There being a lack of motor function expressed in the structures holding the kidney in situe, a relaxation of these structures is permitted, thus allowing the kidney to be displaced. The adipose tissue in which the kidney is imbedded is absorbed and the renal vessels are this condition most frequently occurs in lean elongated. If the movability is great there is a dragging pain in the lumbar region or deeply in the abdomen. Occasionally there is severe coliky abdominal the pain, with nausea, vomiting and extreme prostration. If this congestion occurs in the arteries it is called active congestion, the vessel congestion. This begins with a tired, aching pain over the kidneys which intensifies after a time and radiates diagonally across the abdomen following the course of the the bladder is very irureters to the bladder and groin. An abnormal condition in which there is the is retention of certain excretory substances, part of which urea, within the body. The most common, however, is acute or chronic nephritis in which there is an excess of urea retained in the blood, because of the inability of the kidney to excrete it. The characteristic renal pallor soon appears, the skin becomes dry and has a urinary odor. The patient has occipital or vertical headache, irritability of temper, nausea and vomiting, itching of the skin, and finally uremic convulsions cation, may first supervene. Occasionally these convulsions may be the They vary in form, symptom often closely simulating the convulsion of epilepsy, but in most cases have a fever of 103 to 106 degrees. The convulsion may consist of a single paroxysm, during which time the muscles are in a tonic spasm, or there may be a series of muscular contractions, the entire attack lasting several hours. Consciousness may be affected in various degrees, but, as a rule, the^ fever case has coma, especially following the convulsion. The urine will always show the presence of albumin, and a simple test for albumin will often confirm the analysis when the other prominent symptoms to attract the attention. Uremic coma differs from apoplectic coma in that there the absence of hemiplegia, no conjugate deviation of the eyes, pupils not unequal, and no high arterial tension in is uremia. The inflammation usually effects the urinThe vessels become hyperemic, the lining becomes swollen, the kidney is enlarged, and the cortex is a deep red color. Exudation of serum, fibrin, blood cells and debris into the tubules forms casts and fills up the lumen of the tubules. The edema usually first seen beneath the eyelids and about the ankles, but soon spreads to the entire body, developing into general dropsy or anasarca. The abdomen becomes distended, the diaphragm is pressed upward, thus interfering with respiration, and necessitates the patient assuming the erect position. There is usually slight or moderate fever, nausea and vomiting, pain over the kidneys, dry, harsh skin, with a urinary odor, and a rapid, full pulse. Pathologically this is known as the large white kidney, often becoming twice the normal size; it is smooTn aricl of a whitish-yellow color. There be a proliferation of the connective tissue cells, with a resulting thickening of the interstitial tissue. Upon the thickening of the connective tissue it contracts and diminishes the size of the kidney. There is suppression of urine, more gradual than in the acute form, which gradually leads to the uremic symptoms. The dropsy increases, interfering with respiration so that the may have to constantly assume an erect posture, even while sleeping. The dropsy will be most noticeable in the parts of the body that are in the lowest level that is, if the patient should lie upon the right side, the right arm, leg and right side of the face and body will be swollen, while the opposite side may show but slight signs of edema. Anemia becomes pronounced from the loss of albumin and patient; the retention of urine in the blood. This usually affects both kidneys; they becoming inflamed, the vessels of the connective tissue becoming hyperemic, and the connective tissue cells proliferating and contracting.
The paucity of cavitation distinguishes acute blastomycosis from histoplasmosis and tuberculosis. Chronic disease can develop in the upper lobes, with cavities and fibronodular infiltrations similar to those seen in tuberculosis, but unlike in tuberculosis or histoplasmosis, these lesions rarely caseate or calcify. General Considerations the causative fungus, Blastomyces dermatitidis, is found in soil primarily in the Mississippi and Ohio River valleys, additional southeastern and south central states, and the states bordering the Great Lakes. Differential Diagnosis Primary pulmonary infection resembles acute viral, bacterial, or mycoplasmal infections. Blastomycosis should be considered when a significant pulmonary infection in an endemic area fails to respond to antibiotic therapy. Patients with diabetes mellitus are especially prone to superficial Candida infection; thrush and vaginitis are most common. Candida is the third most common blood isolate in hospitals in the United States and is a common cause of catheter-related urinary tract infection. Treatment Mild pulmonary blastomycosis does not require treatment; indeed, it is rarely recognized. Surgical debridement is required for devitalized bone, drainage of large abscesses, and pulmonary lesions not responding to medical therapy. Mongkolrattanothai K et al: Urine antigen detection of blastomycosis in pediatric patients. Oral candidiasis (thrush)-Adherent creamy white plaques on the buccal, gingival, or lingual mucosa are seen. Lesions may be few and asymptomatic, or they may be extensive, extending into the esophagus. Thrush is very common in otherwise normal infants in the first weeks of life; it may last weeks despite topical therapy. Spontaneous thrush in older children is unusual unless they have recently received antimicrobials. Angular cheilitis is the name given to painful erythematous fissures caused by Candida at the corners of the mouth, often in association with a vitamin or iron deficiency. Vaginal infection-Vulvovaginitis occurs in sexually active girls, in diabetic patients, and in girls receiving antibiotics. Pronounced erythema with a sharply defined margin and satellite lesions is typical. Congenital skin lesions-These lesions may be seen in infants born to women with Candida amnionitis. Dissemination may occur in premature infants, or in term infants after prolonged rupture of membranes. Scattered red papules or nodules-Such findings may represent cutaneous dissemination. Paronychia and onychomycosis-These conditions occur in immunocompetent children but are often associated with immunosuppression, hypoparathyroidism, or adrenal insufficiency (Candida endocrinopathy syndrome). The selective absence of specific T-cell responses to Candida can lead to marked, chronic skin and nail infections called chronic mucocutaneous candidiasis. In immunosuppressed individuals: systemic infections (renal, hepatic, splenic, pulmonary, or cerebral abscesses); cotton-wool retinal lesions; cutaneous nodules. In either patient population: budding yeast and pseudohyphae are seen in biopsy specimens, body fluids, or scrapings of lesions; positive culture. Speciation is important because of differences in pathogenicity and response to azole therapy. C albicans is ubiquitous and often present in small numbers on skin, mucous membranes, or in the intestinal tract. Normal bacterial flora, intact epithelial barriers, neutrophils and macrophages in conjunction with antibody and complement, and normal lymphocyte function by skin test reactivity are factors in preventing invasion. Chronic draining otitis media-This problem may occur in patients who have received multiple courses of antibiotics and are superinfected with Candida.

If the effused blood remains in the air sacs, signs of consolidation will be present, but this blood is usually removed by expectoration or absorption. Embolism is an obstruction of a blood vessel, carried to the point of obstruction by the blood stream. Emboli most frequently consists of destroyed epithelium or endothelium from the valves of the heart folDefinition. If a medium-sized vessel is obstructed there will be cough, dyspnoea, cyanosis, blood-streaked expectoration, and, possibly, hemoptysis. There is extreme mental anxiety, depression of spirits, syncope, and, possibly, coma or convulsions. This begins with a capillary bronchitis, in which the mucous membrane lining the terminal bronchioles becomes hyperaemic and swollen. This extends to the alveoli and air cells with which the bronchiole communicates, which is followed by exudation, so that there is soon noticed multiple areas is of consolidation less over both lungs. This exudate more or purulent in character, and consists of mucus, desquamated epithelium and leucocytes. It may be mixed with blood, which slowly oozes from the dilated capillaries, giving to it a reddish color. The onset may be gradual, with pleurisy pains around the region of the nipple, axilla or scapula with short, jerky respirations and a gradual rise in the bodily; temperature. Other cases may begin more abruptly, with a chill and rapid rise in the temperature. The pulse is rapid, the breathing is is rapid, shallow and jerky, and is there tical, all slight cyanosis. The respiratory movement ver- as the respiration is of the superior costal type, and accessory muscles of respiration are brought into play. The cough is very loose at first and the expectoration is abundant, but as the air cells become conA solidated and incapable of containing air it lessens. About 75 per cent of pneumonia found in children is bronchQzpjieumonia, and in those cases cerebral symptoms are marked, the most common being the fever delirium, but there may be stupor and coma. Broncho-pneumonia differs from less bronchitis, in that the fever of the latter is slight, the rales are large and of the mucous variety, the dyspnoea is areas of consolidation are absent and the exmarked, pectoration is very profuse. In lobar pneumonia the area of consolidation is circum- scribed and unilateral, while in broncho-pneumonia the areas of consolidation are multiple and scattered on both sides. Lobar pneumonia has a sudden onset, and terminates by crisis in less than two weeks. The inflammation of the connective tissue produces a hyperaemia of its blood vessels, a swelling of the tissue" which, becomes permanent because of the proliferation of the connective tissue cells adding to its bulk, a loss of its elasticity and a final stretching of the air cells. During the early stages the most pronounced symptom is cough, which is dry and irritated by Dyspnoea soon becomes dust, cold air, and upon exertion. In the advanced stages there is retraction of the respiratory muscles of the affected side, and thus decreased expansion upon that side. The ribs on the affected side approximate each other, the shoulder droops and there^is a curvature of thgjspine in theupper dorsal region. The concavity of the cuTvature is toward the affectecfside, whilejtscpnvexity is toward thejslevated shoulder of the unaffected side. The is greatly increased in size, the intercostal spaces on this side are wide and the ribs run more horizonThere is usually a compensatory pmphyscma of the tally. Expectorate is colored by dust from various materials, dependent upon the occupation of the patient. The symptoms are those of chronic bronwith cough, labored breathing, deficient expansion on the affected side, deformity of the thorax, as in fibroid pneumonia, and profuse expectoration. This may be very variable, as any condition preventing the passage of air into the alveoli of the lung will produce atelectasis. Among these may be mentioned obstruction of the bronchi by consolidation by pressure from without, such as tumor of ^he mediastinum, aneurisnuif. Most frequently the upper portion of the lungs are and are of a pale red color with thin vesicular walls. The dilatation of the walls is so great in many cases that the interalveolar septa is torn and the capillaries destroyed, so the affected portion of the lung lacks normal blood supply and is dry. The resistance offered to the pulmonary circulaaffected, tion may be so great as to effect right ventricular hyper- trophy] Symptoms.
Asabsorptionviatheoral routeisvariable,threedosesareneededoverthefirst 4 weeks of life to achieve adequate liver storage. Vitamin K should be given to all newborn infants to prevent haemorrhagic disease of the newborn. If the hip is dislocatable, the femoral head will be pushed posteriorly out of the acetabulum(Fig. Ligamentousclicks withoutanymovementoftheheadoffemurareofno 152 Biochemical screening (Guthrie test) Biochemical screening is performed on every baby. Newborn hearing screening is performed on all infants to detect severe hearing impairment. Screeningforcysticfibrosisisperformedbymeasuring the serum immunoreactive trypsin, which is raised if there is pancreatic duct obstruction. Further reading Lissauer T, Fanaroff A: Neonatology at a Glance, ed 2, Oxford, 2011, Blackwell. If it is anticipated during pregnancy that the infant is likely to require longterm intensive care or surgery, it is preferable for the transfer to the (a) Neonatal mortality by birthweight 800 Neonatal mortality rate <1500g 600 400 200 0 50 55 60 65 70 75 80 85 90 95 00 05 19 19 19 19 19 19 19 19 19 19 20 20 (b) Causes of neonatal deaths Infection 5% Other specific causes 4% Congenital anomaly 23% 1500-1999g 2000-2499g 10 Immaturity 57% Year Figure 10. When a baby requirestransferpostnatally,transportshouldbebyan experienced team of doctors and nurses. Com promised cardiac output diminishes tissue perfusion, causing hypoxicischaemic injury to the brain and other organs. Theneuronaldamagemaybeimmediatefromprimary neuronal death or may be delayed from reperfusion injury causing secondary neuronal death. Although hypoxicischaemic injury usually occurs antenatally or during labour or delivery, it may occur postnatallyorbecausedbyaneonatalcondition. Injuries may also occur during manual manoeuvres, from forceps blades or at Ventouse deliveries. Nerve palsies Brachial nerve palsy results from traction to the bra chial plexus nerve roots. Humerus/femur Usually midshaft, occurring at breech deliveries, or fractureofthehumerusatshoulderdystocia. Surfactantdeficiency is rare at term but may occur in infants of diabetic mothers. Thetermhyalinemembranediseasederives from a proteinaceous exudate seen in the airways on histology. Glucocorticoids, given antenatally to the mother, stimulate fetal surfactant production and are givenifpretermdeliveryisanticipated(seeCh. The rate and severity of problems associated with prematurity decline markedly with increasing gesta tion. Central venous line for parenteral nutrition, if indicated Insertedperipherallywheninfantisstable. Chest X-ray with or without abdominal X-ray Assistsinthediagnosisofrespiratorydisordersandto confirmthepositionofthetrachealtubeandcentral lines. Minimal handling All procedures, especially painful ones, adversely affectoxygenationandthecirculation.
Department of Orthopedics and Ilizarov Unit, Alessandro Manzoni Hospital, Lecco, Italy. It is a considerable surgical challenge, especially when associated with extensive skin and soft tissue damage. Amputation was the only solution in the past, but current limb-salvage options include contralateral or ipsilateral microvascularized or free-fibular transfer. We report seven patients with massive tibial bone loss treated by gradual medial transport of the ipsilateral fibula using an Ilizarov traction apparatus with olive wires after proximal and distal fibular osteotomies. This method has the advantages of avoiding surgery on the contralateral limb while allowing early weightbearing because of the stability of the Ilizarov frame. Hypertrophy of the transported fibula accompanied by full weightbearing and satisfactory joint motion occurred in all patients. All patients were satisfied with the results, and none thought amputation would have been a better treatment. We think the Ilizarov frame for ipsilateral fibular gradual transport is a reasonable alternative for limb salvage in patients with massive tibial bone loss. The objective of this study was to evaluate the use of indirect reduction with Ilizarov external fixation as a viable alternative in the surgical treatment of certain calcaneal fractures. A limited percutaneous plantar skin incision was used to improve reduction of the posterior facet. The average score increased to 74 for patients with more than 10 months followup and to 77 for patients with isolated calcaneal fractures. Open fractures also had early debridement and soft-tissue coverage; no deep infections were seen in this subgroup. There were 11 complications, including nine superficial pin track infections, one superficial skin necrosis under an area of fracture blister, and one deep infection in a diabetic smoker with severe hemorrhagic fracture blisters. All superficial infections responded to local pin or wound care and oral antibiotics. No secondary reconstructive procedures, including osteotomies, subtalar fusions, or amputations, have been done. Particularly favorable results were obtained in open fractures when soft-tissue reconstruction also was done. Advantages include shorter time to surgery, immediate weightbearing, minimal invasiveness, few serious wound problems, and no residual hardware. Disadvantages include technical difficulty, incomplete reduction of fracture fragments, and the need for secondary surgery (fixator removal). Management of complex tibial and femoral nonunion using the Ilizarov technique, and its cost implications. Of these, we classified 41 in 40 patients as complex cases because of infection (22), bone loss (6) or failed previous surgery (13). Using the Association for the Study and Application of the Methods of Ilizarov scoring system we obtained 17 excellent, 14 good, four fair and six poor bone results. The functional results were excellent in 14 patients, good in 14, fair in two and poor in two. A total of six patients were lost to follow-up and two had amputations so were not evaluated for final functional assessment. The average cost of treatment to the treating hospital was approximately pound 30,000 per patient. We suggest that early referral to a tertiary centre could reduce the morbidity and prolonged time off work for these patients. The results justify the expense, but the National Health Service needs to make financial provision for the reconstruction of this type of complex nonunion. Department of Plastic and Reconstructive Surgery, Chaim Sheba Medical Center, Israel. This article discusses the treatment of recurrent flexion-contracture of the knee after circumferential burns involving the entire limb. A two-team approach to surgery is used: the orthopedic team widely excises the scar tissue and releases tendons, muscles, and adjacent soft tissue that limit joint movement. The microsurgery team covers the exposed popliteal neurovascular elements with a latissimus dorsi free flap.
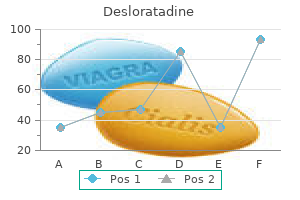
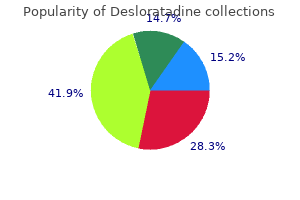
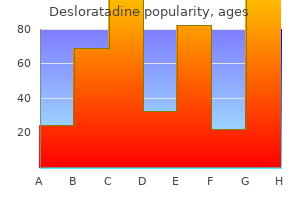
Silica (Silicon). Desloratadine.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97042
Psychosocial support Thediagnosisofapotentiallyfatalillnesshasanenor mous and longlasting impact on the whole family. Theyneedtheopportunitytodiscusstheimplications of the diagnosis and its treatment and their anxiety, fear, guilt and sadness. Most will benefit from the counselling and practical support provided by health professionals. Help with practical issues, including transport, finances, accommodation and care of siblings, is an early priority. Thechildrenthem selves, and their siblings, need an ageappropriate explanation of the disease. Clinical symptoms and signs result from disseminated disease and systemic illhealth from infiltration of the bone marrow or other organs with leukaemic blast cells. In most children, leu kaemia presents insidiously over several weeks (see Case History 21. Chest X ray is required to identify a mediastinal mass characteristic of Tcell disease. Remission induction Beforestartingtreatmentofthedisease,anaemiamay require correction with blood transfusion, the risk of bleeding minimised by transfusion of platelets, and infection must be treated. Additional hydration and allopurinol(orurateoxidasewhenthewhitecellcount ishighandtheriskisgreater)aregiventoprotectrenal function against the effects of rapid cell lysis. Remis sion implies eradication of the leukaemic blasts and restorationofnormalmarrowfunction. Bone marrow examination is essential toconfirmthediagnosisandtoidentifyimmunological and cytogenetic characteristics which give useful Signs and symptoms of acute leukaemia General Malaise, anorexia Anaemia Bone marrow infiltration Neutropenia Thrombocytopenia Pallor, lethargy Infection Bruising, petechiae, nose bleeds Bone pain Hepatosplenomegaly Reticulo-endothelial infiltration Lymphadenopathy Superior mediastinal obstruction (uncommon) Central nervous system Other organ infiltration* Testes *Rare at diagnosis, more often at relapse Headaches, vomiting, nerve palsies Testicular enlargement Figure 21. Examination showed pallor, petechiae, modest generalised lymphadenopathy and mild hepatosplenomegaly. Brain tumours In contrast to adults, brain tumours in children are almostalwaysprimaryand60%areinfratentorial. The use of radiotherapy and/or chemotherapyvarieswithtumourtypeandtheageof thepatient. Clinical features Signs and symptoms are often related to evidence of raisedintracranialpressurebutfocalneurologicalsigns maybedetecteddependingonthesiteofthetumour (seebelow). Late effects the functional implications of the site of the tumour, the potential hazards of surgery and the importance of radiotherapy in treatment all combine to place childrenwithbraintumoursatparticularriskofneuro logical disability and of growth, endocrine, neuro psychological and educational problems. Magnetic resonance spectroscopy can be used to examine the biological activity of a tumour. Management Surgery is usually the first treatment and is aimed at treating hydrocephalus, providing a tissue diagnosis andattemptingmaximumresection. Even tumours Hodgkin lymphoma Clinical features Classically presents with painless lymphadenopathy, most frequently in the neck. Investigations Lymph node biopsy, radiological assessment of all nodal sites and bone marrow biopsy is used to stage diseaseanddeterminetreatment. Tcell malignancies may present as acute lympho blastic leukaemia or nonHodgkin lymphoma, with both being characterised by a mediastinal mass with varyingdegreesofbonemarrowinfiltration. Bcell malignancies present more commonly as nonHodgkin lymphoma, with localised lymph node disease usually in the head and neck or abdomen.
The pathology of spastic spinal paralysis is the same as that of lateral sclerosis, and when affecting adults is is usually considered the same. At the onset the patient complains of a feeling of tiredness and stiffness in the legs with some aching pain in the back. The muscles become weak and stiff so that In infants the onset may be with the spastic gait develops^ a convulsion, after which the child does not appear to be itself. As a rule it does not learn to walk, dentition is deThe arms and layed, and the child may not learn to speak. In all cases the legs are jtiff, the knees drawn close together, the legs are moved stiffly and with hesitation, and the toes drag" and catch on the ground. This disease usually affects the posterior lateral columns, and begins with chronic inflammation, in~~which the vessels of the cord become hyperemic, the white substance becomes swollen, the neuroglia becomes thickened, pressing upon the nerve substance and replacing it. This may begin in one tract and later appear in other parts, as can be determined by the symptoms. If the degeneration lies in the cervical part of the cord the arms will be affected in a similar manner as the legs. There is diarrhoea of the bowels, ankle clonus, ataxic gait, and a paraplegia involving both the motor and sensory functions. Meningitis could be caused by a local subluxation anywhere in the spine, but is not so common as that produced by the atlas. There is no definite nerve-tracing in meningitis, on account of the abnormal condition lying within the neural canal, but tenderness is extreme and diffuse along the spine. The meninges become inflamed and and over-filled swollen, their blood vessels are dilated with blood, and there is an exudation into the neural canal and into the intermeningeal spaces, which produces pressure upon the cord and is responsible for many of the symptoms that arise. The onset is with severe spinal pain, which radiates along the course of the spinal nerve s over the trunk and jegs. Myperaesthesia is very marked along the spine, r and is general in its distribution. Clonic spasms of various groups of muscles are present, and in the more"severe cases there is a partial paralysis, usually in the form of a paraThe muscles affected are stiff, and become atroplegia. During the course of the meningitis, and especially early, there is fever of 100 to 102 degrees, with gastric and intestinal disturbances, scanty and highly-colored urine, coated tongue, and general weakness. An the thin membranes acute inflammation or excessive heat of of the spinal cord, affecting the pia and the arachnoid membranes. As in the external form, this is caused by an atlas or axis subluxation interfering with the flow of calorific impulses and producing excessive heat. Exudation occurs from the membrane into the intermeningeal spaces and If the pressure at the presses upon the cord substance. Since the pia mater is nearer to the cord than the dura, there is a greater degree of paralysis and less this pain in leptomengitis than in external meningitis. The muscles finally become atrophied but may remain spastic, the sensory function may be dulled, and the patient is left in a state of paralysis which pursues a chronic course. As its name implies, is an inflammation of membranes surrounding the brain, accompanied with an Also known as exudative meningitis. The atlas or axis subluxation causes the in- flammation or excessive heat in the meninges of the brain. Excessive heat is characterized by swelling of the membranes, hyperemia of the bipod vessels and exudation of serum. In cerebral meningitis this effusion is large and presses upon the brain, producing many cerebral symptoms. This begins with a severe headache, spinal pain, chill, and a fever varying from 102 to 105 degrees. With the rise in the temperature the cereBmTsymptom^are manifest, and consist principally of a low muttering delirium". There is cutaneous hyperaesthesia over the entire legs, There is cervical retraction, stiff. The blood pressure is usually the local subluxation reduces the amount of motor high. The brain substance being soft, is easily displaced and pressed upon by the clot, which renders the part functionless, and produces a motor paralysis of all parts of the body supplied by nerves arising from the affected portion of the brajn. Hemorrhage of the brain most frequently occurs from the middle cerebral artery or its branches.
These traditional "recipes" are considered the best ways, and sometimes they are, but they are also often considered the only ways, which is one reason why circus acts tend to look so much alike. The radio and television star Arthur Godfrey, after doing a show at Sea Life Park, invited me to visit him and his wife at their farm in Virginia to watch the horse training. Godfrey was an excellent rider and trainer himself and owned a number of performing horses. We were watching a horse being trained to bow, or kneel on one knee, by a traditional method involving two men and a lot of ropes and whips; the horse under this method is repeatedly forced onto one knee until it learns to go down voluntarily. If there were another way to train a bow, he would know about it-that we had to walk him around the outside of the barn two or three times to cool him off. In a more formal situation, however-in giving a lesson, say, or in shaping behavior in an animal-the trainer should keep his or her attention on the training subject or the class until the training period is over. This is more than just good manners or good self-discipline; it is skilled training. When a subject essays to earn reinforcers, it enters into a contract, so to speak, with the trainer. If the trainer starts chatting to some bystander or leaves to answer the telephone or is merely daydreaming, the contract is broken; reinforcement is unavailable through no fault of the trainee. This does more harm than just putting the trainer at risk of missing a good opportunity to reinforce. Of course if you want to rebuke a subject, removing your attention is a good way to do it. Picking up the fish bucket and walking away for one minute is one of the few ways one has of saying "No! Sometimes outside circumstances will temporarily eradicate a well-learned behavior-when stage fright, for instance, makes it impossible to give the thoroughly memorized speech, or a bad fall severely affects your rock-climbing skills. Sometimes subsequent learning overlies or contradicts the original learning, so that mix-ups occur-you strive for the Spanish word and come up with the German. Sometimes the side effects of punishment or other aversive events interfere with unrelated behavior. Attorney and dog fancier Morgan Spector describes an obedience trial in which every single dog that competed shied away from one particular corner of the ring. Sometimes an apparently well-trained behavior just breaks down, and you never will identify the reason. Your high-scoring competition obedience dog who has never done such a thing before in his life gets up in the middle of the three-minute Long Sit exercise and wanders out of the ring. At Sea Life Park we called this "going back to kindergarten," and the technique often brought a poor behavior up to par in ten or fifteen minutes. Of course we are doing just this whenever we review for an exam or refresh our memories by glancing at a script before going onstage. It is useful to remember that if you can more or less match the original shaping process, reviewing works equally well for physical as for mental skills. Cats often seem to get restless after perhaps a dozen reinforcers, so five minutes might be plenty. Human lessons of many sorts are traditionally an hour long, and football practice, graduate seminars, and various other endeavors often go on all day. This is true for whole sessions, but it also applies to stages within a session, when you stop working on one behavior and go on to another. You should move on on a high note-that is, as soon as some progress has been achieved. The last behavior that was accomplished is the one that will be remembered best; you want to be sure it was a good, reinforceable performance. What happens all too often is that we get three or four good responses-the dog retrieves beautifully, the diver does a one-and-a-half for the first time, the singer gets a difficult passage right-and we are so excited that we want to see it again or to do it again. So we repeat it, or try to , and pretty soon the subject is tired, the behavior gets worse, mistakes crop up, corrections and yelling take place, and we just blew a training session. I detest watching people practice jumping their horses; so often they go past the point when they should have stopped, when the animal was doing well and before the behavior began falling apart. But you may find that in the next session the retrieve, the somersault dive, the solo obbligato is not only as good as the last one of the previous session but noticeably better. At the start of the next session, the performance may actually begin a step beyond where it left off, and then you have just that much more to reinforce. It can produce not only steady progress but absolutely error-free training, and this can go extremely fast; I once halter-broke a pony yearling in fifteen minutes, from start to finish, and permanently, by moving back and forth between five shaping tasks (forward, stop, left, right, and back) while reinforcing progress in each one.
References:




