
Incoordination, tremor, ataxia, confusion, stupor, coma, and even death occur at progressively higher blood alcohol levels. How often during the last year have you been unable to remember what happened the night before because you had been drinking Drug Therapy Several medications may be useful in alcoholic rehabilitation; usually medications are continued for 6 months if a positive response is seen. These receptors mediate the opiate effects of analgesia, euphoria, respiratory depression, and constipation. Endogenous opiate peptides (enkephalins and endorphins) are natural ligands for the opioid receptors and play a role in analgesia, memory, learning, reward, mood regulation, and stress tolerance. The prototypic opiates, morphine and codeine, are derived from the juice of the opium poppy. The semisynthetic drugs produced from morphine include hydromorphone (Dilaudid), diacetylmorphine (heroin), and oxycodone (OxyContin). The purely synthetic opioids and their cousins include meperidine, propoxyphene, diphenoxylate, fentanyl, buprenorphine, tramadol, methadone, and pentazocine. Since 2007, prescription opiates have surpassed marijuana as the most common illicit drug that adolescents initially abuse. Additionally, the adulterants used to "cut" street drugs (quinine, phenacetin, strychnine, antipyrine, caffeine, powdered milk) can produce permanent neurologic damage, including peripheral neuropathy, amblyopia, myelopathy, and leukoencephalopathy; adulterants can also produce an "allergic-like" reaction characterized by decreased alertness, frothy pulmonary edema, and an elevation in blood eosinophil count. Withdrawal Withdrawal produces nausea and diarrhea, coughing, lacrimation, mydriasis, rhinorrhea, diaphoresis, twitching muscles, piloerection, fever, tachypnea, hypertension, diffuse body pain, insomnia, and yawning. Buprenorphine produces fewer withdrawal symptoms compared with methadone but does not appear to result in better outcomes. Completion rates are high, but the approach is highly controversial due to the medical risks and even mortality associated with this approach. Except for the terminally ill, physicians should carefully monitor opioid drug use in their pts, keeping doses as low as is practical and administering them over as short a period as the level of pain would warrant in the average person. In general, screening is most effective when applied to relatively common disorders that carry a large disease burden and have a long latency period. False-positive results can lead to unnecessary lab tests and invasive procedures and can increase pt anxiety. History should include medication use, allergies, vaccination history, dietary history, use of alcohol and tobacco, sexual practices, safety practices (seat belt and helmet use, gun possession), and a thorough family history. Routine measurements should include assessments of height, weight, bodymass index, and blood pressure. While behavioral changes are frequently difficult to achieve, it should be emphasized that studies show even brief (<5 min) tobacco counseling by physicians results in a significant rate of long-term smoking cessation. The top causes of age-specific mortality and corresponding preventative strategies are listed in Table 213-1. Chronic lower either fecal occult blood testing, respiratory disease flexible sigmoidoscopy, or 7.
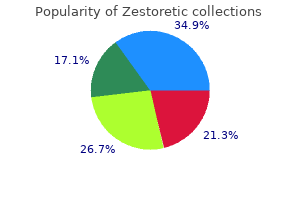
Douglas Spruce (Oregon Fir Balsam). Zestoretic.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96500
However, because of its greater efficacy and lower toxicity, valproate is now preferred for the latter condition. Carbamazepine and phenytoin were associated with the lowest percentage of failures. These agents invariably produce sedation and drowsiness at high doses in adults, whereas children often become hyperactive and irritable even at levels in the therapeutic range. Sedation, usually present at relatively low levels during the first few days of treatment, subsides thereafter as tolerance to this effect develops. Sedation or somnolence reappears only at high therapeutic or supratherapeutic levels, usually 30 mg/L. As dose levels increase further, neurologic toxicity appears, characterized by dysarthria, ataxia, incoordination, and nystagmus. Some differences Chapter 53: Phenobarbital and Primidone 653 persisted 3 to 5 years later (85). In one study of crosssensitivity, among patients who developed a rash on carbamazepine and phenytoin, 26. These include Dupuytren contractures, plantar fibromatosis, heel and knuckle pads, frozen shoulder, and diffuse joint pain (110). Assessment of the specific risk for a given agent in clinical studies has been complicated by polytherapy and the underlying risk for malformation due to maternal epilepsy. Folic acid supplementation taken at 5 to 12 weeks of amenorrhea may decrease the risk of anomalies (112). Because of its long elimination half-life and slow accumulation, the full maintenance dose can be administered on the first treatment day, although steady-state plasma levels will be reached only after 2 to 3 weeks. Close monitoring of plasma levels and dosage reductions may be necessary in patients with advanced renal disease (121) and cirrhosis (122). The rate of administration should not exceed 100 mg/min (2 mg/kg/min in children weighing less than 40 kg). The initial loading dose of 15 to 20 mg/kg in newborns is similar to the dose in children and adults, and will achieve a plasma level of about 20 mg/L. This level can usually be maintained in newborns with a dose of 3 to 4 mg/kg/day (124). The dose can then be increased every 3 days as tolerated, to a final daily maintenance dose of 10 to 20 mg/kg. Maintenance doses are 15 to 25 mg/kg/day in newborns, 10 to 25 mg/kg/day in infants, and 10 to 20 mg/kg/day in children. This phenomenon is due to pharmacodynamic mechanisms that cause a state of rebound hyperexcitability when the amount of the drug decreases in the brain, resulting in a lower seizure threshold, and predisposing the patient to more severe than usual seizures or even to status epilepticus. Effect of phenobarbital on cortical after-discharge and overt seizure patterns in the rat. Barbiturate reduction of calcium-dependent action potentials: correlation with anesthetic action. Research on the significance of phenobarbital, produced by biotransformation, for the anticonvulsant action of pyrimidone [German]. Seizure protection, neurotoxicity, and therapeutic index of individual compounds in mice. Seizure protection, neurotoxicity, and therapeutic index of varying combinations in mice. Comparison of the anticonvulsant efficacy of primidone and phenobarbital during chronic treatment of amygdalakindled rats. Plasma concentrations of phenobarbital in the treatment of seizures in the newborn. Relative bioavailability of rectally administered phenobarbital sodium parenteral solution. Primidone and phenobarbital during lactation period in epileptic women: total and free drug serum levels in the nursed infants and their effects on neonatal behavior. Phenobarbital and phenytoin in neonatal seizures: metabolism and tissue distribution. The solid straight line connects the corresponding predicted values (5, 10, 15, and 20 mg/L). Metabolic disposition of primidone and its metabolites in epileptic subjects after single and repeated administration.

This neglected the idiopathic syndrome of benign epilepsy of childhood with centrotemporal spikes, and therefore the 1985 (3) and 1989 (1) revisions applied idiopathic and symptomatic to the focal epilepsies as well. The term cryptogenic was added in the 1989 (1) classification to describe epilepsy syndromes that are presumed to be symptomatic but are of unknown cause in specific patients. Discussion of the 1989 Proposal Despite its widespread use, the 1989 proposal has been criticized because of its stiff separation between "partial" and "generalized" epilepsies neglecting multiregional epilepsies and other conditions on the borderline between generalized and focal epilepsies. Furthermore the terms "idiopathic," "cryptogenic," and "symptomatic" have frequently been misunderstood and were thought to be imprecise. Additionally, this system did not accommodate the rapidly growing knowledge in the field and did not differentiate between "wellaccepted" and "controversial" syndromes (9,10). Additionally, the system accommodated didactic grouping purposes but was not helpful in clinical practice: a working diagnosis is usually assigned first and subsequently etiologies are explored. A final diagnosis and classification was frequently not possible before workup was completed. Additionally, the system did not provide sufficient description of seizure semiology, and mingled seizure semiology and epilepsy type or syndrome and only allowed a strict one-toone relationship between seizure type and epilepsy. Axis 2 was based on a list of accepted epileptic seizure types constructed by the task force. These seizure types were closely related to diagnostic epilepsy entities or indicated underlying mechanisms, pathophysiology, or etiology, or implicated related prognosis and therapy. Axis 3 identified the epilepsy syndrome diagnosis and separated epilepsy syndromes from entities with epileptic seizures. Epilepsy syndromes were divided into "syndromes in development" and fully characterized syndromes (10). Axis 4 delineated the etiology of epilepsies, which included pathologic and genetic causes as well as diseases frequently associated with epilepsy and this list was a work in progress at the time of publication. Axis 5 was incomplete at the time of publication and was intended to include an optional classification of the degree of disability and impairment caused by the epilepsy. The introduction of a multiaxial diagnostic scheme reflected the recognition of epilepsy as a clinical symptom that can manifest with different semiologic seizure types and be intertwined with different etiologies. It also responded to criticism that seizure semiology was not sufficiently emphasized in previous classifications. Furthermore, it addressed the more and more confluent borders between generalized and focal epilepsies. Additionally, it modeled epilepsy syndromes more flexibly by defining "accepted syndromes" versus "syndromes in development. These studies indicate that more patients can be classified as further information becomes available in each case and the more skilled the classifying physician is. This proposal (9) was again based on epilepsy syndromes that appeared in previous classifications. The authors defined an epileptic syndrome as "[a] complex of signs and symptoms that define a unique epilepsy condition" (9). However, after discussion and debate this proposal was again revised 5 years later and another progress report was issued 5 years later (12). Axis 1 described ictal seizure semiology through a standardized glossary of descriptive ictal terminology (11). This terminology was independent of pathophysiological mechanisms, epilepsy focus, or seizure etiology. Subsequently, the group scored epilepsy syndromes listed in the 2001 proposal on a scale from 1 to 3, with 3 being the most clearly and reproducibly defined. The proposal mentioned that this was a very preliminary method and intended to ignite further research and category suggestions or possible cluster analysis of signs and symptoms (12). Based on this proposal epilepsy syndromes could be assigned in up to 70% of cases in a first comparison (17). This uses five dimensions to capture the critical features in patients with epilepsy. Dimensions of the PatientOriented Classification Dimension 1: the Epileptogenic Zone the first dimension characterizes the localization of the epileptogenic zone, as determined by all available clinical information. Classification is recognized as an ongoing interactive process with an increasing degree of precision as additional clinical data become available.
The main division in this classification is into partial seizures and generalized seizures. In the partial seizures the abnormal electrical discharges start in a localized area of the brain. These discharges may remain localized, or they may spread to other parts of the brain and then the seizures become generalized (secondary generalized seizures). In generalized seizures, on the other hand, the seizure is generalized from the onset. The patient himself has no memory of the seizure, except in simple partial seizures and only of the aura of other seizures. If he is not too young, he can inform us about the presence and the nature of an aura. During his lifetime, a patient does not necessarily have only one type of seizure. The type may change over the years, depending on the age and maturation of the brain. Both these groups may develop into generalized seizures, then forming a third group. Simple partial seizures the patient does not lose consciousness, and therefore is able to tell what happened, but the experience may be so strange that he may not be able to express himself properly. The twitching may remain there, or spread up the whole extremity and even become completely generalized. The spreading is called a Jacksonian march (named after Huglings Jackson 1835 - 1911). The sensory seizures have their focus in the post central gyrus (primary sensory cortex). There might be feelings of tingling, pins and needles, cold or heat, or numbness of a limb. Sometimes there may be strange feelings with visual signs, or hearing or smelling sensations. There maybe: a sensation rising from the epigastrium to the throat, palpitations, sweating or flushing. The psychic symptoms may consist of changes in mood, memory, or thought (thinking). There may be distorted perceptions (time, space, or person) or problems with language. These simple partial seizures are usually only recognized as epileptic seizures when they develop into generalized seizures. Complex partial seizures Here the patient has impaired consciousness, there is no complete loss of consciousness, he is slightly aware of what is going on, but he cannot respond to anything, neither can he change his behaviour during an attack. There is an aura, a strange feeling in the stomach rising up to the throat and head, or a sensation of light, smell, sound or taste. Sometimes the seizure occurs with hallucinations or with psychomotor symptoms such as automatisms, automatic movements. These automatisms may become very complex, the patient is able to perform difficult tasks, or travel somewhere, but later not remember having done such a thing. During such an automatism the patient may become aggressive and violent when restrained. There is a slow recovery after a complex partial seizure, with a period of confusion. The beginning is as described above, but they end alike the primary generalized tonic-clonic seizures as described below. They come on suddenly and unexpectedly, and if the patients fall, they may injure themselves. Absence seizures these are short periods of loss of consciousness lasting only a few seconds (not more than half a minute). They are of sudden onset, there are usually no, or only minimal motor manifestations. There is a blank stare, brief upward rotation of the eyes, an interruption of ongoing activity.

Ask simple questions and give child two-step directions-"Pick up the block and put it on the shelf. While looking at pictures, imitate the sounds of pictures and encourage child to make them too, such as the cat says meow, the horn goes beep. Make sure child often sees own name in writing such as on cubby or personal space, on all personal belongings, and on artwork or other creations, if child wishes. In the first few weeks of life, infants will look to parents and caregivers for signals of comfort such as friendly smiles, gazes, and gentle speech patterns. However, at this early age, infants typically do not develop a strong feeling of anxiety in the arms of other adults. In the next few weeks up to about 8 months of age, infants continue to develop bonds with people who are consistent in their lives. Many times young toddlers will show a general level of anxiety and may become worried or hesitant around strangers. It is always important to give the toddlers signals of confidence if they show anxiety. By using consistent communication and calming signals and facial expressions, parents and caregivers will help support children during transitions into new spaces and when around new people. They look to adults in their lives to learn how to respond to situations that are unfamiliar to them. Hold and talk to baby throughout the day during diapering, dressing, and eating routines. As they grow and develop, they gain control over some of their feelings and learn new ways to express them. Enjoys being gently bounced or moved around Communicates being overwhelmed through yawning, fussing, turning away, arching back, and extending arms and legs Smiles and coos to show happiness. Ask for help, take time away from baby, and if you feel the stress may affect your interaction with the baby, put the baby in a safe place. Because babies are fragile, any angry handling or shaking may seriously injure a child. If you believe your child may have colic or sensitivity to foods or stimuli, seek the advice of your pediatrician. Responds to own name Shows preference for certain foods, textures, sounds, and music Young children and their caregivers benefit from a daily routine that includes feeding, playing, changing, and sleeping. As the infant begins eating solid food, the feeding routine becomes an eating event. As the infant grows to toddler age, and begins toilet training, the changing routine becomes toileting time. Infants and toddlers feel secure and loved when routine events follow each other in a predictable order. Routines are times when an adult and baby are interacting and form a relationship. The infant trusts the adult to take care of his needs and when the adult is warm and positive, the infant looks forward to these special one on one times. Parents and caregivers can help the young child relax and enjoy each routine by having the same way of starting and ending each one. The patterns are very important as they directly impact mental and physical development. Some research has shown that lack of sleep in young children can be attributed to issues in brain development as well as some behavior disorders.
Intraventricular monitoring for temporal lobe epilepsy: report on technique and initial results in eight patients. Responses to single pulse electrical stimulation identify epileptogenesis in the human brain in vivo. However, any lesion should not be assumed to be the source of the seizures ("dual pathology"), as some are often incidental. Scenarios When Intracranial Localization May Be Limited Although most cases of extratemporal onset involve difficult intrahemispheric localization, lateralization is occasionally at issue. This is particularly common in seizures arising from the supplementary sensorimotor area, where symptomatology and midline epileptiform discharges indicate mesial frontal onset, but lateralization is unclear in the absence of imaging abnormalities or clinical lateralizing signs (55). When the noninvasive presurgical evaluation does not sufficiently narrow the possibilities for localization, invasive studies may be of limited benefit. Presurgical evaluation strategies in patients with localization-related epilepsy remain variable and controversial. No universal scheme is accepted by all epilepsy surgery centers, and techniques continue to evolve (56). Appreciating the brain coverage, strengths, and weaknesses of each invasive technique will help in this choice. In addition, the risk of invasive techniques varies among surgeons; as with other types of surgical procedures, experience and successful practice are important. Advancement in neuronavigation techniques allows for more accurate placement of the electrodes with less complication rate. Of course, the lowest complication rates can be expected from experienced epilepsy neurosurgeons at high-volume epilepsy surgery centers. The predictive value of intraoperative electrocorticography in resections for limbic epilepsy associated with mesial temporal sclerosis. Significance of spikes recorded on intraoperative electrocorticography in patients with brain tumor and epilepsy. Significance of spikes recorded on electrocorticography in nonlesional medial temporal lobe epilepsy. Results of surgical treatment in patients with bitemporal epileptiform abnormalities. Comparison of combined versus subdural or intracerebral electrodes alone in presurgical focus localization. False lateralization by subdural electrodes in two patients with temporal lobe epilepsy. Combined use of subdural and intracerebral electrodes in preoperative evaluation of epilepsy. Interictal spike detection comparing subdural and depth electrodes during electrocorticography. Tailored resections in occipital lobe epilepsy surgery guided by monitoring with subdural electrodes: characteristics and outcome. Operative results without invasive monitoring in patients with frontal lobe epileptogenic lesions. All physiological and pathological consideration renders it improbable that the lesion has any direct relation with epilepsy. The patient was a 22-year-old man with focal motor seizures as a result of traumatic brain injury from a carriage accident. In the same year, Horsley resected a brain tumor and adjacent cerebral cortex guided by analysis of ictal semiology "in order to prevent, as far as possible, the recurrence of the epilepsy" (4). Initially, most cases reported in the literature were resections in the frontal and parietal regions in close proximity to the motor and sensory cortices. Clinical observations made by Jackson associated "dreamy states" and psychical experience with lesions of the mesial temporal lobe. Penfield confirmed these ictal clinical features when he noticed that patients with complex auditory and visual hallucinations as part of their seizures could have their symptoms elicited by focal stimulation of the temporal neocortex and amygdale (5). Penfield described successful control of seizures when he extended the resection to include the uncus and hippocampus in patients whose anterior and lateral resections did not initially eliminate seizures. Most experts use a classification that combines anatomical, clinical, and neuroimaging criteria into the following clinicopathologic categories: 1. Temporal lobe epilepsy without an identified epileptogenic lesion (termed cryptogenic, nonlesional, and paradoxical). Memory-related symptoms, ranging from a feeling of familiarity or strangeness, to elaborate hallucinations, when the patient may feel that he is taking part in a scene experienced before.
Syndromes
Some patients may experience prominent side effects at concentrations in the lower end of the therapeutic range, while others may be free of complaints despite elevated drug concentrations. Although small decreases may completely alleviate complaints, significant dose alterations may dramatically decrease serum concentrations, leading to a recurrence of seizures. Nausea, vomiting, and epigastric pain are often improved by dividing the dose or taking it with meals (or both). In general, however, effects appear modest when serum concentrations are kept within standard therapeutic ranges and polypharmacy is avoided (158,159). Unfortunately, patients taking phenytoin may suffer from cognitive side effects even when these guidelines are followed (160). In one study, phenytoin appeared to be associated with more cognitive effects than carbamazepine, although reanalysis excluding patients with elevated phenytoin concentrations showed no difference (161,168). When used as prophylaxis against seizures following head trauma, phenytoin demonstrated negative cognitive effects compared with placebo (169). No clinically significant difference in cognitive effects between phenytoin and valproate was detected in either healthy adults (170) or patients following craniotomy (140). In one study of elderly patients, phenytoin and valproic acid had similar effects (171), whereas a second study reported no cognitive impairment resulting from modest increases in serum phenytoin concentrations (between 11 g/mL and 16 g/mL) (172). Fluctuations in phenytoin serum concentrations by as much as 50% had no or an immeasurably small effect in children with well-controlled seizures receiving monotherapy with low therapeutic dosages (175). Removal of chronic phenytoin in patients receiving polypharmacy resulted in significant improvement in one test of concentration and two tests of psychomotor function (162). Prophylaxis For seizure prophylaxis in pregnancy-induced hypertension, phenytoin has similar (135) or inferior (136,137) efficacy to magnesium sulfate. Patients receiving phenytoin had more rapid cervical dilation, a smaller decrease in hematocrit after delivery, and a lower incidence of hot flushes (138). In addition, phenytoin did not confound the computer analysis of fetal heart rate (139). Phenytoin is often used following neurosurgical procedures and cerebrovascular accidents. A randomized, double-blind trial compared the efficacy, tolerability, and impact on quality of life and cognitive functioning of anticonvulsant prophylaxis with phenytoin versus valproate in 100 patients following craniotomy (140). No major betweentreatment differences emerged in efficacy, tolerability, impact on quality of life, or cognitive functioning (140). A doubleblind comparison of phenytoin or carbamazepine with no treatment after supratentorial craniotomy noted no significant differences but a higher incidence of side effects in the treated group (141). Thus, prophylactic anticonvulsants cannot be recommended routinely after this type of procedure. The efficacy of phenytoin in the prevention of posttraumatic seizures was studied in a randomized, double-blind trial of 404 patients with serious head trauma (142). Patients received a phenytoin-loading dose within 24 hours of injury; free phenytoin serum levels were maintained in a range from 0. From the time of drug loading to day 7, significantly fewer seizures occurred in the phenytoin group than in the placebo group (3. No benefit was seen in the phenytoin group after day 8, however, leading to the conclusion that phenytoin had an early suppressive effect, but not a true prophylactic effect, on seizures, and that it reduced the incidence of seizures only during the first week after injury. In a secondary analysis of this study (143), no significant difference in mortality was found between patients assigned to phenytoin and those assigned to placebo (143). In a randomized, double-blind, placebo-controlled trial in children with moderate to severe blunt head injury, phenytoin did not prevent posttraumatic seizures within 48 hours of the trauma (144).

Buttner 1992; Feldman and Bolino 2000; Good and others 2006; Liles 1974 (cited in Vasumathi and others 2003); Mazurana and others 2014; and Savoca and Rosenheck 2000. Ambiguity, insecurity, uncertainty; and financial, career, family, social and environmental risks; exposure to Unpredictability/risk trauma. There are stressors related to the business environment, such as increased competition, insufficient time or space, technological development, conflicting demands from stakeholders, and so on. In addition, there are some typical operational stressors, such as cash flow management, recruiting and retaining staff, meeting targets, coping with red tape, worklifebalance, and so on. All of these stressors have been shown to increase job stress and anxiety (Ahmad and Salim 2009; Edwards 1992; Hall and Savery 1986; Robertson 2004; and Rythonen and Strandvik 2005). Broadly speaking, entrepreneurs suffer from three key rolerelated stressors: role conflict, role ambiguity, and role overload (Tahir 2016). Role conflict arises when there is a discrepancy in role expectations between the entrepreneur and others (Kahn and others 1964). Role ambiguity stems from a lack of clarity regarding desired expectations, and is intensified by a lack of skills, experience, and information (Tahir 2016). Finally, role overload occurs when entrepreneurs lack sufficient resources to meet the expected commitments and obligations associated with their role (Latack 1981). Uncertainties in the external environment - which may also be perceived by entrepreneurs to be outside of their control - can also create stressors that impact their ability to function within their business environment. This includes, among others, factors such as natural disasters, largescale migration, and violent conflict. Across studies, these have been linked to higher stress and anxiety (although not specifically tested with entrepreneurs), as well as general unpredictability and risk that affect functionality and the work of the entrepreneurs (Grant and Ferris 2017; and Tahir 2016). Studies have shown that waraffected households and individuals tend to have less diversified livelihood sources, assets, wealth, and wages (Good and others 2006; Mazurana and others 2014; and Savoca and Rosenheck 2000). In Uganda, the total losses for households directly exposed to violence amounted to 10 percent, whereas the total losses from perceived risk amounted to 37 percent (Rockmore 2016). Although the literature is scant when it comes to the impact of trauma on entrepreneurs and business performance, the link between trauma and stress, and its subsequent effect on livelihoods is wellestablished. They recognized the impacts of these symptoms on their productivity and sense of wellbeing, which in turn lead to a vicious cycle of more stress. Box 2 describes the experiences of these entrepreneurs and perceived stressors in their own words. Due to conflict in the region, people report being in a state of fear for their safety. Security issues have also resulted in unfavorable economic conditions for doing business, thereby impeding the chances of success in any business, including the ability to repay loans. Work related stressors spill over into their personal spaces, affecting the tranquility of family life. In their words: "Due to the fear (of bomb blasts/terrorism) people do not want to invest in the expansion of their businesses. When the (work) pressure increases (challenges and stakes are high), the person gives up saying that I cannot do business any more. This requires a better understanding of how to increase the psychological (cognitive and behavioral) capacities of entrepreneurs working in these regions so that they can deal with the increasing number of challenges while persisting in growing their businesses. Since stress depletes psychological resources, the next section will examine strategies to (re)build psychological capital to mitigate such stress. As part of this effort, the study will identify and evaluate the various interventions and training curricula that have been tried and tested in the field of psychology through rigorous impact evaluations. Strategies to (Re)Build Psychological Capital for Stress Mitigation Psychologically healthy, thriving entrepreneurs not only benefit themselves. As stress depletes psychological resources, a key question becomes how to rebuild these capabilities. One way to think about it is to view it from the lens of an entrepreneur, that is, through different "types of capital".
Over the past few years, there have been increasing reports in the use of radiosurgery or Gamma Knife to perform a corpus callosotomy, as reported by both Feichtinger et al. Complications Complications unique to corpus callosotomy as a surgical procedure are neuropsychological in nature. Well-described acute and chronic neuropsychological sequelae are possible after callosotomy (47,48). This syndrome is characterized by a lethargic, apathetic mutism during the first few days after surgery. In our experience and in the experience of other investigators, this is always transient. The predictors of this transient state are related to the extent of callosal sectioning, baseline cognitive impairments, and the amount of traction necessary to gain access to the corpus callosum. The chronic disconnection syndrome was initially not well recognized when callosotomy was initially described (1). Detailed neuropsychological testing reveals deficits that are common after callosotomy, but are not usually clinically significant. The majority of the neuropsychological alterations, other than mutism, occur with posterior callosotomy. This is caused by disruption of communication between visual and tactile cortical sensory functions and verbal expression. Because of the disconnection between the hemispheres, an object placed only in the left visual field of a left-hemispheredominant patient will be seen by the right hemisphere, but the information will not be transferred to the left hemisphere for speech production. Similarly, an object placed in the left hand, but not seen, may be recognized by its shape and size but it will not be named. This is interesting but not clinically disabling to the patient because objects are normally seen by both hemispheres and can be felt with either hand. If a patient has bilateral speech representation, dysphasia may be a postoperative complication. This should be considered before complete callosotomy is undertaken on a patient with mixed speech dominance. Once an unencumbered view of the intrahemispheric fissure is obtained, the medial aspect of the exposed frontal lobe is covered with moist cottonoids, and self-retaining retractors are gently advanced. An error that is sometimes made is to mistake this view of the adherent cingulate gyri for the corpus callosum. The cingulated gyri are separated under magnification in the midline, exposing the corpus callosum and the pericallosal arteries. Once this view is obtained and the retractors are set, a final check of the anterior exposure confirms the exposure of the anterior corpus callosum if the genu is visible. The actual division of the anterior corpus callosum is done with a microdissection instrument and gentle suction. At this level, certain landmarks, such as the cavum of the septum pellucidum, are visible beneath the corpus callosum, even if it is only a potential space in the individual patient. This midline landmark is valuable, if found, because it confirms the complete transection of the callosal fibers and it allows one to stay out of the lateral ventricles. If the lateral ventricle is entered, intraoperative or postoperative bleeding may cause hydrocephalus. The transection is then carried forward into the genu and the rostrum of the corpus callosum. The disconnection is carried out downwards following the A2 branches as they approach the anterior communicating artery complex. Some surgeons advise a simple one-half callosal sectioning, which can be measured by comparing the intraoperative transection to the length of the callosum on the 988 Part V: Epilepsy Surgery A disturbing complication known as alien hand syndrome has been reported (48). In this syndrome, poor cooperation or even antagonistic behavior between the left and right hand is noted. The verbal dominant hemisphere may express displeasure with the actions of the ipsilateral extremities. This phenomenon is usually short lived and is usually seen only in the immediate postoperative period; however, on rare occasions it may persist. Initially, performing only an anterior callosotomy can minimize the likelihood and the extent of these neuropsychological sequelae.
Midazolam is metabolized rapidly by -hydroxylation of the methyl group on the fused imidazo ring. This metabolite is biologically active, but is eliminated with a half-life of about 1 hour after hepatic conjugation with glucuronic acid (293). Midazolam syrup has been associated with respiratory depression and arrest, and should only be given where resuscitative drugs, equipment, and experienced personnel are immediately available. Paradoxical reactions (agitation, tremor, involuntary movements, hyperactivity, and combativeness) occur in about 2%, seizures and nystagmus in about 1%. Hypotension and decreased cardiac output likely result from peripheral vasodilatation (283). Sudden discontinuation after long-term use can result in withdrawal seizures (295). Phenytoin and carbamazepine reduce the bioavailability of oral midazolam by inducing cytochrome P450, which enhances first-pass hepatic metabolism (297). Midazolam was tolerated well by neonates, with no change in pulse or blood pressure and no adverse reactions. Intranasal midazolam was rapidly effective (175,309), and parents preferred it over rectal diazepam due to faster action and the ability to give it in public (175). The time to end of seizure was not different between groups, and no cardiorespiratory adverse events occurred. Intrabuccal and intranasal midazolam are thus viable routes of administration in this patient population. Midazolam suppresses respiratory drive, so patients must be entubated and mechanically ventilated. Tolerance may develop, and doses up to 2 mg/kg/hr have been required for seizure control (298). In a similar series of 20 children (mean age 4 years), midazolam was well tolerated and stopped seizures in 95% of patients (305). Clonazepam is 81% to 98% absorbed after oral administration, with peak plasma levels occurring in 1 to 4 hours (6). It is highly lipid soluble with somewhat lower plasma protein binding (86%) than diazepam (124). Clonazepam is primarily metabolized to an inactive product, 7-amino-clonazepam, which is conjugated to glucuronide and excreted by the kidneys (6). Plasma half-lives were similar in single and multiple-dose studies, with Chapter 55: Benzodiazepines 679 ranges of 18. Adverse Effects and Drug Interactions Drowsiness and lethargy occur in about 50% of adult patients initially, but tolerance to these symptoms develops with continued administration (311). Drowsiness was seen in up to 85% of children treated with clonazepam and, along with other side effects, necessitated termination of the drug in 27% of patients (6). Nystagmus is fairly common; incoordination, ataxia, hypotonia, dysarthria, and dizziness are less frequent. Behavior disturbances including aggression, hyperactivity, and paranoia can be seen in up to 12% of children (312). Increased salivary and bronchial secretions, anorexia, or hyperphagia can also occur. A "burning mouth syndrome" with painful oral dysesthesias has been described (315). Other conditions reported to respond to clonazepam include hyperekplexia (330), acute intermittent porphyria (331), epilepsy with continuous spike-and-wave during slow-wave sleep (332), and neonatal seizures (333). Its role in epilepsy is limited to adjunctive therapy of refractory generalized or partial seizure disorders, particularly in the setting of comorbid anxiety disorders. Dissolving clonazepam into a droplet of propylene glycol followed by buccal administration achieved therapeutic levels in 10 to 15 minutes, and might be a strategy for treating serial seizures (319). Good control of absence seizures was obtained at plasma levels of 13 to 72 ng/mL (317).
References:




