To Lactation Consultant Sunrise 114 legislate an area of care such as this is ridiculous in that it is limiting what we as humans do best, helping each other, by those who are invested and passionate in that area. To decrease the availability of lactation consultants or those who can provide care/assistance can only result in less mothers reaching out in ways they feel comfortable, to those they are comfortable seeking help from. The best ones in our area are not certified, and they would not be able to work anymore. They should be the go-to for problems, but education, evaluations and problem identification can belong to many categories of providers. Midwives and many others involved in birth work have great interest in helping mothers and babies and their experiences and knowledge should never be undervalued. Due to the high rates of tongue/lip ties Seattle Breast Feeding is about 2 -4 weeks out for frenotomies 25. Mothers need to be able to contact their caregiver at all hours for breastfeeding help. The lactation consultants behind this would better serve their communities by building a reputation that has families willing to pay privately for help, rather than building in more alienation and making it harder to get help. All care providers who see end of pregnancy and immediate postpartum and lactating clients need to have basic to excellent lactation training. As a nursing mother in Central Washington I had difficut time finding resources and accessing support to help me with a very specific challenge. The hospital lactation consultants were my only source of support, and they were not familiar with my particular issues. In my experience there have been multiple issues (tongue and lip ties specifically) not picked up by hospital staff (pediatrician, nurse, lactation consultant) that have negatively impacted feeding relationships in our area. Narrowing the number of people available and trained to assist with these matters will negatively impact breastfeeding rates in our area as success with breastfeeding early on typically increases rates of continued breastfeeding. If only a select few can assist with these matters there will be longer wait times, more time and money required and likely a reduction in successful breastfeeding relationships. Care providers trained in these areas that are already being sought out for other care/appointments (such as midwives) should be allowed to continue doing so as our goal is more successful breastfeeding not less. There are many other healthcare professions, such as midwives, who are credentialed, and more than capable of serving breastfeeding women. I have extensive background knowledge and experience with Lactation, and provide excellent, in-home, evidence-based, compassionate care. It is ridiculous that I might not be compensated or allowed to do this important work of Lactation services with all of my clients. They are much more likely to recommend scheduling, nipple shields, and formula (or pumping and feeding with a bottle). If I am unable to help in a relatively short time, my referrals tend to be to their pediatricians and their office nurses, since they seem to have the incentive to satisfy theit clients and seem less competitive towards the midwives. The client usually knows the pediatrician and plans on regular appointments in their office. We should not be taking away the rights of women to seek quality breastfeeding care from qualified professionals. The ability of a woman to access help through experience yet unlicensed care providers they know and trust is very important to young mothers. Making it illegal for them to do so would negatively affect many women in my area. The following comments were submitted on social media, below links to the survey, instead of being submitted as part of the survey: 38. When continuity of care is disrupted, the chance of positive outcome is compromised. If she is forced to find other support, especially in remote areas, her healthcare is limited as well as her right to chose her provider. He just had a lip and tongue tie corrected on Monday and I need some help to correct our poor latch that resulted from the ties. Living in a rural community often limits access to specialized healthcare professionals.
Pain Associated With Previous Dental Treatment Patients may experience acute symptoms following dental treatment. After treatment such as deep caries excavation or an extraction or surgical procedure, acute sequelae may be expected and are predictable occur- Figure 6-8 Periodontal abscess between the first and second molars. In some cases, the discomfort may occur because the treatment was incompletely or improperly done. For example, when an initial and limited debridement is performed on a patient with significant pockets and subgingival deposits, the gingiva may shrink and become firm after the procedure, eliminating the existing pathway for exudate to egress from the periodontal pocket, resulting in a periodontal abscess. The demise of the pulp and development of an apical infection years after placement of a deep restoration is a case in point. Another example is the development of a symptomatic lesion (such as a denture sore or ulcer or a denture stomatitis) in response to changes in the tissues under a prosthesis. In most of these situations, a thorough history and a careful clinical examination usually reveal the problem and its source. When a patient fractures a restoration or prosthesis, he or she may express concern that the problem will cause pain in the future. Immediate treatment is usually not warranted, but the patient deserves an evaluation and a diagnosis that includes a professional opinion regarding the prognosis for the tooth, restoration, or prosthesis, and the likelihood of additional problems. Rendering such an opinion reassures the patient and has important risk management and practice management benefits as well. Other Sources of Oral Pain A small percentage of the patients whose chief complaint is pain have symp- toms that are not related to the teeth or periodontium. This diverse group of problems may present diagnostic difficulties, especially if the patient has trouble localizing the pain. In many situations, the dentist develops a list of possibilities, which by a process of elimination leads to a differential diagnosis. This process can be challenging for the dentist, frustrating for the patient, and time consuming for both. The following paragraphs describe instances of such conditions along with others that are easier to detect. Three common types of ulcers may cause problems for patients: herpetic ulcers, traumatic ulcers, and aphthous ulcers. Patients with herpes zoster may experience acute pain and prodromal itching before the outbreak of characteristic vesiculation and ulceration. Zoster also is expected to present as a unilateral process distributed in a specific dermatome. Traumatic ulcers are diagnosed by their history and location, usually in proximity to a recognizable source of trauma. Aphthous ulcers are usually found on movable tissue in the oral cavity and are typically diagnosed by their characteristic appearance (Figure 6-12). Oral ulcers are often seen in patients with immunocompromising conditions or as a reaction to some medications. The patient in debilitated health or suffering from an autoimmune disorder may be prone to multiple and recurrent vesicles, bullae, erosions, or ulcers. It may be appropriate to refer such patients to an oral medicine specialist, an oral and maxillofacial surgeon, or an internal medicine specialist to confirm the specific cause and recommend treatment. Chapter 6 the Acute Phase of Treatment 127 Figure 6-12 Aphthous ulcer on the buccal mucosa. A patient may have an acute open lock-the patient cannot close the jaw and occlude the teeth-or a closed lock, which prevents normal opening of the mouth. Trigeminal neuralgia is an exquisitely severe, electriclike, lancinating pain that is related to the distribution of the trigeminal nerve. A neuritis can be a deep, constant burning pain that runs the course of a nerve trunk. Trauma to a nerve can produce various symptoms from increased sensation (hyperesthesia); to altered sensation (paresthesia) with burning, itching, or tingling; to complete loss of sensation.
The outbreak of frontier affrays in 1913 and further disagreements about the treaty induced recourse to arbitration. Lardy, a member of the Hague Court of Arbitration, and Swiss Plenipotentiary at Paris, decided in favour of the Dutch view of the track of the eastern frontier of the Ocussi enclave. As various exchanges are recorded to have taken place in November 1916 it may be assumed that the treaty with the decision of the arbitrator is in process of being carried into · effect. The differences between the Dutch and Portuguese on Timor extended to the islands of Solor, Plores, Adunara, Lomblen, Pantar, and Alor (Ombay). From the beginning of their relationship the Portuguese laid claim to certain parts of Flores, Adunara, and Solor. A treaty was therefore negotiated by which the position of the islands was definitely settled, and this treaty was ratified in 1859. The eighth article of the treaty confirmed Hollaad in entire possession of all islands north of Timor to wit, Flores, Adunara, Solor, Lomblen, Pantar, and Alor, with the small - islands belonging to the Solor archipelago. The ninth article states that as compensation for the cession of the above islands Portugal was to be remitted certain debts owed to the Netherlands Government. Present Situation An interesting expression of opinion is that of the State Commission which, in 1913, issued a report on the defences of Netherlands India. Brief reference was made to the situation as it had developed during the previous thirty years Germany had become a colonial power with territory in New Guinea Japan had acquired Formosa, and America the Philippines, while Holland herself had considerably extended her sway in the Malay Archipelago. Further, Japan had become one of the great Powers, Australia was making vigorous progress, and, more recently, there had arisen the possibilities attaching to a republican China. Of importance also were the various combinations of Powers expressed in the Anglo-Japanese Conven;; tion of 1905, the Franco-Japanese Treaty of 1907, the Treaty of 1909 between Japan and America, and the Russo-Japanese Treaty. After expressing some anxiety as to the prospect of a European war it was agreed that the only policy for Holland in the Indies was that of strict neutrality secured by the favourable treatment without partiality of all foreigners and foreign Although it was recognized that Netherlands India capital. The danger is thought to come from Japan, and while some Dutch- are said to accept the annexation of their colony as inevitable, others recommend the fullest naval and military men preparations. It regards, however, the aggrandisement of Japan in the German and Russian spheres in China as averting the danger, and offering an opportunity of initiating a policy of friendship with the Japanese. Algemeen Overzicht van de Uitkomsten van het Wdvaart-onderzoek, gehouden op Java en Madoera in 1904-5. Medededingen van hd Bureau voor de Bestuurszahen der bewerkt door het Encyclopaedisch Bureau. Essai stir les principes regissant V administration de la Justice aux Indes hollandaises. Zeitschrift filr Kolonialpolitik, Kolonialrecht und Kolonialmrtschaft, 1910 (Administration). Overzichthaart of various islands (Borneo 1: and Sumatra, 1: 2,000,000; Celebes, 1,250,000, &c. Acheh: see Achin Achin, 165, 252, 269, 340, 341, 343-346, 348, 352, 356, 415, 436, 440, 487 seg. Adunara, 80, 231, 518, 530 Agave, 326 Ageng, Sultan, 435, 448 Agrarian conditions, 285 Agrarian Law of 1870, 320, 483 Agricultural Ambon see Amboina Amburombo Mt. Banda Sea, 11, 89 Banda-Elat, 218 Banda-Eli, 218 Banda Neira, 65, 206, 216, 382, 445 338 Batjan Battaks Bandayuda R. Boompyes, 32 Bopati, 471 Borneo, British, 10, 13,: Bena, 445 Bena, 402 Bengalis, 164 Bengkalis, 103 seq. Van der, Celebes Sea, 11 Central Moluccas, 382 Central Sumatra Road, 483 Confucianism, 139. Cochin, 525 Cocoa, 281, 322 Coco-nut, 278, 332, 346, 366, 370 see also Copra Coffee, 115, 274, 281, 299, 318, 342, 351, 364, 371, 463, 473, 374, 457,: Deli Railway, 418 Deli River, 392, 393 Deli Tuan, 418 Demak, 304, 334, 434, 435, 455 Dempo Mt. Den Pasar, 425, 512 Departments, 249 Desa, 155, 158, 261 Desa Dayaks, 190 483 Diamonds, 360, 498 Digul R. Java Bank, 292 Java Head, 21 Javana, 455 Javanese,150,188, 248, 268 Java Pool, 376 Java Rebellion, 479 Java Sea, 89 Java, War of, 452 Jelutong, 347, 352, 359 Jember, 92, 425 Jembrana, 508 Kamrau B. Jampuwa, 503 Janssens, Governor-General, 472, 485 Kayoa, 61 410 Juwana, 23, 387, Ke Jb. Japanese, 19, 132, 264, 494, 514 Japara, 23, 448, 455 Jappen see Jobi: K Kaba Mt. Krapiyak, 448 471 Krian, 410 484 Lombok, 83, tenure, 286 Land, Krawang, 405, 409, 425, Langapura, 381 Langkat, 350, 351, 355, 384, 419 Langra, 383 Langsa, 381, 387, 419 Languages, 135, 152; see also 103, 227, 231, 238, 252, 373, 374, 417, 512, 514: Lombok Pk. Misol, 77, 227, 508, 528 Misore: see Schouten 159, N Nagrek, 269 Nangamesi: seeWaingapu Nangamesi Bay, 398 Nangka, 280 Narumonda, 415 Nassau Mts.
There is usually acute fever and toxaemia, although the disease may sometimes run a more chronic course. Penetrating wounds of the chest Immediate application of a dressing is required in order to prevent suction of air into the pleural space. Minor cases require only wound toilet with an underwater intercostal drain to allow escape of any accumulated blood or air in the pleural space. Large wounds demand formal exploration with excision or repair of damaged lung tissue, repair of any diaphragmatic tear and exclusion of injury to underlying abdominal viscera. Special investigations · Chest X-ray shows a solid opacity or a fluid level if the abscess communicates with the bronchus. Cardiac tamponade this may follow open or closed injuries to the chest or upper abdomen. Treatment is emergency surgical exploration; the pericardium is opened, the blood is evacuated and the cardiac laceration sutured. The mainstay of therapy for lung abscess is postural drainage combined with antibiotics. Surgical excision is required only for the small percentage who fail to respond to this therapy, when some underlying cause needs to be treated, or when, in a late case, there is a complicating empyema that requires drainage. Lung abscess Aetiology · Bronchial obstruction secondary to carcinoma of the lung. The chest and lungs 65 Aetiology · Underlying lung disease: pneumonia, bronchiectasis or carcinoma of the lung; tuberculous empyema is now uncommon. Malignant 1 Primary a squamous cell carcinoma; b adenocarcinoma; c small-cell carcinoma; d large-cell carcinoma; e carcinoid. The infecting organisms are usually Pneumococcus, Streptococcus or Staphylococcus. The tumour arises from the mucosa usually of the main bronchus as a cherry-red swelling, which ulcerates and bleeds (hence the common presenting symptom of haemoptysis). The growth may eventually block the bronchus with resulting pulmonary collapse and infection. Although slow growing, it cannot be considered benign, as infiltration and metastases may eventually take place. Occasionally, serotonin (5-hydroxytryptamine) is secreted, producing attacks of flushing and dyspnoea (carcinoid syndrome; see Chapter 23, p. Treatment An acute empyema may respond to repeated aspirations together with antibiotic therapy, based on the sensitivity of the responsible organism and given both systemically and into the pleural cavity. If the condition fails to respond to this treatment, drainage by means of excision of a rib overlying the empyema becomes necessary. An intercostal tube is inserted and progress followed by repeated sinograms to ensure adequate drainage and ultimate obliteration of the empyema cavity. In women, it accounts for 11% of all new cancers, and is the third commonest cancer in women after breast (31%) and colorectal cancer (12%). The lung segments distal to the occlusion may show collapse, bronchiectasis or abscess formation. Mostly poorly differentiated and arising in an area of squamous metaplasia of bronchial epithelium. Very rapidly growing tumour often found in the periphery of the lung, associated with a large fibrotic (desmoplastic) reaction. Large cells containing abundant cytoplasm and without evidence of squamous or glandular differentiation. This has neuroendocrine properties and produces peptides giving rise to paraneoplastic syndromes (Chapter 7, p. It has a poor prognosis, has generally spread by the time of diagnosis and is best treated by chemotherapy. Passive smoking, air pollution with diesel, petrol and other volatile hydrocarbon fumes, asbestos exposure and exposure to radioactive gases such as radon in uranium mines are also predisposing factors. Carcinoma of the lung has an extremely poor prognosis, and the gravity of this condition should be impressed on all patients who are inveterate smokers. There is an increased incidence of carcinoma of the lung even in patients who smoke only a few cigarettes a day, and this danger is greatly increased in patients smoking more than 20 cigarettes a day for a number of years. Compression of the superior vena cava by massive mediastinal node involvement produces gross oedema and cyanosis of the face and upper limbs (superior vena cava syndrome). Pathology There used to be a considerable predominance of men over women in this disease (6:1 in the 1950s), but the ratio is decreasing as women tend to smoke more and men less.
A suggested outline for adjuvant systemic therapy is as follows: 1 Premenopausal women. Survival Several factors are thought to have contributed to increased survival rates for breast cancer, including breast screening, specialist multidisciplinary teams and more individualized treatment plans that optimize each aspect of patient treatment. The 10 year survival is now 72%, with 64% of all women surviving for 20 years as compared with 44% in the 1980s. These figures are likely to improve with recent advances in hormone therapy, chemotherapy and targeted therapies such as trastuzumab. Inoperable and locally advanced tumours Locally advanced breast cancers are usually defined as tumours greater than 5 cm with or without involved axillary lymph nodes or skin involvement. In patients with locally advanced breast cancer, the overall response rates to chemotherapy are good, although the rate of complete pathological response is rarely more than 15%. As a result, the majority of these patients subsequently proceed to surgery and/or radiotherapy. Following breast-conserving surgery, such as wide local incision for invasive cancer, radiotherapy significantly reduces the risk of recurrence within the breast. In premenopausal women receiving adjuvant chemotherapy, postmastectomy radiotherapy may also improve survival. The factors associated with a high risk of local recurrence are tumour size, high grade, nodal involvement, lymphatic invasion and involvement of deep margins. After all forms of axillary surgery, the decision as to whether the axilla should be irradiated represents a balance between the risks of recurrence and the risk of morbidity. After axillary sampling, the axilla should be irradiated only if node positive or inadequately sampled. If there is doubt about residual disease in the axilla Inflammatory breast cancer Inflammatory breast cancer is rare, representing only 2% of breast cancers. The breast appears swollen, red, firm and warm to touch, all cardinal features of inflammation. Symptoms can appear quite quickly as cancer cells block the small lymphatics in the breast, and mastectomy is usually required. It is an aggressive disease associated with 5 and 10 year survival rates of the order of 50% and 30%, respectively. The combination of chemotherapy, surgery and chest wall radiotherapy is accepted as achieving the highest local control and survival. The breast 307 Patients unfit for surgery these will usually be elderly patients, and some may have locally advanced tumours. The principles of management are closer to those for metastatic disease, the aim of therapy being to control the primary tumour while maintaining the best quality of life. For advanced disseminated disease, chemotherapy can produce reasonable palliation. It presents as a unilateral red, bleeding, eczematous lesion of the nipple and areolar epithelium. It is associated with an intraduct carcinoma of the underlying breast in 50% of cases, which may or may not form a palpable mass. Metastatic disease the aim of treatment is to relieve symptoms while maintaining the highest quality of life. All patients with metastatic disease should be considered for some form of systemic therapy. Hormone therapy is less toxic than chemotherapy and is therefore often used as the first line of treatment. As the disease progresses patients may require referral to palliative care specialists for control of symptoms and to augment support for patients and carers. Treatment Treatment will be determined by any underlying breast carcinoma detected on clinical or radiological investigation. Surgical management includes mastectomy and axillary surgery for lesions associated with invasive disease. In the absence of invasive disease, or if a small central tumour lies close to the nipple, cone excision of the nipple and underlying tissue followed by breast radiotherapy may be considered.
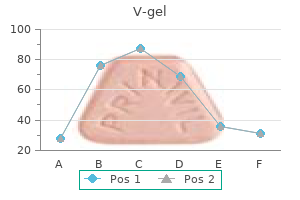
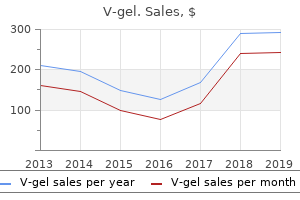
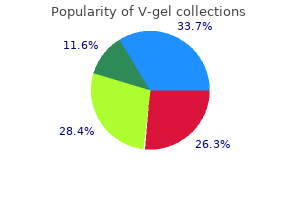
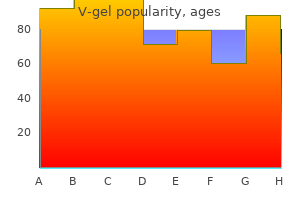
Scutellariae Radix (Baikal Skullcap). V-gel.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96869
His mother is an insulin dependent diabetic who had good control during her pregnancy. Management of gestational diabetes is generally achieved through close glucose monitoring to insure normalization of blood glucose values after dietary and exercise changes. Gestational Diabetes Requiring Insulin- Insulin is added to the treatment plan of a woman with gestational diabetes if good glucose control is not achieved with appropriate changes in diet and exercise. Hypoglycemia: the highest incidence of hypoglycemia occurs 4-6 hours after delivery but can occur any time after delivery up to 48 hours after birth. Normal > 45 mg/dl infants <24 hours of age and > 50 mg/dl infants >24 hours of age P a g e 226 d. Prevention: Good metabolic control in the last trimester may decrease the incidence of neonatal hypoglycemia. Macrosomia: Increased body fat, muscle mass and organomegaly especially of the heart and liver b. Congenital Heart Disease: double-outlet right ventricle, truncus arteriosus, transposition of the great vessels, congestive or hypertrophic cardiomyopathy. The infant may exhibit: tachypnea, respiratory distress, difficulty feeding, tachycardia, +/ cyanosis, abnormal pulses or may be asymptomatic if the defect is mild. Asphyxia: May be associated with macrosomia and may acutely affect respiratory, renal, central nervous system and gastrointestinal functioning. Infants born to mothers with hyperglycemia have upregulated their insulin production to compensate for the higher levels of glucose they experienced in utero. After birth, this increased production of insulin in the infant drives glucose levels down placing the infant at risk for hypoglycemia. Insulin functions as the primary anabolic hormone of fetal growth and development resulting in visceromegaly and macrosomia. A mother with no prenatal care and a history of known substance abuse delivers a baby at term. What special medical and social concerns do you have about caring for this infant? Neonatal abstinence syndrome scoring system- A system of scoring that assigns points based on each symptom of withdrawal the newborn exhibits and its severity. Review of Important Concepts: Historical Points the importance of prenatal care: the primary purposes of prenatal care are to identify and treat complications of pregnancy and fetal health and to promote healthy behaviors. Outcome data suggest that babies born to mothers who do not receive prenatal care are more likely to be of low birth weight and more likely to die compared with babies born to mothers who receive prenatal care. Lack of prenatal testing places the infant at increased risk for a host of diseases and conditions routinely picked up with adequate prenatal care. P a g e 229 Which substances did the mother use and what are the risks to the infant exposed to one or more substances of abuse? Generally, the need for pharmacologic treatment for withdrawal symptoms is limited to neonates exposed to opioids or opiates. Pharmacologic treatment may involve morphine, methadone, phenobarbital, buprenorphine or diazepam. Which classes of drugs have been associated with causing neonatal psychomotor behavior consistent with withdrawal? Seizures during withdrawal are possible with this risk being higher in the methadone exposed infant compared with the infant exposed to heroin. The abnormalities seen in stimulant exposed infants likely represent the effect of the drug and not a withdrawal from the drug. Withdrawal is uncommon but when present, the symptoms may be indistinguishable from narcotic induced withdrawal although milder in severity. Infants exposed to alcohol in utero are at increased risk for Fetal Alcohol Syndrome: a constellation of physical, behavioral and cognitive abnormalities. Social Work Consult: the role of the social worker in this setting is to help evaluate the capability of the mother to provide a safe, supportive environment for her infant. This involves in depth discussions with the mother and often other family members and close friends and relatives.
My views stem from the basics, advance to particulars, and then draw conclusions based back on the basics. In every sense, and as far as possible, self-determination and self-responsible action should be central aims. If one allows the whole "force" of music a base for development, then, the time factor in particular must be considered. For example, it did not pose any major problems for every student of my flute classeight mentally handicapped students to play one song to his satisfaction. The individual charm and the therapeutic effect emanating from individual sounds and the music are not addressed hereafter, let alone questioned. Instead, the intention of my essay is to offer ideas which enable and enhance group music-making. It must be explicitly stated, that this common sense of music is not related to the 134 feeling of inclusion experienced, for example, in heteronomous or group drivensinging at football pitches. This also does not involve the teacher making the music while the students independently enjoy a funny "drum-along" session. Just as the aim of speech training is to ensure the person knows whereof he speaks, or the aim of reading training is to ensure he understands what he reads (German language speaks of catching the meaning by reading), the aim of music education in general as well as instrumental playing with handicapped people is to absorb the original power of meter and rhythm gratefully, participate in it, but still see its aim in the self-understood and self-determined actions as listeners or players. First the fundamentals: Disabled people as well as non-disabled people have a need of music. Disabled people as well as non- disabled people have a need to express themselves and give substance to form their own "internal performance". Disabled people as well as non- disabled people have a need to get involved in discussion by means of music and via music with themselves and others. Disabled people as well as non- disabled people have fun with music, listening to music and incorporating themselves into music in varied ways. The quality grades of musical action (making music, forming music in a similar way, creating music) are thus only superficially quality grades of musical experience. An example may clarify this: lying flatly on water, being carried motionless, is not only a targeted preliminary practice for later swimming but also depends on trust, devotion, willingness to engage and practice. Fast swimming times state nothing about the ability to be carried by water and do not say anything about the pleasure of realizing water and therefore to communicate through it with oneself. The question of course, only asked in secret if it is worth musically educating disabled people is ridiculous and also falsely put, as it is based on false aims and quality features. Even the question which often is raised by music teachers, mostly based on fear of over-challenging handicapped students, as to where the borders of capacity are, (physically and mentally) really only blurs the view of the main questions: 1. Does this self-perception and subsequent communication skill, with the student himself and others therefore enable an appropriate better self-perception and communication ability with others? Does musical communication with others 135 lead to a healthy self-development exist? I will attempt to link both questions through a chain of arguments and try to answer them. You should first more closely examine musical experience without following in my opinion the wrong track cementing a hierarchy within the quality attributes of musical activity. Permit me to: · · · listen to oneself listen to the other person while playing by oneself to differentiate listening to oneself while playing with the others Now you could discuss at cross-purposes whether the image of quality "grades" might make sense. Or whether the levels should really be climbed strictly one after another or built on to each other? Undeniably though there must be a joyful experience which takes place on each level or in each grade. Moreover, people themselves hold the key, depending on what kind of challenge they set themselves. If one overstrains himself, he therefore limits himself and might not get the chance to experience his full potential. If students are asked in their group: "Could you hear the nice sound of the trumpets? I myself doubt whether one should dismiss such a situation as a passing but necessary stage of development. In fact, I believe compellingly in the need, from the outset, of awareness of others being firmly instilled so you can achieve a "healthy" personal musical development.
How do people truly enjoy a restaurant dinner with family, an evening at theater, or the laughter of children if their hearing fails? Hearing loss is a major issue for children as well, affecting nearly one million children in the U. More than 50 years ago, we played a pivotal role in the development of cochlear implantation, thanks to the 37 As German philosopher Immanuel Kant said, " Not seeing separates us from things; not hearing, from our fellow man. Imagine a World in Silence No More What if treatments that repair the damaged inner ear could restore lost hearing, quiet tinnitus, and improve balance? What if we could identify all of the hundreds of genes responsible for hearing loss, instead of only the relatively few that have been identified to date? What if we could identify the genes responsible for noise and drug susceptibilities that could instruct a person to avoid specific challenges to the inner ear in his or her life, thereby preventing early onset age-related hearing loss? And what if we could find a unifying approach to treat a broad spectrum of hearing disorders, including congenital, age-related, and drug- and noise-induced, and provide patient-tailored treatments for these different forms of hearing loss? A simple example of this is our combined effort to broadly study the pathology of noise exposure in animals from molecular changes in cells, cochlear cytomorphology, cochlear anatomy, and cell and systems physiology. In-depth understanding of the pathology allows us to design novel methods to diagnose the precise location of a cochlear defect and to generate tools for repair. Having a team of basic scientists and clinician/scientists allows us to translate results from animal models directly to humans. Eleven world-class researchers at the Stanford School of Medicine, Otolaryngology Head & Neck Surgery Department lead the initiative. Rapid advances in bioscience and technology, many of which originated at Stanford, make it realistic to envision a cure for hearing loss within the foreseeable future. In laboratory animals, we can now regenerate inner ear hair cells, a tantalizing discovery, which we are working hard to adapt for human benefit. The challenge before us is to refine the method and make it safe and effective in humans. These environmental exposures, in combination with the effects of aging and genetic disposition, are causing a worldwide pandemic of hearing loss," says Stefan Heller, PhD. We are motivated to take on the high-risk/ high-impact questions that go beyond the traditional methods of incremental advances. Such approaches are currently very rarely supported by government funding agencies. This synergistic approach allows us to address the most critical questions in the field with the highest innovative spirit possible. Similarly, this understanding also provides clues as to why some people will not lose their hearing even when working in a loud-noise environment for most of their lives. Knowing the genetic mechanisms of "susceptible ears" and also the genetic circumstances that lead to "robust ears" is important for development of drugs that prevent hearing loss. The elegant cochlear spiral and the auditory nerve remain viable, often with only a specific population of hair cells missing. Major strides have been made in regenerating hair cells in the mouse and connecting them to the hearing nerve. Contrary to conventional thought, we are finding that these cells may actually be affected before sensory hair cells are lost. Drugs that stabilize these other structures of the cochlea offer hope in the treatment of individuals at risk for hearing loss. Finding ways to keep these cells healthy may prove a valuable pathway to prevent hearing loss from noise, toxins, or other injury-in ways not possible by focusing on the sensory hair cells alone. Cicero / Stanford University News Service cochlear implants work better and could reduce age-related hearing loss. Ricci and Cheng has yielded insights to prevent antibiotic-related inner ear damage in millions of future patients. Their work has developed novel aminoglycoside antibiotics that lack the side effect of damaging the inner ear, and result in hearing loss and balance impairment in many exposed individuals.
References:




