 2017; accepted after revision August 3. From the Department of Radiology, University of Texas Health Science Center San Antonio, San Antonio, Texas. These measurements were obtained in sagittal reformatted images of the cervical spine in a soft-tissue window where cartilage can be easily seen around the dens (Fig 1).
The obvious physical degradation of the European races long settled in the United States, I do not ascribe to the intermingling of the European races on that con tinent, but to the influence of climate, which sooner or later disposes of all exotics; neither do I think that the amalgamation of all the races of men on the earth would lead to the extermination of manlrind,`I for each race would separate, and after the lapse of centuries revert to its original types The tribe of Griquas, on the Orange River, has been often cited as proof of the existence of a self supporting hybrid race. Now the Griquas whom I have seen seemed to me a bastard Hottentot race, in no way self-supporting. Hasty observations have greatly injured ethnology, as they have done science in general. I never had the smallest belief in such theories, which, indeed, I knew to rest on no scientific inquiry. But the distinguished French ethnologist thinks that it was not necessary to go to Poly nesia or to the desert banks of the Orange River in order to find a self-supporting hybrid race. He bids us look nearer home, and we shall find the race we inquire for in modern France and in other European countries. The two great nations raised by accident to be at the present moment arbiters of all human affairs, are supposed by those who support this view to be composed each of a hybrid race, distinct, self-supporting, and possessed of mixed moral and physical characters, distinct from those of the primitive race from which they spring. To me, on the contrary, it appears that modern Gaul, after having been overthrown by several races, has in the course of centuries depurated itself from all exotic elements. He admits that "the Belgians, Aquitains, and Celts differ from each other in their language, customs, and laws; but they are all Gauls, and have all a Gaulish look. The immortal Dictatm` speaks of " the levity of the Gauls, who are very changeable in their counsels and fond of novelties;" and, if I right-1y remember, speaks of their "religion as of a gloomy and ferocious character. The Dictator describes the Gauls as being extremely superstitious; the Germans, on the contrary, "acknowledge no gods but those that are objects of sight. There exists no hybrid race in Holland, the people being either Scandinavian or German; whilst the Kymri, a Gaulish race, have remained distinct from the Celt to the present day. They were pro bably the Kymrai, a Gaulish race, dispersed and broken up before his time. With this Belgian and Kymraig races the race or races we call Saxons largely intermingled. These so-called Saxons were in reality the Jutes, Angles, and old Saxons from North Germany, composed mostly of Germans or Teutons. This extremely plausible and even probable theory is therefore not supported by history. In the chapter on the Past, Present, and probable Future of Africa, I shall en deavour to show that the attempts made on a large scale in that continent to produce a hybrid race, have entirely failed; for the present, I shall confine myself to a few ob servations which no doubt have often occurred to others. Were the two races (the Teutonic and Celtiberian) so distinct as to render the formation of a hybrid race impossible The Gauls who invaded Asia Minor are said to have been a fair-haired race, and therefore were not pure Celts, but a mixed race, as the Kymri of Wales have dark hair. It is probable that with the Gaulish force there proceeded into Asia many Teuton or Germanic tribes; but be this as it may, it is generally admitted that all traces of these Europeans have disappeared from Asia Minor. Did the conquerors at Magenta and Solferino find any sympathy in the native population Did the victors at Marengo find in the aborigines the descendants of their Gaulish progenitors, even the remotest trace that the ground on which they stood had once been as essen tially Gaul in respect of its population as the banks of the Loire and the Seine The immortal Dictator does not say that they were of one race, but he ascribes to all " a Gaulish aspect. Both races migrate in great numbers to the United States of America, but they mingle not with the Anglo-Saxon nor with the Teuton; true to their nature, they await the advent of a leader-a sultan whom they will be sure to follow. The Teutonic Franks conquered France, and gave a name to the country; but this Teuton blood has alto gether disappeared.
The assessment of pulmonary venous connections is also possible but rather difficult in early gestation. The transvaginal approach to determining fetal situs may be challenging given the difficulty inherent in the transvaginal probe orientation. Associated extracardiac anomalies in heterotaxy are typically not detected in the first trimester and include various gastrointestinal anomalies and extrahepatic biliary atresia. Note the presence of an abnormal cardiac axis and an abnormal four-chamber view in A. Right ventricular hypertrophy, which represents the fourth anatomic feature of the "tetralogy," is typically not present prenatally. A and B: Axial planes of the chest at the four-chamber view in gray scale and color Doppler, respectively. In A and B, the four-chamber view appears normal with an axis deviation to the left (A) and with normal filling during diastole (B). Note in C overriding of the dilated aorta over the ventricular septal defect (star). Typically color Doppler demonstrates reverse flow in a tortuous ductus arteriosus and pulmonary artery in an oblique view of the chest, inferior to the aortic arch. Associated Malformations A right-sided aortic arch can be present in 20% to 50% of all cases. Associated extracardiac findings include a high incidence of chromosomal aberrations. The ductus arteriosus is absent in 50% of the cases, and when present it remains patent postnatally in about two-thirds of patients. This implies a normal connection between the atria and ventricles; the right atrium is connected to the right ventricle through the tricuspid valve and the left atrium is connected to the left ventricle through the mitral valve, but there is a switched connection of the great vessels, the pulmonary artery arising from the left ventricle, and the aorta arising from the right ventricle. Both great arteries display a parallel course, with the aorta anterior and to the right of the pulmonary artery. This oblique view of the fetal chest is not a standard plane of the obstetric ultrasound examination and thus is not displayed on routine ultrasound scanning. Also note that the aortic arch courses to the right of the trachea, as a right-sided aortic arch. The three-vessel-trachea view (A) demonstrates the presence of a single great artery of normal size, representing the superiorly located aorta (Ao). Associated Malformations Associated cardiac findings are common and include a full spectrum of cardiac lesions. Pulmonary stenosis is the most common associated malformation and occurs in about 70% of cases. A right aortic arch is associated with three main subgroups of arch abnormalities: right aortic arch with a right ductus arteriosus, right aortic arch with left ductus arteriosus, and double aortic arch. Right aortic arch can be part of a complex cardiac malformation, but can often also be an isolated finding. It is commonly suspected on transabdominal scanning when the relationship of the transverse aortic and ductal arches is evaluated. In recent years, we were able to diagnose right aortic arch with its three subgroups in the first trimester. Differentiating between the U-sign right aortic arch and the double aortic arch (lambda sign) may be difficult in the first trimester. When suspected in the first trimester of pregnancy, the identification of the actual subtype of right aortic arch can be confirmed on follow-up ultrasound examination in the second trimester of pregnancy. Associated Malformations Even if the right aortic arch appears as an isolated finding on ultrasound, fetal chromosomal karyotyping should be offered to rule out chromosomal aberrations, primarily 22q11 microdeletion12 and occasionally trisomy 21 and other aneuploidies. Associated intracardiac anomalies are more common when the aorta and ductus arteriosus are on the right (V-sign) than with double aortic arch or with the U-sign right aortic arch.
References:




