In the acute stages, the most important leukocyte is the neutrophil, which adheres to the blood vessel lining, squeezes between the endothelial cells and enters the tissues (see Fig. Phagocyte activity is promoted by the raised temperatures (local and systemic) associated with inflammation. After about 24 hours, macrophages become the predominant cell type at the inflamed site, and they persist in the tissues if the situation is not resolved, leading to chronic inflammation. They phagocytose dead/dying tissue, microbes and other antigenic material, and dead/dying neutrophils. Some microbes resist digestion and provide a possible source of future infection. Chemotaxis this is the chemical attraction of leukocytes, including neutrophils and macrophages, to an area of inflammation. It may be that chemoattractants act to retain passing leukocytes in the inflamed area, rather than actively attracting them from distant areas of the body. Known chemoattractants include microbial toxins, chemicals released from leukocytes, prostaglandins from damaged cells and complement proteins. Increased temperature the inflammatory response may be accompanied by a rise in body temperature (pyrexia), especially if there is significant infection. Body temperature rises when an endogenous pyrogen (interleukin 1) is released from macrophages and granulocytes in response to microbial toxins or immune complexes. Interleukin 1 is a chemical mediator that resets the temperature thermostat in the hypothalamus at a higher level, causing pyrexia and other symptoms that may also accompany inflammation. Pyrexia increases the metabolic rate of cells in the inflamed area and, consequently, there is an increased need for oxygen and nutrients. The increased temperature of inflamed tissues has the twin benefits of inhibiting the growth and division of microbes, whilst promoting the activity of phagocytes. Although pain is an unpleasant experience, it may indirectly promote healing, because it encourages protection of the damaged site. Suppuration (pus formation) Pus consists of dead phagocytes, dead cells, fibrin, inflammatory exudate and living and dead microbes. The most common pyogenic (pus-forming) bacteria are Staphylococcus aureus and Streptococcus pyogenes. Outcomes of acute inflammation Resolution this occurs when the cause has been successfully overcome. Damaged cells and residual fibrin are removed, being replaced with new healthy tissue, and repair is complete, with or without scar formation. Development of chronic inflammation Acute inflammation may become chronic if resolution is not complete. Chronic inflammation the processes involved are very similar to those of acute inflammation but, because the process is of longer duration, considerably more tissue is likely to be destroyed. The inflammatory cells are mainly lymphocytes instead of neutrophils, and fibroblasts are activated, leading to the laying down of collagen, and fibrosis. If the body defences are unable to clear the infection, they may try to wall it off instead, forming nodules called granulomas, within which are collections of defensive cells. Tuberculosis is an example of an infection that frequently becomes chronic, leading to granuloma formation. The causative bacterium, Mycobacterium tuberculosis, is resistant to body defences and so pockets of organisms are sealed up in granulomas within the lungs. Chronic inflammation may either be a complication of acute inflammation (see above) or follow chronic exposure to an irritant. Immunity Learning outcomes After studying this section, you should be able to: discuss the roles of the different types of T-lymphocyte in providing cell-mediated immunity describe the process of antibody-mediated immunity distinguish between artificially and naturally acquired immunity, giving examples of each distinguish between active and passive immunity, giving examples of each. Immunity possesses two key attributes not seen with non-specific defences: specificity and memory. Specificity Unlike mechanisms such as the inflammatory response and the phagocytic action of macrophages, which are triggered by a wide range of threats, an immune response is directed against one antigen and no others. Memory Again, unlike general defence mechanisms, an immune response against a particular antigen will usually generate immunological memory of that antigen. This means that the immune response on subsequent exposures to the same antigen is generally faster and more powerful. This long-lived white blood cell is manufactured in the bone marrow, and has a characteristically large, single nucleus.
Reports of vivax malaria marked by delirium, seizures, renal failure, shock, hepatic dysfunction, severe anemia, lung injury, pulmonary edema, and acute respiratory distress have come from South and Southeast Asia, the Middle East, and South America. The mature schizonts often contain golden-brown hemozoin pigment granules (malarial pigment). The overwhelming majority (>80%) of clinical cases of vivax malaria occur in South America and Southeast Asia. Laboratory Diagnosis Microscopic examination of thick and thin films of blood is the method of choice for confirming the clinical diagnosis of malaria and identifying the specific species responsible for disease. The thick film is a concentration method and may be used to detect the presence of organisms. Blood films can be taken at any time over the course of the infection, but the best time is midway between paroxysms of chills and fever, when the greatest number of intracellular organisms is present. Serologic procedures are available, but they are used primarily for epidemiologic surveys or for screening blood donors. Serologic findings usually remain positive for approximately a year, even after complete treatment of the infection. Treatment, Prevention, and Control the treatment regimen, including the use of primaquine to prevent relapse from latent liver forms, is similar to that used for P. Bed rest, relief of fever and headache, regulation of fluid balance, and in some cases blood transfusion are supportive therapies. Gametocidal: aimed at destroying erythrocytic gametocytes to prevent mosquito transmission Chloroquine is the drug of choice for suppression and therapeutic treatment of P. Primaquine is especially effective in preventing a relapse from the latent forms of P. Because antimalarial drugs are potentially toxic, it is imperative that physicians carefully review the recommended therapeutic regimens. Recrudescence does occur, and attacks may develop after apparent abatement of symptoms. The early symptoms are influenza like, with fever patterns of 72 hours (quartan or malarial malaria) in periodicity. As a consequence, the host cell becomes enlarged and distorted, usually in an oval form. Schьffner dots appear as pale pink granules, and the cell border is frequently fimbriated or ragged. Laboratory Diagnosis Observing the characteristic bar and band forms and the rosette schizont in thick and thin films of blood establishes the diagnosis of P. Treatment to prevent relapse caused by latent liver forms is not required because these forms do not develop with P. Babesiosis is a zoonosis infecting a variety of animals such as deer, cattle, and rodents; humans are accidental hosts. Physiology and Structure Human infection follows contact with an infected tick (Figure 74-5). The infectious pyriform bodies are introduced into the bloodstream and infect erythrocytes. The intraerythrocytic trophozoites multiply by binary fission, forming tetrads, and then lyse the erythrocyte, releasing the merozoites. Infected cells can also be ingested by feeding ticks, in which additional replication can take place. Infection in the tick population can also be maintained by transovarian transmission. Babesia divergens, which has been reported more frequently in Europe, causes severe, often fatal infections in people who have undergone splenectomies. Clinical Syndromes After an incubation period of 1 to 4 weeks, symptomatic patients experience general malaise, fever without periodicity, headache, chills, sweating, fatigue, and weakness. As the infection progresses with increased destruction of erythrocytes, hemolytic anemia develops and the patient may experience renal failure. Epidemiology More than 70 different species of Babesia are found in Africa, Asia, Europe, and North America, with B. Ixodes dammini is the tick vector responsible for transmitting babesiosis in this area, and the natural reservoir hosts are field mice, voles, and other small rodents. Serologic Laboratory Diagnosis Examination of blood smears is the diagnostic method of choice.
Diseases
The species of Schistosoma can be differentiated by their characteristic egg morphology (Figures 76-11 to 76-13). In all these areas, there are also reservoir hosts, specifically primates, marsupials, and rodents. Schistosomiasis may be considered a disease of economic progress; the development of massive land irrigation projects in desert and tropical areas has resulted in dispersion of infected humans and snails to previously uninvolved areas. Epidemiology the geographic distribution of the various species of Schistosoma depends on the availability of a suitable snail host. It has also become well established in the Western Hemisphere, particularly in Brazil, Suriname, Venezuela, parts of the West Clinical Syndromes Cercarial penetration of intact skin may be seen as dermatitis with allergic reactions, pruritus, and edema. Migrating worms in the lungs may produce cough; as they reach the liver, hepatitis may appear. The patient was admitted to the hospital because of the recent onset of paraplegia. He was in good health until 33 days before admission, when he noted the onset of progressive low back pain with radiation to the lower limbs. During this period, he was evaluated three times in another institution, where radiographic films of the lower thoracic, lumbar, and sacral spine were normal. Four weeks after the pain began, the disease progressed acutely with sexual impotence, fecal and urinary retention, and paraparesis progressing to paraplegia. At this time, the pain disappeared, replaced by a marked impairment of sensation in the lower limbs. On admission to the hospital, he gave a history of exposure to schistosomal infection. Neurologic examination revealed flaccid paraplegia, marked sensory loss, and absence of superficial and deep reflexes at and below the level T11. Myelography, computed tomographymyelography, and magnetic resonance imaging showed a slight widening of the conus. The diagnosis of neuroschistosomiasis was confirmed by the demonstration of viable and dead eggs of S. These eggs are similar in size to those of Schistosoma mansoni but can be differentiated by the presence of a terminal rather than lateral spine. Deposition of eggs in the bowel mucosa results in inflammation and thickening of the bowel wall, with associated abdominal pain, diarrhea, and blood in the stool. Eggs may be carried by the portal vein to the liver, where inflammation can lead to periportal fibrosis and eventually to portal hypertension and its associated manifestations. On gross examination, the liver is studded with white granulomas (pseudotubercles). Severe neurologic problems may follow when eggs are deposited in the spinal cord and brain (Clinical Case 76-4). Laboratory Diagnosis the diagnosis of schistosomiasis is usually established by demonstration of characteristic eggs in feces. Stool examination reveals the large golden eggs with a sharp lateral spine (see Figure 76-11). Using rectal biopsy, the clinician can see the egg tracks laid by the worms in rectal vessels. Quantitation of egg output in stool is useful in estimating the severity of infection and in following the response to therapy. Serologic tests are also available but are largely of epidemiologic interest only. Development of newer tests using stagespecific antigens may allow the distinction of active from inactive disease and thus have greater clinical application. Schistosomal dermatitis and Katayama syndrome may be treated with administration of antihistamines and corticosteroids. Education regarding the life cycles of these worms and molluscacide control of snails are essential. Unfortunately, treatment with praziquantel provides low cure rates in some areas, raising the specter of emerging resistance to this important therapeutic agent. The addition of artemether, an antimalarial, in combination with praziquantel has shown improved activity against S. In contrast to praziquantel, artemether acts against juvenile schistosomes in the host and may be used as a chemoprophylactic agent. Vaccine trials are in progress, but the ideal target antigen has not been identified.
Systemic disorders affecting neutrophil, monocyte/ macrophage, and lymphocyte function result in altered production or activity of host inflammatory mediators. Evidence has also shed light on the converse side of the relationship between systemic health and oral health, that is, the potential effects of periodontal disease on a wide range of organ systems. This field of periodontal medicine addresses the following important questions: · Can bacterial infection of the periodontium, commonly known as periodontitis, have an effect remote from the oral cavity? Although pathogenic bacteria are necessary for periodontal disease, they are not sufficient alone to cause the disease. In a host who is not susceptible to disease, pathogenic bacteria may have no clinical effect. Conversely, the susceptible host experiences clinical signs of periodontitis in the presence of pathogenic bacteria. Recognition of the importance of host susceptibility opens a door to understanding the differences in the onset, natural history, and progression of periodontitis seen throughout the scientific literature. Because of differences in host susceptibility, not all individuals are equally vulnerable to the destructive effects of periodontal pathogens. Thus patients may not necessarily have similar disease expression despite the presence of similar bacteria. Likewise, the response to periodontal treatment may vary depending on the wound-healing capacity and susceptibility of the host to further disease progression. The importance of host susceptibility is clearly evident in the medical literature. For example, respiratory tract pathogens may have minimal effect on many individuals, but in a susceptible host such as an elderly patient, these same pathogens may cause life-threatening respiratory tract illnesses. For example, patients with immune suppression may not be able to mount an effective host response to subgingival microorganisms, resulting in more rapid and severe periodontal destruction. Although the potential impact of many systemic disorders on the periodontium is well documented, recent evidence suggests that periodontal infection may significantly enhance the risk for certain systemic diseases or alter the natural course of systemic conditions. In 1900, William Hunter, a British physician, first developed the idea that oral microorganisms were responsible for a wide range of systemic conditions that were not easily recognized as being infectious in nature. In addition to caries, pulpal necrosis, and periapical abscesses, Hunter also identified gingivitis and periodontitis as foci of infection. He advocated extraction of teeth with these conditions to eliminate the source of sepsis. Hunter believed that teeth were liable to septic infection primarily because of their structure and their relationship to alveolar bone. He also believed that oral organisms had specific actions on different tissues and that these organisms acted by producing toxins, resulting in low-grade "subinfection," which produced systemic effects over prolonged periods. Finally, Hunter believed that the connection between oral sepsis and resulting systemic conditions could be shown by removal of the causative sepsis through tooth extraction and observation of the improvement in systemic health. The theory, while offering a possible explanation for perplexing systemic disorders, had been based on very little, if any, scientific evidence. Hunter and other advocates of the theory were unable to explain how focal oral sepsis produced these systemic maladies. They were also unable to elucidate possible interactive mechanisms between oral and systemic health. Furthermore, the suggested intervention of tooth extraction often had no effect on the systemic conditions for which patients sought relief. However, in order for the "hypothesis not to fall into disrepute for a second time, there must be no unsubstantiated attributions, no theories without evidence. To establish a relationship between conditions A and B, different levels of evidence must be examined. Even stronger evidence is provided by longitudinal studies, in which subject populations are examined over time. For example, a group of subjects might periodically have cholesterol levels evaluated over several years. Finally, intervention trials may be designed to alter the potentially causative condition and to determine the effect of this change on the resultant condition. For example, patients with elevated cholesterol may be divided into two groups: a group who uses a cholesterol-lowering drug or diet and a control group who has no intervention. These two groups might also be compared with a third group with normal cholesterol levels. At each level of evidence, it is important to determine whether a biologically plausible link exists between conditions A and B.
The Bibliography lists several excellent reviews for more complete information and discussions of available antiparasitic agents. Antiprotozoal Agents Similar to antibacterial and antifungal agents, antiprotozoal agents are generally targeted at relatively rapidly proliferating, young, growing cells. Most commonly, these agents target nucleic acid synthesis, protein synthesis, or specific metabolic pathways. HeavyMetals the heavy metals used for the treatment of parasitic infections include arsenical (melarsoprol) and antimonial compounds (sodium stibogluconate, meglumine antimonate). These agents are thought to oxidize sulfhydryl groups of enzymes that are essential catalysts in carbohydrate metabolism. Arsenicals also inhibit sn-glycerol-3-phosphate oxidase, which is needed for the regeneration of nicotinamide adenine dinucleotide in trypanosomes but is not found in mammalian cells. The antimonials, sodium stibogluconate and meglumine antimonate, inhibit the glycolytic enzyme phosphofructokinase and certain Krebs cycle enzymes in Leishmania organisms. They have also been shown to interfere with the metabolism of glutathione and trypanothione, resulting in an increased sensitivity of the organisms to oxidant stress. Toxicity is greatest on cells that are most metabolically active, such as neuronal, renal tubular, intestinal, and bone marrow stem cells. Their differential toxicity and therapeutic value are largely related to enhanced uptake by the parasite and its intense metabolic activity. Melarsoprol is the drug of choice for trypanosomiasis involving the central nervous system. It can penetrate the blood-brain barrier and is effective in all stages of trypanosomiasis. Meglumine antimonate and sodium stibogluconate are important agents for the treatment of leishmaniasis and are active against all forms of the disease. Prolonged therapy is usually required for disseminated leishmaniasis, and relapses are common. Despite the use of antimonials worldwide for treatment of leishmaniasis for over 6 decades with little evidence of resistance, acquired resistance has become a clinical threat within the past 10 years. This resistance is so far unique to Leishmania donovani, which causes visceral leishmaniasis in the hyperendemic region of Bihar, India. The mechanism of resistance is not completely understood but likely involves activation of an efflux pump in the plasma membrane of the organism with transport of the drug out of the cells. QuinolineDerivatives the quinoline derivatives include the 4-aminoquinolines (chloroquine), the cinchona alkaloids (quinine, quinidine), the 8-aminoquinolines (primaquine), and the synthetic quinoline compounds (mefloquine, halofantrine, lumefantrine). These compounds all have antimalarial activity and accumulate preferentially in parasitized red blood cells. Quinine, quinidine, the 4-aminoquinolines, and the synthetic quinolines rapidly destroy the erythrocytic stage of malaria and thus may be used prophylactically to suppress clinical illness or therapeutically to terminate an acute attack. Chloroquine remains the drug of choice for prophylaxis and treatment of susceptible malaria strains. Both quinine and quinidine are quite toxic and not rapidly parasiticidal; thus they should not be used alone but rather in combination with a sulfonamide or tetracycline antibiotic with antimalarial activity. Mefloquine is a 4-quinolinemethanol antimalarial agent used for prophylaxis and treatment of falciparum malaria. Unfortunately, mefloquine-resistant strains of falciparum malaria have been reported from Southeast Asia and Africa. Halofantrine is a synthetic phenanthrene-methanol compound with proven efficacy in the treatment of P. Halofantrine is more active than mefloquine; however, cross-resistance between these drugs occurs. It is considered a second-line agent for the treatment of malaria because of its expense and toxicity. Lumefantrine is also a phenanthrene-methanol compound that is available only as a fixed formulation combined with artemether. Recent studies from Cambodia have raised the possibility of declining efficacy to artemetherlumefantrine, with failure rates for the treatment of P. Protozoa are unable to absorb exogenous folate and thus are susceptible to drugs that inhibit folate synthesis. The folic acid antagonists that are useful in treating protozoan infections include diaminopyrimidines (pyrimethamine and trimethoprim) and sulfonamides.
The E2 glycoprotein is responsible for mediating viral attachment and membrane fusion and is the target of neutralizing antibodies. Pathogenesis and Clinical Syndromes Most human coronaviruses have an optimum temperature for viral growth of 33° C to 35° C, and therefore infection remains localized to the upper respiratory tract. Coronaviruses cause cytolytic infections and when inoculated into the respiratory tracts of human volunteers, they infect and disrupt the function of ciliated epithelial cells (Box 47-2). Most human coronaviruses cause an upper respiratory tract infection, accounting for approximately 10% to 15% of upper respiratory tract infections in humans. The disease is similar to the common cold caused by rhinoviruses but with a longer incubation period (average, 3 days). The infection may exacerbate a preexisting chronic Box 47-1 Unique Features of Coronaviruses Virus has medium-sized virions with a solar coronalike appearance. Coronavirus disease appears either sporadically or in outbreaks in the winter and spring. Antibodies to coronaviruses are uniformly present by adulthood, but reinfections are common, despite the preexisting serum antibodies. Coronavirus-like particles have also been seen in electron micrographs of stool specimens obtained from adults and children with diarrhea and gastroenteritis and in infants with neonatal necrotizing enterocolitis. The outbreaks of these viral diseases have occurred when the animal reservoir has come in contact with man. A combination of viral pathogenesis and immunopathogenesis causes significant lung, kidney, liver, and gastrointestinal tissue damage and depletion of immune cells. The virus apparently jumped to man from animals (masked-palm civets, raccoon dogs, and Chinese ferret badgers) raised for food. Travel restrictions and public concern resulted in a loss of hundreds of millions of dollars in travel and other business. Protein synthesis is divided into early and late phases, similar to that in the togaviruses. The genome associates with rough endoplasmic reticulum membranes modified by virion proteins and buds into the lumen of the rough endoplasmic reticulum. Vesicles that contain virus migrate to the cell membrane, and virus is released by exocytosis. The E2 glycoprotein interacts with receptors on epithelial cells, the virus fuses or is Box 47-2 Disease Mechanisms of Human Coronaviruses Virus infects epithelial cells of upper respiratory tract. Virus replicates best at 33° C to 35° C; therefore it prefers the upper respiratory tract. The glycoprotein "corona" helps this enveloped virus survive the gastrointestinal tract. Severe acute respiratory syndrome infection is exacerbated by inflammatory responses. Treatment, Prevention, and Control Control of respiratory transmission of the common cold form of coronavirus would be difficult and is probably unnecessary because of the mildness of the infection. The noroviruses are members of the Caliciviridae family, which also includes astroviruses and other small, round gastroenteritis viruses. Many of the other viruses in this family also bear the names of the geographic locations where they were identified (Box 47-3). Structure and Replication Noroviruses resemble and are approximately the same size as the picornaviruses. The genome is contained in a 27-nm naked capsid consisting of 60,000-Da capsid proteins. Norwalk virions are round with a ragged outline, whereas other calicivirion capsomeres have cup-shaped indentations or a sixpoint star shape. The virions of the astroviruses have a five- or six-point star shape on the surface but no indentations. Antibodies from seropositive people can also be used to distinguish these viruses. Most caliciviruses and astroviruses can be grown in cell culture, but the Norwalk viruses cannot. Expression of the structural protein genes of different Norwalk viruses in tissue culture cells produces Norwalk viruslike particles. These particles were used to show that Norwalk viruses bind to the carbohydrate of either the A, B, or O blood group antigen on the cell surface.
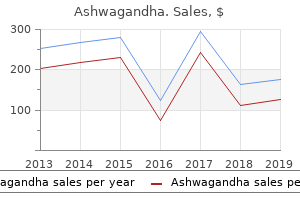
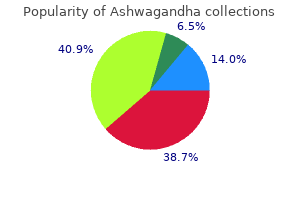
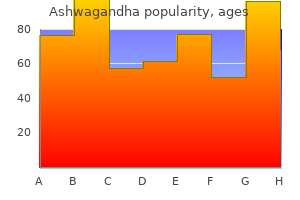
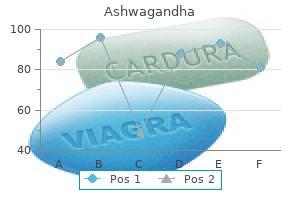
Asparagus Root (Asparagus Racemosus). Ashwagandha.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97111
These methods can be categorized primarily according to the pattern of motion when brushing and are primarily of historical interest, as follows:75 Roll: Roll method3 or modified Stillman technique 71 Vibratory: Stillman,124 Charters,24 and Bass12 techniques Circular: Fones technique47 Vertical: Leonard technique90 Horizontal: Scrub technique137 Controlled studies evaluating the effectiveness of the most common brushing techniques have demonstrated no clear superiority for any method. Patients with periodontal disease are most frequently taught a sulcular brushing technique using a vibratory motion to improve access in the gingival areas. The method most often recommended is the Bass technique because it emphasizes sulcular placement of bristles. The basic premise is to adapt the bristles tips to the gingival margin in order to reach the supragingival plaque, using controlled movement to avoid trauma and moving the brush systematically around all the teeth. Place the head of a soft brush parallel with the occlusal plane, with the brush head covering three to four teeth, beginning at the most distal tooth in the arch. Place the bristles at the gingival margin, pointing at a 45-degree angle to the long axis of the teeth. Exert gentle vibratory pressure, using short, back-and-forth motions without dislodging the tips of the bristles. This motion forces the bristle ends into the gingival sulcus area (Figure 50-4), as well as partly into the interproximal embrasures. The repetitive motion cleans the tooth surfaces, concentrating on the apical third of the clinical crowns, the gingival sulci, and as far onto the proximal surfaces as the bristles can reach. Lift the brush, move it to the adjacent teeth, and repeat the process for the next three or four teeth. After completing the maxillary arch, move the brush to the mandibular arch, and brush in the same organized way to reach all the teeth. If the brush is too large to reach the lingual surfaces of the anterior teeth, it should be turned vertically to press the end of the brush into the gingival sulcus area. Brush the occlusal surfaces of three or four teeth at a time by pressing the bristles firmly into the pits and fissures and brushing with several short, back-and-forth strokes. A, Place the toothbrush so that the bristles are angled approximately 45 degrees from the tooth surfaces. B, Start at the most distal tooth in the arch, and use a vibrating, backand-forth motion to brush. A, Proper position of the brush in the mouth aims the bristle tips toward the gingival margin. B, Diagram shows the ideal placement, which permits slight subgingival penetration of the bristle tips. Figure506 Positioning the powered toothbrush head and bristle tips so that they reach the gingival margin is critical to achieving the most effective cleaning results. The Bass technique requires patience and placement of the toothbrush in many different positions to cover the full dentition. Other methods of brushing, such as the modified Stillman71,124 and Charters,24 are variations of the Bass technique also designed to achieve thorough plaque removal at the gingival margins. They emphasize stimulation of the gingival circulation, which has not been demonstrated to achieve healing results beyond those achieved by good plaque removal. BrushingwithPoweredToothbrushes the various mechanical motions built into powered toothbrushes do not require special techniques. The patient need only concentrate on placing the brush head next to the teeth at the gingival margin and proceeding systematically around the dentition. A systematic method of brushing all the teeth, similar to the method described for manual brushing, should be used with powered toothbrushes (Figure 50-6). Recommendations · the principles of the Bass method have two advantages over other, more complex techniques: 1. Short, back-and-forth motion is easy to master because it is similar to the scrubbing that most patients normally perform. Cleaning action is focused on the cervical and interproximal portions of the teeth, where plaque accumulates first. This is true for all brushers, even periodontal patients with wide-open embrasures.
Interferons work by binding to cell surface receptors and initiating a cellular antiviral response. In addition, interferons stimulate the immune response and promote the immune clearance of viral infection. It has been approved for the treatment of condyloma acuminatum (genital warts, a presentation of papillomavirus) and hepatitis C (in combination therapy). Natural interferon causes the influenza-like symptoms observed during many viremic and respiratory tract infections, and the synthetic agent has similar side effects during treatment. Imiquimod, a Toll-like receptor ligand, stimulates innate responses to attack the virus infection. This therapeutic approach can activate local protective responses against papillomas, which generally escape immune control. Saquinavir, indinavir, ritonavir, nelfinavir, and other agents work by slipping into the hydrophobic active site of the enzyme to inhibit its action. Protease inhibitors (boceprevir, telaprevir, simeprevir) are also improving the outlook for treating patients with chronic hepatitis C. Educating all personnel regarding points 1, 2, and 3 and in the ways to decrease high-risk behaviors Methods for disinfection differ for each virus and depend on its structure. Most viruses are inactivated by 70% ethanol, 15% chlorine bleach, 2% glutaraldehyde, 4% formaldehyde, or autoclaving (as described in Guidelines for Prevention of Transmission of Human Immunodeficiency Virus and Hepatitis B Virus to Health-Care and Public-Safety Workers, issued in 1989 by the U. Most enveloped viruses do not require such rigorous treatment and are inactivated by soap and detergents. In addition to these procedures, special care must be taken with syringe needles and surgical tools · Antiinfluenza Drugs Amantadine and rimantadine are amphipathic amine compounds with clinical efficacy against the influenza A but not the influenza B virus (see Figure 40-3). Both compounds are acidotrophic and concentrate in and buffer the contents of the endosomal vesicles involved in the uptake of the influenza virus. This effect can inhibit the acidmediated change in conformation in the hemagglutinin protein that promotes fusion of the viral envelope with cell membranes. However, the specificity for influenza A is a result of its ability to bind to and block the proton channel formed by the M2 membrane protein of the influenza A virus. Amantadine and rimantadine may be useful in ameliorating an influenza A infection if either agent is taken within 48 hours of exposure. The principal toxic effect is on the central nervous system, with patients experiencing nervousness, irritability, and insomnia. Control of an outbreak usually requires identification of the source or reservoir of the virus, followed by cleanup, quarantine, immunization, or a combination of these measures. The first step in controlling an outbreak of gastroenteritis or hepatitis A is identification of the food, water, or possibly the day-care center that is the source of the outbreak. Education programs can promote compliance with immunization programs and help people change lifestyles associated with viral transmission. Such programs have had a significant impact in reducing the prevalence of vaccinepreventable diseases such as smallpox, polio, measles, mumps, and rubella. Bibliography Carter J, Saunders V: Virology: principles and applications, Chichester, England, 2007, Wiley. Collier L, Oxford J: Human virology, ed 3, Oxford, England, 2006, Oxford University Press. De Clercq E: A 40-year journey in search of selective antiviral chemotherapy, Ann Rev Pharmacol Toxicol 51:124, 2011. Websites New Medical Information and Health Information: Antiviral drugs: Antiviral agents, antiviral medications. Food and Drug Administration: Influenza (flu) antiviral drugs and related information. A patient has been exposed to influenza A virus and is in his fifth day of symptoms. To what therapeutic agents is the patient referring, and why did you decline to use the treatment? Steps in viral replication that depend on cellular processes are generally poor antiviral drug targets. Amantadine and rimantadine inhibit influenza A virus replication by preventing uncoating of the virus in the cytoplasm. Oseltamivir and zanamivir are neuraminidase inhibitors that inhibit both influenza A and B virus by preventing proper release of the virus. These drugs are effective as prophylactics and before inflammatory and immune responses are generated.

Empirical therapy for serious infections should use a combination of a broad-spectrum -lactam. Although most isolates are resistant to penicillins, the bacteria are uniformly susceptible to other antibiotics. No pathogens were isolated on routine stool culture, but specimens were also inoculated on a Campylobacter-selective medium and incubated microaerophilically at 40° C. Examination of the plates after 42 hours revealed the presence of flat, nonhemolytic, mucoid colonies that were subsequently identified as Campylobacter jejuni. Campylobacter and Helicobacter are now widely recognized as significant human pathogens; however, they were only discovered in the last 20 to 30 years. Campylobacter is thin, at the resolving power of light microscopy, and is not typically observed in Gramstained specimens. Helicobacter is also difficult to grow, requiring enriched media, a microaerophilic atmosphere, and prolonged incubation. The bacteria are actively motile and rapidly penetrate through the gastric mucus and adhere to gastric epithelial cells, followed by penetration into the cells. Members of these families share two important properties that contribute to problems with recovering the organisms in culture and identification by traditional biochemical testing: (1) microaerophilic growth requirements. Because of this, the clinical significance of two important human pathogens, Campylobacter and Helicobacter (Table 28-1), was only recently appreciated. These properties have been exploited for the selective isolation of pathogenic campylobacters in stool specimens. Although this property led to the initial discovery of campylobacters (stools were filtered looking for viruses), filtration of stool specimens is a cumbersome procedure and is not used in clinical laboratories. A total of 33 species and 14 subspecies are now recognized, many of which are associated with human disease, but only four species are common human pathogens (Table 28-2). Campylobacter is the most common cause of bacterial gastroenteritis in both developed and developing countries, with Campylobacter jejuni responsible for most infections and Campylobacter coli associated with a minority of cases of Campylobacter gastroenteritis in the United States (more commonly observed in developing countries). The incidence of gastroenteritis caused by Campylobacter upsaliensis is unknown because the organism is inhibited by the antibiotics used in isolation media for other campylobacters; however, some have estimated that 10% of Campylobacter gastroenteritis is caused by this bacterium. A variety of other species are rare causes of gastroenteritis or systemic infections, with one exception. Unlike other Campylobacter species, Campylobacter fetus is primarily responsible for causing systemic infections such as bacteremia, septic thrombophlebitis, arthritis, septic abortion, and meningitis. Pathogenesis and Immunity Although adhesins, cytotoxic enzymes, and enterotoxins have been detected in C. The organisms are killed when exposed to gastric acids, so conditions that decrease or neutralize gastric acid secretion favor disease. People living in a population of high endemic disease develop measurable levels of specific serum and secretory antibodies and have less severe disease. As would be expected, patients with hypogammaglobulinemia have prolonged severe disease with C. The mucosal surface appears ulcerated, edematous, and bloody, with crypt abscesses in the epithelial glands and infiltration of the lamina propria with neutrophils, mononuclear cells, and eosinophils. Another immune-related late complication of Campylobacter infections is reactive arthritis, a condition characterized by joint pain and swelling involving the hands, ankles, and knees and persisting from 1 week to several months. Bacteremia is particularly common in debilitated and immunocompromised patients, such as those with liver disease, diabetes mellitus, chronic alcoholism, or malignancies. However, the precise roles of cytopathic toxins, enterotoxins, and endotoxic activity that have been detected in C. Although this is an uncommon complication of Campylobacter disease (1 in 1000 diagnosed infections), the syndrome has been associated with specific serotypes (primarily C. It is believed that the pathogenesis of this disease is related to antigenic crossreactivity between the surface lipooligosaccharides of some strains of Campylobacter and peripheral nerve gangliosides. Thus antibodies directed against specific strains of Campylobacter can damage neural tissue in the peripheral Campylobacter infections are zoonotic, with a variety of animals serving as reservoirs (see Table 28-2). Fecaloral transmission from person-to-person contact may also occur, but it is uncommon for the disease to be transmitted by food handlers. The actual incidence of Campylobacter infections is unknown because disease is not reported to public health officials.
This chapter provides a general description of the principles of specimen collection and processing necessary to diagnose most parasitic infections. Specific details of these and other procedures of general and limited usefulness may be found in several reference texts listed in the Bibliography. Understanding the life cycle of parasitic organisms is a key to understanding important features of geographic distribution, transmission, and pathogenesis of many parasitic diseases. For example, in the life cycle of filariae that infect humans, certain species. Sampling the blood of such patients during daytime hours may fail to detect the microfilariae, whereas blood specimens collected between 10 pm and 4 am may demonstrate many microfilariae. Likewise, intestinal nematodes such as Ascaris lumbricoides and hookworm, which reside in the lumen of the intestine, produce large numbers of eggs that can be detected easily in the stool of an infected patient. In contrast, another intestinal nematode, Strongyloides stercoralis, lays its eggs in the bowel wall rather than in the intestinal lumen. As a result, the eggs are rarely seen on stool examination; to make the diagnosis, the parasitologist must be alert for the presence of larvae. Finally, parasites may cause clinical symptoms at a time when diagnostic forms are not yet present in the usual site. For example, in certain intestinal nematode infections, migration of larvae through the tissues may cause intense symptomatology weeks before the characteristic eggs are present in feces. Because the majority of parasitologic examinations and identifications are based entirely on recognizing the characteristic morphology of the organisms, any condition that may obscure or distort the morphologic appearance of the parasite may result in an erroneous identification or missed diagnosis. As noted previously and in Box 71-1, there may be alternatives to microscopy for detection and identification of certain parasites. Sampling of perianal skin is a useful means of recovering the eggs of Enterobius vermicularis (pinworm) or Taenia species (tapeworm). Fecal Specimen Collection Patients, clinicians, and laboratory personnel must be properly instructed on collection and handling of specimens. Fecal specimens should be collected in clean wide-mouthed, waterproof containers with a tight-fitting lid to ensure and maintain adequate moisture. Specimens must not be contaminated with water, soil, or urine, because water and soil may contain free-living organisms that can be mistaken for human parasites, and urine can destroy motile trophozoites and may cause helminth eggs to hatch. Specimen collection should be delayed for 5 to 10 days to allow barium to clear and for at least 2 weeks after antibiotics such as tetracycline to allow intestinal parasites to recover from the toxic (but not curative) effects of the drugs. Purged specimens may be collected when organisms are not detected in normally passed fecal specimens; however, only certain purgatives (sodium sulfate and buffered sodium biphosphate [phosphosoda]) are satisfactory. One series of purged specimens may be examined in place of or in addition to a series of normally passed specimens. Unpreserved formed fecal specimens should arrive in the laboratory within 2 hours after passage. If the stool is liquid and thus more likely to contain trophozoites, it should reach the laboratory for examination within 30 minutes. The number of specimens required to demonstrate intestinal parasites varies depending on the quality of the specimen submitted, the accuracy of the examination performed, the severity of the infection, and the purpose for which the examination is made. If the physician is interested only in determining the presence or absence of helminths, one or two examinations may suffice, provided concentration methods are used. For a routine parasitic examination, a total of three fecal specimens is recommended. The examination of three specimens using a combination of techniques ensures detection of more than 99% of infections. In a survey conducted in the United States, examination of three specimens was required to detect 100% of infected patients (Table 71-3). It is inappropriate for multiple specimens to be collected on the same patient on the same day. It is also not recommended for the three specimens to be submitted one each day for 3 consecutive days.
References:




