In those with a history of occupational asthma, 39/56 demonstrated bronchial hyperresponsiveness on challenge testing with histamine. Bronchial challenge was carried out in 32/64 workers with a history of occupational asthma and 14 with exacerbation of asthma on return to work. The test was conducted with a boiling water extract of crab or with subjects standing close to boiling pots whilst at work. Progressive deterioration in serial peak expiratory flow rate measurements at work with improvement on cessation of exposure was noted in 12/14 with satisfactory recordings. A significant increase in bronchial hyperresponsiveness after return to work was observed in 16 cases and significant eosinophilia was demonstrated in 15/27 subjects. It was concluded that the results of the challenge and lung function tests confirmed occupational asthma in a total of 46 cases. Certainly a significant proportion of the workforce studied developed asthma as a result of exposure to crab. Respiratory symptoms of 186 workers at 3 king crab processing plants have been compared with those of 36 workers in a fish processing factory (Orford and Wilson, 1985). Pulmonary function, measured prior to and immediately after work, was assessed in 15 subjects from the first and 11 from the second group. Despite having smoked less than fish processors, crab processors had a greater frequency of respiratory symptoms. Further analysis of individual data revealed significant impairment of pulmonary function related to work in 2 crab process workers. In a case study, a chef presented with wheezing, dyspnoea and cough 4 years after starting work involving the preparation of lobster (Patel and Cockcroft, 1990). Spirometry showed reversible airflow obstruction and histamine challenge revealed marked airway hyperresponsiveness. In a study of 57 workers involved in shrimp and clam production, exposure to shrimps gave rise to rhinoconjunctiuvitis in 3 and asthma in 2 subjects (Desjardins et al. Asthma in one individual was confirmed by a positive challenge reaction to a mixture of shrimp with lactose. Corresponding figures for a skin prick test using prawn extract were 7/17 and 6/32. A skin prick test in a worker involved in cooking of prawns was positive with prawn extract and prawn broth as well as crab and crayfish (Dugue et al. Levels of serum IgE and IgG antibodies to prawn antigens were measured in 26 workers complaining of respiratory symptoms resulting from working in a prawn processing factory (McSharry et al. All subjects worked in an area where meat was extracted from the prawns by water jets, generating an aerosol. Each symptomatic worker was matched for age, sex and years of exposure with an asymptomatic control subject working in the same part of the factory. Specific IgE to prawn 31 antigens was detected in 15 workers with symptoms and in one asymptomatic worker. In a study of a single case of occupational asthma related to shrimpmeal exposure, a skin prick test to shrimpmeal was positive and specific IgE to shrimp and crab was identified (Carino et al. A skin prick test using crab extracts was conducted on 303 workers involved with snow crab processing (Cartier et al. Interpretable skin reactions occurred in 298, 65 of which were positive (27/44 with occupational asthma, 38/254 without). Further study of these workers showed a significant relationship between the presence of immediate skin reactivity or increased serum levels of specific IgE to crab extracts and the occurrence of occupational asthma (Cartier et al. In a study of 57 workers involved in shrimp and clam production, 9 showed a positive skin prick test to shrimp and 8 showed an increase in specific IgE to shrimp (Desjardins et al. Intradermal skin tests, using crab antigens, among 15 king crab processors produced a positive response in 9 cases (Orford and Wilson, 1985). A positive skin prick test to lobster extract has been observed in a case of occupational asthma due to handling of lobster by a chef (Patel and Cockcroft, 1990). Similarly, mechanistic information is sparse, but it is clear that an immunological response occurs in a proportion of exposed, symptomatic workers. It has been reported that most workers exposed to the dust experience respiratory and mucosal irritation (Armeli, 1968; Graham et al.
Syndromes

Used to adverse childhood experiences - Potentially traumatic events that occur in childhood. These events can include violence, abuse, neglect, separation, substance abuse, mental health problems, or witnessing a family suicide. Climate change encompasses both increases and decreases in temperature, as well as shifts in precipitation, changing risk of certain types of severe weather events, and changes to other features of the climate system. This type of forecast significantly reduces errors in model output and enables a level of certainty to be placed on the projections. More broadly: Rather than relying on the outcome of a single climate model, scientists run ensembles of many models. Each model in the ensemble plausibly represents the real world, but as the models differ somewhat they produce different outcomes. Those analyses provide both the projection of the future resulting from the ensemble of models, and define the level of certainty that should be placed on that projection. Weather is what conditions of the atmosphere are over a short period of time, and climate is how the atmosphere "behaves" over relatively long periods of time. Evaporation takes place at the surface of a liquid, where molecules with the highest kinetic energy are able to escape. When this happens, the average kinetic energy of the liquid is lowered and its temperature decreases. In contrast, La Niсa (cooling phase) generally means cooler (and sometimes wetter) winters for Montanans. The two phases each last approximately 6-18 months, and oscillate between the two phases approximately every 3-4 yr. They are the most advanced tools currently available for simulating the response of the global climate system to increasing greenhouse gas concentrations. Earth relies on the warming effect of greenhouse gases to sustain life, but increases in greenhouse gases, particularly carbon dioxide from the burning of fossil fuels, can increase average global temperatures over historical norms. In medicine, an intervention is generally undertaken to help treat or cure a condition. Combustion of fossil fuels, agricultural activities, and industrial practices contribute to the emissions of greenhouse gases. Because climate systems are complex, increases in global average temperatures do not mean increased temperatures everywhere on Earth, nor that temperatures in a given year will be warmer than the year before (which represents weather, not climate). Microclimate is usually, however, characterized by considerable uniformity of climate over the site involved and relatively local when compared to its enveloping macroclimate. The differences generally stem from local climate factors such as elevation and exposure. It can be thought of as the depth of water that would theoretically result if you melted the entire snowpack instantaneously. Soil moisture is a pathogen - Microorganisms, viruses, and parasites that can cause disease. Limited to crops harvested solely for dry grain, thereby excluding crops harvested green for food, oil extraction, and those that are used exclusively for sowing purposes. It is a measure of the condition of water relative to the requirements of one or more biotic species and/or to any human need or purpose. Similar terms include basin, sub-watershed, drainage basin, catchment, and catch basin. She has an international reputation as a highly respected health equity researcher based on her work in community-based participatory research, working in partnership with communities to understand and solve health challenges using both scientific rigor and crucial community knowledge. Her work also includes leading a large collective impact project on statewide obesity prevention and health promotion with over 3000 community, public health, and academic partners in Wisconsin. He worked for roughly 11 years as lead environmental engineer for a Hewlett-Packard business unit. Scott has authored, co-authored, or edited two environmental impact statements, book chapters, technical papers, five popular press books, and successful proposals totaling tens of millions of dollars. Angelina Gonzalez-Aller PhD is a researcher, educator, and organizer working at the intersections of health, climate change, and social justice. Angelina currently works at the Center for Large Landscape Conservation as the Community Resilience Program Manager where she strives to support communities in their efforts to achieve conservation goals and prepare for a changing world. Philip Higuera PhD is an Associate Professor of fire ecology in the Department of Ecosystem and Conservation Sciences at the University of Montana. He directs the PaleoEcology and Fire Ecology Lab, funded largely from the National Science Foundation and Joint Fire Science Program, and he teaches undergraduate and graduate courses in fire and disturbance ecology.
Criteria for Discontinuation of Protocol Treatment Progression of disease during the "blinded component" of the protocol; (note that patients would potentially be eligible for unblinded bevacizumab and approved combination regimens with bevacizumab see 11. The methods for analyzing these images will be standardized and are more fully described in the next paragraph. This will include initial visual assessments, but the manual quantitative measurements and semi-automated analyses of regions of interest will provide the majority of work and address the specific aims of the study (see Section 2. Two neuroradiologists will perform readings at different reading sessions to ensure that the interpretations will remain independent and the readers will perform each analysis in the case set. If readings are discordant, a third radiologist will adjudicate and determine the measurement category for the dataset. The readers will be blinded to the order of the scans but will interpret the data from all time points available. This approach will ensure that images are appropriately compared and will limit the confusion from differences in boundaries. Reader bias will be decreased by alternating temporal sequence, blinding any previous interreader results, and suppressing survival outcomes. In addition, we plan to incorporate the Vasari common data elements for the baseline scan for each case. Each set of two technologists will be paired with one of the central readers, and technologists will perform their contours blinded to the imaging time-point. Patients will be identified by initials only (first middle last); if there is no middle initial, a hyphen will be used (first-last). Last names with apostrophes will be identified by the first letter of the last name. The e-mail must include study and case numbers or, if the data is phantom, "dry run" or "benchmark". For exams submitted via electronic transmission, complete this worksheet and fax to (215) 9231737. For exams submitted via media, complete this worksheet and include with the media shipment. The research associate may use the calendar as a case management tool for data submission and follow-up scheduling. Each web form is separated into modules; each module must be completed sequentially in order for the internal programming to be accurate. The user selects the link to the appropriate form and enters data directly into the web-based form. As information is entered into the web form application, various logic checks will be performed. These logic checks look for data that are missing, out of range, or in the wrong format. Such errors will be detected as soon as the user attempts to either submit the form or move to the next data element. Forms that are not completed in one sitting can still be submitted and completed at a later date. The form will remain available on the web until the "Complete Form" button is depressed. E-mail confirmation of web data entry is automatically generated and sent to the site investigator or research associate listing all of the data generated and just submitted. Access to the system is controlled by a sequence of identification codes and passwords. A protocol-specific validation program is used to perform more extensive data checks for accuracy and completeness. Future Forms Due Reports may be sent on an as-needed basis in addition to past due reports. Progression-free survival, defined as the interval from randomization to progression or death, whichever occurs first Secondary Endpoint Treatment-related toxicity. Limited published data exist concerning the effects of bevacizumab with and without temozolomide on these endpoints as well. Performance status is inadequate as a proxy for formal measurement of neurocognitive function, symptoms and health-related quality of life.
Teach parents danger signs requiring child to return immediately and ensure a 14-day follow-up appointment is made. Green area: "Does not have cancer" the child has been placed in the green area of the classification; this means that for the time being the child does not have any sign or symptom suggestive of cancer. Make sure growth and development monitoring and immunization are done, and teach the mother preventive health measures, such as: Maintaining a smoke-free environment. Decrease high-fat foods, such as fried food, primarily if the child is overweight or obese. This objective means that the staff rapidly resolves all administrative problems that occur and, without taking a long time to conduct paraclinical tests, sends the child to a specialized center where in the end any diagnosis will be confirmed or ruled out. If the cancer diagnosis is fortunately ruled out, in any case the symptoms reported are critical and study is needed to diagnose the underlying disease causing them. Once we have a child with a probable diagnosis of cancer, based on a proper clinical history, a complete physical exam, and the identification of suspicious signs or symptoms, the final diagnosis is anatomopathological, carried out in a referral facility. Hence, the importance of understanding that, when there is a suspected possibility of cancer, the child should be referred to a center that specializes in its diagnosis. Although it is necessary to refer the child immediately, it is important to do so under appropriate conditions. Some children will definitely need to be stabilized before being sent to a specialized center, as described below. Oxygen Every child classified with severe or very severe disease, with danger signs, with respiratory problems, or symptoms of shock, and all those who required any resuscitation procedure, should be referred with supplementary oxygen. There is no ideal method for providing oxygen, nor is there one method that is better than another. How oxygen is administered depends on the availability of equipment, the adaptation of the child to the method (mask or nasal cannula), and the required concentration of oxygen. Hemodynamic stability A child with signs of severe dehydration, or with hypovolemia of another etiology, or shock should be stabilized before referral. Lack of a pediatric blood pressure monitor is no excuse for not doing a good assessment of volume status. In this regard, it is necessary to know that some clinical signs are good predictors of hypovolemia and low perfusion and of the need to improve volume. It is important to remember, however, that some children with cancer can have severe anemia, which means that a rapid load of fluids can produce pulmonary edema in them. Systematic use of these protocols is the factor that has made the biggest difference in improving pediatric cancer cure rates-at present, some 70% of children diagnosed with cancer survive. Even more, it is expected that these high cure rates will mean that in coming years, one out of every thousand young people will be a survivor of childhood cancer. For this reason, the current treatment focus for pediatric cancer is aimed at curing, but with the fewest adverse effects possible. These statistics and these goals, however, are still not the reality in Latin America and the Caribbean. This is because in our countries, and even when health services use the same protocols as developed countries, children with signs and symptoms of cancer do not visit the clinic, or they go very late, or they drop out of treatment, or, for various reasons, they do not receive the right treatment at the right time. This module is not meant to teach proper treatment for each of the types of cancer that can affect children, but instead it focuses on the early diagnosis and proper referral of the child to the appropriate health facility. Its purpose is to have the entire health care team, starting at the first level of care, work to offer the child with cancer the best chances possible for survival. In the newborn, 10% dextrose should be administered without electrolytes at 80 mL/kg/day, via umbilical catheter or, if possible, by peripheral vein. From the second day of life, sodium chloride (10 ml/500 ml solution) should be added to the fluids, and from the third day, potassium chloride (5 ml/500 ml solution). The infant older than 2 months referred with intravenous fluids should receive, if there is no dehydration or shock, 5% dextrose with electrolytes in volumes calculated as follows (Holliday-Segar method, based on water and calorie requirements): <10 kg: 10-20 kg: >20 kg: 100 ml/kg/day 1000 ml + (50 ml/kg per each kg >10 kg) per day 1500 ml + (20 ml/kg per each kg >20 kg) per day these are maintenance fluids in a child without oral access or that requires venous access, but does not have dehydration or shock. Pain management If the child is in pain, treat before referring: Mild pain: Paracetamol 10-20 mg/kg/dose every 4-6 hours Mild or moderate pain: Ibuprofen: 5-10 mg/kg/dose every 6 hours Diclofenac: 1-1. Management of intracranial hypertension If a patient with a suspected brain tumor is exhibiting neurological deterioration, you must begin management of intracranial hypertension before referring, according to these steps: Bed rest with head of bed elevated 45°. Administration of high doses of steroids: intramuscular or intravenous dexamethasone at a rate of 0.
Bronchial challenge tests, which were poorly described, were performed on 30 of the patients with asthma, and 13 reacted to an extract of the storage mite. In these cases it was not possible to tell whether the storage mite or the flour dust had induced the asthma. Four single cases (3 European, 1 Canadian) of occupational asthma with positive bronchial challenges to storage mite extracts have also been reported (Warren et al. While these do not provide the same strength of evidence as bronchial challenges, they do confirm the allergenicity of storage mites and their ability to provoke reactions in the upper respiratory tract. In the study by Musken and Bergmann (1992), described above, 148 nasal challenges were carried out in people who had given positive intradermal tests with storage mite. Only about 10% were positive, but whether these findings correlated with symptoms was not discussed. One hundred and six dairy farmers from Finland took part in a study of nasal challenges with storage mite species and cow dander extract (Terho et al. Eighty six suffered from rhinitis with or without asthma, while 20 were free of respiratory disease. Nasal challenge was carried out with storage mite in 63, with cow dander in 70 and with both in 27. Eighteen percent of the symptomatic farmers proved positive in nasal challenges to storage mite, and 20% to cow dander, with only a few reacting to both. Thus in this study population, farmers tended to be allergic to either storage mite or cow dander. There are no studies in which the prevalence of occupational asthma due to storage mite has been estimated from positive bronchial challenge tests. However, in two Scandinavian studies asthmatic symptoms have been correlated with the results of immunological tests, giving prevalences of 6. Using similar criteria, an Italian study of 149 farmers compared to 148 controls indicated a prevalence of approximately 1% (Patussi et al. Thus the prevalence in farmers is 1 to 2% with a higher rate (6%) amongst those working solely with grain. In some of these studies, positive specific IgE has correlated well with bronchial challenge results or with symptoms (Warren et al. However, in other investigations there have been indications that the presence of specific IgE reflects exposure rather than the development of symptoms, and it was considered that only 10% of skin prick tests were clinically relevant (Musken and Bergmann, 1992; Marx et al. The lack of cross-response to bronchial challenges with storage mite and house dust mite discussed above suggests that any cross-reactivity that exists may not be clinically relevant (van Hage-Hamsten et al. Allergologie 15; 202-209 Patussi V, Mazzucato S, Lorusso A et al (1994) Storage mites and their role in the onset of asthma and oculorhinitis among cattle farmers in north-east Italy Med Lav. The main source of occupational exposure to fungal alpha amylase is in the baking industry. However, the precise incidence of occupational asthma in bakery workers specifically attributable to fungal alpha amylase, as opposed to flour or other allergens encountered in baking, is difficult to judge from the information available. Within industry the most commonly used alpha amylases are those of fungal and bacterial origin. Fungal alpha amylase is used for the preparation of flour improvers and subsequently in flour milling and bread baking; also to a lesser extent in starch hydrolysis and alcohol production. Bacterial alpha amylase is used in the manufacture of detergents and animal feeds; also for starch hydrolysis, textile processing and brewing. It is not clear how many workers are exposed to concentrated fungal alpha amylase and bacterial alpha amylase preparations. However, many tens of thousands of workers are potentially exposed to lower concentrations of these enzymes. Small-scale laboratory uses have been identified for porcine pancreatic alpha amylase, but little information is available for this area of use. The 2 subjects with symptoms of asthma underwent bronchial challenge testing using a double-blind protocol. One showed slight bronchial hyperesponsiveness with methacholine challenge, the other was unresponsive.
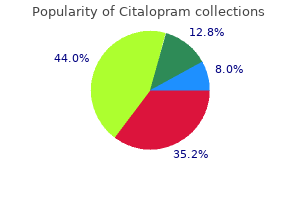
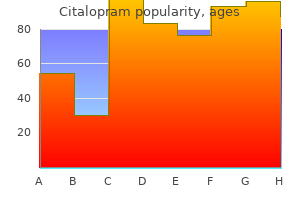
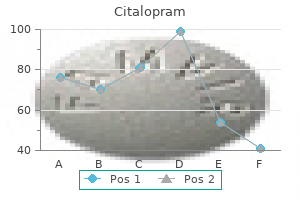
Cynanchum vincetoxicum (German Ipecac). Citalopram.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96658
Hidden in plain sight - reconsidering the use of race correction in clinical algorithms. Clinically relevant and minimally invasive tumor surveillance of pediatric diffuse midline gliomas using patient-derived liquid biopsy. Non-invasive early detection of cancer four years before conventional diagnosis using a blood test. Pulmonary venous circulating tumor cell dissemination before tumor resection and disease relapse. Use of tumor-infiltrating lymphocytes and interleukin-2 in the immunotherapy of patients with metastatic melanoma. Immune recognition of somatic mutations leading to complete durable regression in metastatic breast cancer. Dendritic cell paucity leads to dysfunctional immune surveillance in pancreatic cancer. Adjuvant therapy Additional cancer treatment that is Breast cancer Cancer that forms in tissues of the breast. Adjuvant therapy may include chemotherapy, radiotherapy, hormone therapy, targeted therapy, or immunotherapy. Another type of breast cancer is lobular carcinoma, which begins in the lobules (milk glands) of the breast. Invasive breast cancer is breast cancer that has spread from where it began in the breast ducts or lobules to surrounding normal tissue. Antibodydrug conjugate A therapeutic comprising an antibody chemically linked to a cytotoxic chemotherapeutic. The antibody binds to specific proteins on the surface of certain types of cells, including cancer cells. The linked cytotoxic chemotherapeutic enters these cells and kills them without harming nearby cells. B cell A type of immune cell that makes proteins, called antibodies, which bind to microorganisms and other foreign substances, and help fight infections. Big data Data sets that are too large and complex for processing by traditional database management tools. It is found inside certain cell types- in particular, B cells (see B cell)-where it is involved in signaling pathways (see Signaling pathway/signaling network) that promote cell survival and multiplication. These signaling pathways are very important for survival of cancers arising in B cells, including chronic lymphocytic leukemia and mantle cell lymphoma. Cancer A term for diseases in which abnormal cells divide Biomarker A biological molecule found in blood or other body fluids or tissues that is a sign of a normal or abnormal process, or of a condition or disease. A biomarker may be used to see how well the body responds to a treatment for a disease or condition. It is found inside certain cell types, where it is involved in sending signals that direct cell proliferation. Cancer cells can also spread to other parts of the body through the blood and lymph systems. Sarcomas begin in bone, cartilage, fat, muscle, blood vessels, or other connective or supportive tissue. Leukemias arise in blood-forming tissue, such as the bone marrow, and cause large numbers of abnormal blood cells to be produced and enter the blood. The two main types of cervical cancer are squamous cell carcinoma and adenocarcinoma. Normal cells of the cervix do not suddenly become cancerous; they first gradually develop precancerous changes, then later turn into cancer. These changes can be detected by the Papanicolaou (Pap) test and treated to prevent the development of cancer. Death rates may be reported for people who have a certain disease; who live in one area of the country; or who are of a certain gender, age, or ethnic group. Gene the functional and physical unit of heredity passed from parent to offspring. Leukemia Cancer that starts in blood-forming tissue, such as the bone marrow, and causes large numbers of blood cells to be produced and enter the bloodstream.
Genetic testing may be negative in up to 50% of the cases that meet the clinical criteria. Associated with increased risk of sporadic mismatch repair-deficient colorectal cancer. Risk factors and protective factors for colorectal cancera Evidence grade b Strong convincing Reduced risk Physical activityc,d Increment/contrast Higher versus lower levels Increased risk Processed meat Alcoholic beverages Body fatness Adult attained heighte Strong probable Whole grains Foods containing dietary fibre Dairy products Calcium supplements Limited suggestive Foods containing vitamin C Vitamin D f Fish Multivitamin supplements Sufficient evidence a Increment/contrast per 50 g/day > about 2 drinks a day per 90 g/day per 10 g/day per 400 g/day overall (milk: 200 g/day) > 200 mg/day Red meat > 100 g/day Low intake of starchy vegetables Low intake of fruits per 100 g/day Foods containing haem iron < 100 g/day Smoking g Never-smoker/former smoker/current smoker Risk factors and protective factors for colorectal adenomas are generally consistent with those identified for colorectal cancer. Also, risk factors and protective factors for conventional adenomas and for sessile serrated adenomas generally overlap; the main difference is the higher risk of sessile serrated adenoma in women, as opposed to the higher prevalence of conventional adenomas in men [29]. In high-income countries, a dietary pattern characterized by high intakes of red meat, processed meat, sugar-sweetened beverages, refined grains, desserts, and potatoes is associated with a higher risk of colorectal cancer. Two distinct dietary patterns have been associated with risk of colorectal cancer, and the association is stronger for men than for women. A "healthy" pattern, which is associated with a lower risk of colorectal cancer, is characterized by high intakes of fruits and vegetables, whole grains, nuts and legumes, fish and other seafood, and milk and other dairy products. In contrast, an "unhealthy" pattern, which is associated with a higher risk of colorectal cancer, is characterized by high intakes of red meat, processed meat, sugar-sweetened beverages, refined grains, desserts, and potatoes [32]. One of the nutrient patterns is characterized by a high variety of vitamins and minerals, and the other is characterized by vitamin B12, calcium, phosphorus, riboflavin, cholesterol, and total proteins. Adiposity and body fatness Overweight, obesity, and type 2 diabetes (see Chapter 2. Given the worldwide rising prevalence of obesity and type 2 diabetes, these diseases are likely to have significant impacts on colorectal cancer incidence in the future [35]. Public health strategies aimed at reducing the prevalence of obesity, promoting physical activity, and discouraging the consumption of high-energy, obesogenic foods are gradually being implemented in many regions of the world. Although such strategies could, if successful, lead to a reduction in the colorec- Microbiota There is a growing body of experimental and observational evidence implicating the gut microbiome in the development of colorectal cancer (see Chapter 3. However, human studies linking variation in the gut microbiome with colorectal cancer are limited, and more are needed. A small casecontrol study with available faecal samples demonstrated differences between colorectal cancer cases and controls in the relative abundance of bacterial taxa, with enrichment of Bacteroidetes and depletion of Firmicutes in cases [36]. In addition, increased carriage of the genera Fusobacterium, Atopobium, and Porphyromonas has been associated with colorectal cancer [36,37]. Fusobacterium are prevalent in colon tissue, are maintained in distal metastases, and are thought to be pro-inflammatory [38]. Atopobium, a gram-positive anaerobic bacterium, is associated with Crohn disease and was reported to inhibit colonocyte apoptosis in vitro [39]. These studies are consistent with microbiotic imbalance (known as dysbiosis) leading to a pro-inflammatory microenvironment, which is conducive to colorectal tumorigenesis. However, caution is required in the interpretation of casecontrol and cross-sectional studies, because of the potential of reverse causality [40]. Colorectal cancer incidence and mortality have been observed to decline in countries where the Table 5. Screening trial included people 55 years or older, and current population-based programmes offer screening between age 55 years and age 59 years. Available evidence supporting the colonoscopy screening test refers to people aged 50 years and older and suggests that the impact is lower in elderly people (aged > 75 years). In addition, preliminary reports show a reduction in colorectal cancer incidence, mortality, and surgery rates after the introduction of population-based screening programmes [42,44,45]. These findings confirm the beneficial impact of screening on the colorectal cancer burden at the population level. However, screening rates in adults aged 5075 years remain low, and non-adherence to recommended protocols is an important attributable factor for colorectal cancer mortality, in particular in disadvantaged groups. However, screening rates are higher and the gap by socioeconomic status is smaller in settings with organized programmes than in settings with opportunistic screening; this suggests that implementing population-based screening can ensure the organizational framework for enhancing participation, while reducing inequities in access [49,50]. In individuals at average risk, calcium supplementation (> 200 mg/day) was associated with a reduction in risk of colorectal cancer [32], and use of aspirin (daily or alternate-day dose, 75 mg) appeared to reduce colorectal cancer incidence and mortality, after a latency of about 10 years, with a small reduction in all-cause mortality within 10 years of initiating use [52]. The costeffectiveness of an approach combining screening and chemoprevention still needs to be assessed.
Responsiveness is independent of the tumour histology and is driven only by the mutator phenotype as defined by microsatellite instability [38]. The efficacy of this approach is not confined to mismatch repair-defective tumours. Any tumour with a high somatic mutation burden (these include mutagen-induced cancers such as cutaneous cancers and smoking-related non-small cell lung tumours) is likely to respond to immunotherapy, and this approach offers considerable promise in the treatment of a significant subgroup of human cancers. Detection of carcinogens as mutagens in the Salmonella/microsome test: assay of 300 chemicals. Mutational analysis reveals the origin and therapy-driven evolution of recurrent glioma. Chromothripsis and beyond: rapid genome evolution from complex chromosomal rearrangements. Shanmugam Alan Prem Kumar Gautam Sethi Inflammation Playing a pivotal role in cancer pathogenesis Massimo Tommasino (reviewer) Ioannis P. Modulation of these pro-inflammatory pathways may provide opportunities for both prevention and treatment of chronic diseases, including cancer. Virchow (in the 19th century) and others (in the early 20th century) proposed an association between inflammation and cancer [14]. Worldwide, about 15% of all cancer cases are estimated to be linked to inflammation [5]. Inflammation by itself may not lead to cancer; additional mutations and epigenetic events that occur in the genome of cells as a result of environmental exposures or changes in immunity are also important contributors to oncogenesis [6]. Through the immune response to acute inflammation, activated cells, including macrophages, monocytes, lymphocytes, neutrophils, and leukocytes, are attracted to the injured site and reduce the inflammation (see Chapter 3. Inflammation is a tightly regulated process that can be very effectively turned on or off under normal physiological conditions [7]. Acute inflammation is mainly a selflimiting process and can be treated therapeutically; however, prolonged chronic inflammation is mostly detrimental [6]. Factors linking chronic inflammation and cancer are of great interest, and several lines of evidence suggest that constitutive activation of pro-inflammatory tran- scription factors plays a critical role in the sustained cell proliferation observed in cancers [5]. The majority of cancers are a consequence of chronic inflammation, infection, dysfunctional cell death mechanisms, and dysregulation of cell-cycle molecules. Chronic inflammation is associated with the production of pro-inflammatory cytokines and chemokines, which constitutively activate pro-survival transcription factors that may act as key regulators of carcinogenesis [6]. There are some exceptions; for example, chronic inflammation of the joint or muscle may not lead to the development of cancer. Nonetheless, tumour-associated persistent infection and inflammation are associated with 1520% of cancer deaths worldwide (see Chapter 2. Tumour-caused inflammation, such as necrotic death of cancer cells, insufficient blood supply, and viral infections in the tumour bed, contributes to malignant progression of organ-specific cancers such as liver cancer (see Chapter 5. In addition, in patients who are undergoing chemotherapy or radiotherapy, induced tumour necrosis is often associated with an increase in tumour-associated inflammation, leading to the development of resistance to therapy and/or the induction of anti-tumour immunity. The molecular mechanisms that connect chronic inflammation to cancer development have become a major area of research. Other notable transcription factors that are implicated in inflammation and tumorigenesis are also discussed, i. Finally, opportunities for the prevention and treatment of inflammationdriven cancers are described. These proteins have a key role in innate and adaptive immune functions that can regulate proliferation and survival and stimulate angiogenesis, invasion, and migration, thereby leading to metastasis [14]. They have been characterized, and contain in their C terminus up to seven 33-amino acid consensus ankyrin repeats, which regulate proteinprotein interaction and bind to Rel proteins, thereby masking their nuclear localization signal. In 1858, the German physician Virchow postulated that micro-inflammation that results from irritation may lead to the development of cancer. Such conditions, for example colitis and pancreatitis, often predispose to cancer.
Rates of spontaneous and elective abortions, preterm deliveries, gestational age at delivery, and mean birth weight did not differ between the groups. The sample size in this study has 80% power to detect a 5-fold increase in the rate of major malformation. Several studies have reported no apparent adverse short-term effects on the infant when single dose oral or intravenous omeprazole was administered to over 200 pregnant women as premedication for cesarean section under general anesthesia. Reproductive studies conducted with omeprazole on rats at oral doses up to 56 times the human dose and in rabbits at doses up to 56 times the human dose did not show any evidence of teratogenicity. The peak concentration of omeprazole in breast milk was less than 7% of the peak serum concentration. Because omeprazole is excreted in human milk, because of the potential for serious adverse reactions in nursing infants from omeprazole, and because of the potential for tumorigenicity shown for omeprazole in rat carcinogenicity studies, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother. There were no differences in safety and effectiveness between the elderly and younger subjects. Other reported clinical experience has not identified differences in response between the elderly and younger subjects, but greater sensitivity of some older individuals cannot be ruled out. Pharmacokinetic studies have shown the elimination rate was somewhat decreased in the elderly and bioavailability was increased. The plasma clearance of omeprazole was 250 mL/min (about half that of young volunteers) and its plasma half-life averaged one hour, about twice that of young healthy volunteers. Manifestations were variable, but included confusion, drowsiness, blurred vision, tachycardia, nausea, vomiting, diaphoresis, flushing, headache, dry mouth, and other adverse reactions similar to those seen in normal clinical experience. As with the management of any overdose, the possibility of multiple drug ingestion should be considered. For current information on treatment of any drug overdose, contact a Poison Control Center at 1 800-222-1222. Single oral doses of omeprazole at 1350, 1339, and 1200 mg/kg were lethal to mice, rats, and dogs, respectively. Animals given these doses showed sedation, ptosis, tremors, convulsions, and decreased activity, body temperature, and respiratory rate and increased depth of respiration. The structural formula is: Omeprazole is a white to off-white crystalline powder that melts with decomposition at about 155°C. It is a weak base, freely soluble in ethanol and methanol, and slightly soluble in acetone and isopropanol and very slightly soluble in water. The stability of omeprazole is a function of pH; it is rapidly degraded in acid media, but has acceptable stability under alkaline conditions. The empirical formula for omeprazole magnesium is (C17H18N3O3S)2 Mg, the molecular weight is 713. Each delayed-release capsule contains either 10 mg, 20 mg or 40 mg of omeprazole in the form of enteric-coated granules with the following inactive ingredients: cellulose, disodium hydrogen phosphate, hydroxypropyl cellulose, hypromellose, lactose, mannitol, sodium lauryl sulfate and other ingredients. The inactive granules are composed of the following ingredients: citric acid, crospovidone, dextrose, hydroxypropyl cellulose, iron oxide and xantham gum. The omeprazole granules and inactive granules are constituted with water to form a suspension and are given by oral, nasogastric or direct gastric administration. Because this enzyme system is regarded as the acid (proton) pump within the gastric mucosa, omeprazole has been characterized as a gastric acid-pump inhibitor, in that it blocks the final step of acid production. This effect is dose-related and leads to inhibition of both basal and stimulated acid secretion irrespective of the stimulus. Animal studies indicate that after rapid disappearance from plasma, omeprazole can be found within the gastric mucosa for a day or more. Inhibition of secretion is about 50% of maximum at 24 hours and the duration of inhibition lasts up to 72 hours. When the drug is discontinued, secretory activity returns gradually, over 3 to 5 days. The inhibitory effect of omeprazole on acid secretion increases with repeated once-daily dosing, reaching a plateau after four days. Results from numerous studies of the antisecretory effect of multiple doses of 20 mg and 40 mg of omeprazole in normal volunteers and patients are shown below. The "max" value represents determinations at a time of maximum effect (2-6 hours after dosing), while "min" values are those 24 hours after the last dose of omeprazole. Table 1 Range of Mean Values from Multiple Studies of the Mean Antisecretory Effects of Omeprazole After Multiple Daily Dosing Omeprazole Omeprazole Parameter % Decrease in Basal Acid Output % Decrease in Peak Acid Output % Decrease in 24-hr.
Questions 101 to 103 For each test, select the coagulation factor(s) whose functions are measured. A patient is receiving oral warfarin to effect anticoagulation because of an artificial heart valve. A patient with heparin-induced thrombocytopenia is placed on hirudin and undergoes assessment of his clotting function. If the bleeding has ceased, then immediate fiberoptic exploration in the operating room is indicated. If the bleeding is ongoing, several stopgap measures can be attempted while preparing for median sternotomy in the operating room, including inflation of the tracheostomy balloon to attempt compression of the innominate artery, reintubation of the patient with an endotracheal tube, and removal of the tracheostomy and placement of the finger through the site with anterior compression of the innominate artery. No single parameter is 100% predictive; attempted extubation should be based on correction of the underlying pathology, clinical status and hemodynamic stability, and a combination of the following parameters. The rapid shallow breathing index is the ratio of the respiratory rate to tidal volume. There is evidence to suggest that an index between 60 and 105 predicts successful extubation. The minute ventilation, which is the product of the tidal volume and respiratory rate, should be less than 10 L/min. Renal damage caused by precipitation of hemoglobin in the renal tubules is the major serious consequence of hemolysis. This precipitation is inhibited in an alkaline environment and is promoted in an acid environment. Stimulating diuresis with mannitol and alkalinizing the urine with sodium bicarbonate intravenously are indicated procedures. Fluid and potassium intake should be restricted in the presence of severe oliguria or anuria. As a result of these properties, nitrous oxide may cause progressive distension of air-filled spaces during prolonged anesthesia. Since nitrous oxide diffuses into gas-filled compartments faster than nitrogen can diffuse out, its use can lead to worsened distention, which may be undesirable (eg, in an operation for intestinal obstruction). The diagnosis can be made based on bilateral pulmonary infiltrates on chest x-ray, a PaO2/FiO2 ratio of less than 200, and pulmonary wedge pressures of less than 18 mm Hg (low filling pressures exclude the diagnosis of pulmonary edema). Three major physiologic alterations include (1) hypoxemia usually unresponsive to elevations of inspired O2 concentration; (2) decreased pulmonary compliance, as the lungs become progressively stiffer and harder to ventilate; and (3) decreased functional residual capacity. Progressive alveolar collapse occurs owing to leakage of protein-rich fluid into the interstitium and the alveolar spaces with the subsequent radiologic picture of diffuse fluffy infiltrates bilaterally. Ventilatory abnormalities develop that result in shunt formation, decreased resting lung volume, and increased dead-space ventilation. Chronic lung disease, therefore, results in a shift of the curve to the right, which enhances O2 delivery to peripheral tissues. Both disturbances can be resolved with endotracheal intubation and ventilatory support. Agitation can be an early sign of hypoxemia in an elderly patient and should never be ignored. Benzodiazepines such as Ativan in this patient will cause stupor and worsen his hypoxemia and respiratory acidosis. Bicarbonate should not be administered because buffer reserves are already adequate (serum bicarbonate is still 34 mEq/L based on the HendersonHasselbalch equation). At all doses, the diastolic blood pressure can be expected to rise; since coronary perfusion is largely a result of the head of pressure at the coronary ostia, coronary blood flow should be increased. In low doses (1-5 mg/[kg·min]), dopamine affects primarily the dopaminergic receptors. Activation of these receptors causes vasodilation of the renal and mesenteric vasculature and mild vasoconstriction of the peripheral bed, which thereby redirects blood flow to kidneys and bowel. At these low doses, the net effect on the overall vascular resistance may be slight. As the dose rises (2-10 mg/[kg·min]), 1-receptor activity predominates and the inotropic effect on the myocardium leads to increased cardiac output and blood pressure. Above 10 mg/(kg·min), -receptor stimulation causes peripheral vasoconstriction, shifting of blood from extremities to organs, decreased kidney function, and hypertension. The treatment of choice is respiratory support, including mechanical ventilation, as needed. There is no evidence that the patient has pneumonia or any other indication to perform bronchoscopy or to start antibiotics.
References:




