Major Symptoms of I-Cell Disease A child aged 5 months was referred to a specialist. He had been suffering repeated upper respiratory tract infections and did not seem to be developing his motor abilities, Clinical examination revealed hyperplasia of the gums, restriction of joint mobility and hepatosplenomegaly. Examination of the fibroblasts under the microscope revealed the presence of numerous intracellular inclusions, which on electron microscopy were revealed to be large lysosomes. It has a somewhat unique primary structure in that much of its length is composed of a repeating tripeptide Gly-X-Y-Gly-X-Yetc. Three pro- chains assemble to form a triple helical structure (procollagen), which can now be transferred to the Golgi. The propeptides are cleaved from the ends of procollagen by proteases to form collagen molecules (also called tropocollagen). Like osteogenesis imperfecta, these syndromes are a result of locus heterogeneity in which defects in several different genes (loci) Behavioral Science/Social Sciences can result in similar symptoms. Characteristic features include thin, translucent skin; arterial, intestinal, or uterine rupture; and easy bruising. There are several important diseases associated with defective collagen production. Disorders of Collagen Biosynthesis Disease Scurvy Defect Deficient hydroxylation secondary to ascorbate deficiency Mutations in collagen genes Mutations in collagen genes and proline and lysyl hydroxylases Major Symptoms Petechiae, ecchymoses Loose teeth, bleeding gums Poor wound healing Poor bone development Skeletal deformities Fractures, blue sclera Hyperextensible, fragile skin Hypermobile joints, dislocations, varicose veins, ecchymoses, arterial, intestinal ruptures Depigmented (steely) hair Arterial tortuosity, rupture Cerebral degeneration Osteoporosis, anemia Osteogenesis imperfecta Ehlers-Danlos syndromes Menkes disease Deficient cross-linking secondary to functional copper deficiency Recall Question Vitreous humor is formed from which type of collagen A blood test showed that the infant had low serum ceruloplasmin and only 10% of normal serum copper levels. Common with Ehlers-Danlos diseases, Menkes disease has a symptomology due, in part, to weak collagen. Copper can be absorbed into the mucosal cell, but it cannot be transported into the bloodstream. Consequently, an affected individual will have severe copper deficiency and all copper-requiring enzymes will be adversely affected. Lysyl oxidase requires copper and plays a direct role in collagen formation by catalyzing the cross-linking of collagen fibrils. A deficiency in the activity of this enzyme and other copper-dependent enzymes would be directly responsible for the described symptoms in this infant. For each mutation described in the questions below, choose the most closely related sequence change in the options above. A nasopharyngeal swab obtained from a 4-month-old infant with rhinitis and paroxysmal coughing tested positive upon culture for Bordetella pertussis. A 25-month-old Caucasian girl has coarse facial features and gingival hyperplasia and, at 2 months of age, began developing multiple, progressive symptoms of mental retardation, joint contractures, hepatomegaly, and cardiomegaly. Levels of lysosomal enzymes are elevated in her serum, and fibroblasts show phase-dense inclusions in the cytoplasm. Which of the following enzyme deficiencies is most consistent with these observations Parahemophilia is an autosomal recessive bleeding disorder characterized by a reduced plasma concentration of the Factor V blood coagulation protein. Deficiency arises from a 12 base-pair deletion in the Factor V gene that impairs the secretion of Factor V by hepatocytes and results in an abnormal accumulation of immunoreactive Factor V antigen in the cytoplasm. Collagen, the most abundant protein in the human body, is present in varying amounts in many tissues. If one wished to compare the collagen content of several tissues, one could measure their content of A. A 6-month-old infant is seen in the emergency room with a fractured rib and subdural hematoma. Respiratory tract infections caused by Pseudomonas aeruginosa are associated with the secretion of exotoxin A by this organism.
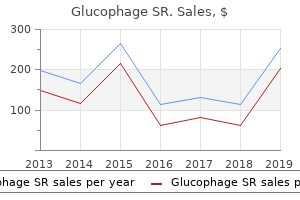
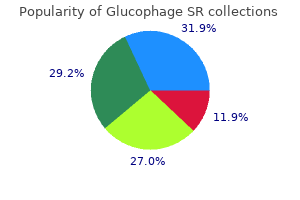
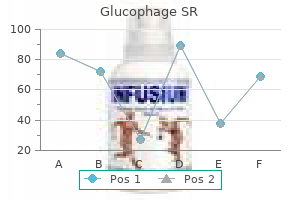
D-Alpha-Tocopheryl (Vitamin E). Glucophage SR.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96917
Among those diagnosed with hypersomnia, the prevalence of a psychiatric disorder is somewhat higher-46. The reasons behind the comorbidity of sleep and psychiatric disorders are not well understood. Comorbidity might be due to one disorder being a risk factor or cause of the other; they might both be manifestations of the same or overlapping physiological disturbance; one might be a consequence of the other. In generalized anxiety disorder, for example, the symptoms of fatigue and irritability used to diagnose it are often the result of a sleep disturbance, which itself is also a diagnostic symptom. Adolescents with major depressive disorders report higher rates of sleep problems and, conversely, those with sleep difficulties report increased negative mood or mood regulation (Ryan et al. In addition, sleep-onset abnormalities during adolescence have been associated with an increased risk of depression in later life (Rao et al. The best studied and most prevalent comorbidity is insomnia with major depression. On the basis of longitudinal studies, insomnia is now established as a risk factor for major depression. Not all people with insomnia have a depression diagnosis; however, studies have found that 15 to 20 percent of people diagnosed with insomnia have major depression (Ford and Kamerow, 1989; Breslau et al. A variety of polysomnographic abnormalities have been found with other psychiatric disorders (Benca, 2005a). Most potential mechanisms for sleep changes in psychiatric disorders deal specifically with insomnia and depression. Possible mechanisms include neurotransmitter imbalance (cholinergicaminergic imbalance), circadian phase advance, and hypothalamic-pituitaryadrenal axis dysregulation (Benca, 2005a). Recent evidence implicating regions of the frontal lobe has emerged from imaging studies using positron emission tomography. Because the amygdala also plays a role in sleep regulation (Jones, 2005), this finding suggests that sleep and mood disorders may be manifestations of dysregulation in overlapping neurocircuits. The authors hypothesize that increased metabolism in emotional pathways with depression may increase emotional arousal and thereby adversely affect sleep (Nofzinger et al. Treatment Comorbid psychiatric and sleep disorders are treated by a combination of medication and/or psychotherapy (Krahn, 2005; Benca, 2005a). A major problem is underdiagnosis and undertreatment of one or both of the comorbid disorders. One of the disorders may be missed or may be mistakenly dismissed as a condition that will recede once the other is treated. In the case of depression, for example, sleep abnormalities may continue once the depression episode has remitted (Fava, 2004). If untreated, residual insomnia is a risk factor for depression recurrence (Reynolds et al. Further, because sleep and psychiatric disorders, by themselves, are disabling, the treatment of the comorbidity may reduce needless disability. Insomnia, for example, worsens outcomes in depression, schizophrenia, and alcohol dependence. Another concern is that medication for one disorder might exacerbate the other. Insomnia and Psychiatric Disorders As mentioned above insomnia is associated with depression, acting as both a risk factor and a manifestation (Ford and Kamerow, 1989; Livingston et al. Several studies done were longitudinal in design, including one that tracked more than 1,000 male physicians for 40 years (Chang et al. Another study, which followed 1,007 young adults at a health maintenance organization for 3. This figure is based on 16 percent of the sample who developed depression with a history of insomnia at baseline, as compared with 4. Insomnia is also a predictor of acute suicide among patients with mood disorders (Fawcett et al. The striking association between insomnia and depression in so many studies suggests that insomnia is also an early marker for the onset of depression, and the two may be linked by a common pathophysiology. Although the pathophysiological relationship is not known, researchers are focusing on overlapping neural pathways for anxiety, arousal, and/or circadian disturbance (Benca, 2005b).
Both animals also had the same black discoloration of the glandular stomach as those in the control group. A low incidence of alopecia and emaciation was observed in control and exposed animals. The mean absolute weights of the heart, liver, and spleen from male mice exposed to 80 ppm (111 mg/m3) H2S were significantly depressed. In addition, the mean absolute kidney weight of 80 ppm (111 mg/m3) female mice was also significantly reduced by approximately 20%. However, relative weights were not significantly different and clinical pathology and histology were negative in both sexes. Histological examination of surviving animals revealed the nasal tract as the only site where lesions were considered compound-related. The lesion was primarily located in the squamous portion of the nasal mucosa but extended into the respiratory type epithelium (ciliated) in some animals. In one female, the lesion was suppurative -2222 and severe involving the entire nasal passage and associated structures. The lesion was also observed in two 80 ppm (111 mg/m3) mice that were exposed in extremis. This effect was present in male (8/9) and female (7/9) animals exposed to 80 ppm (111 mg/m3) H2S. The lesions, judged as minimal to mild in severity, were localized primarily in the squamous portion of the nasal mucosa but extended to regions of ciliated respiratory-type epithelium. Following a 90-day exposure period in rats, 10 males and females from each group were selected for clinical pathology and histology, while the remaining 5 males and females from each group were used for special neuropathologic studies. In the neuropathologic studies, rats were anesthetized with sodium pentobarbital containing 200 units of heparin. Rats were perfused via the left ventricle with a 4% phosphate buffered glutaraldehyde solution. On the following day, the right and left sciatic nerves and the cervical and lumbar portions of the spinal cord were dissected and placed in 4% glutaraldehyde. The left sural nerve and large muscle branch of the tibial nerve were oscimated and placed in cedarwood oil for two weeks. Nerve fibers in the oil were teased and individual fibers mounted to glass slides. After staining, specimens were examined by light microscopy for pathological changes. Body weights were significantly reduced from weeks 1 to 13 in males and females exposed to 80 ppm (111 mg/m3) H2S. No abnormalities in ophthalmology, neurological function, serum chemistry, or urinalysis were reported. Sulfhemoglobin levels were significantly increased in males exposed to 80 ppm (111 mg/m3) H2S. Although elevated sulfhemoglobin levels were also observed in females exposed to 30. The investigators state that assigning biological significance to the sulfhemoglobin values should be done with caution because of sensitivity of the method and the size of the groups investigated. Also, there were no H2S-related lesions in animals selected for special neuropathologic studies. Organ weights were statistically similar between control and exposure weights except for the relative brain weight of males exposed to 80 ppm -2323 (111 mg/m3) H2S. Relative, but not absolute, brain weights were significantly increased in these animals. Minimal multifocal peribronchial lymphocytic infiltrate was observed in the lungs of all rats. None of the histopathologic changes were considered treatment-related by the investigators. In the Sprague-Dawley rats, 15 males and 15 females per group, no mortality was observed during the 90-day study. Statistically significant decreases in body weights were observed in males exposed to 80 ppm (111 mg/m3) H2S during weeks 1 through 3, and in 80 ppm-treated females exposed throughout the 90-day study. Feed consumption was also significantly depressed in males and females exposed to 80 ppm (111 mg/m3) H2S.
Headache is the most commonly found symptom associated with brain tumors and is found in approximately half of cases. Patients with brain metastasis that present with seizures should be started on anticonvulsant therapy in addition to dexamethasone. In this particular case there is associated midline shift that warrants immediate medical management. Melanoma is an exception, being consistently hyperintense on T1-weighted images and hypointense on T2-weighted images. Patients that present with new onset headaches, personality changes, and mood disorders need to be evaluated for brain tumors. See cerebral contusion conductive hearing loss, 434 congenital toxoplasmosis, 265 constipation and amyotrophic lateral sclerosis, 354 and dysautonomia, 231 460 constipation (Cont. See binocular diplopia; monocular diplopia; vertical diplopia dipyridamole, for secondary stroke prevention, 99 divalproex (Depakote), for migraine headaches, 157 Dix-Hallpike test, 311, 313 dizziness, 310 from anticonvulsant therapy, 132 from beta-blockers, 21, 158, 159 defined, 310 from facial paralysis, 294 from postconcussive syndrome, 90 from pseudomotor cerebri, 279 vs. See sixth nerve palsy ischemic stroke causes, 97 diagnostic evaluation, 98 etiologies, 98 vs. See also brain tumors, metastatic; cerebellopontine angle tumors; pseudotumor cerebri syndrome epidermoid tumor, 434 glomus tumor, 434 of parotid/skull base, 294 Tzanck smear, 292, 293 U unreactive pupil, 257. See arboviruses; Arenaviruses; Eastern equine encephalitis virus; human herpesvirus 6; La Crosse virus; retroviruses; St. Preface the nervous system and the muscles are the seat of many primary diseases and are affected secondarily by many others. This pocket atlas is intended as an aid to the detection and diagnosis of the symptoms and signs of neurological disease. The text and illustrations are printed on facing pages, to facilitate learning of the points presented in each. Chapter 2 concerns the functions of the nervous system and the commonly encountered syndromes in clinical neurology. The clinical neurological examination is best understood once the material of the first three chapters is mastered; it is therefore presented in the last chapter, Chapter 4. The choice of topics for discussion is directed toward questions that frequently arise in clinical practice. Some of the illustrations have been reproduced from previous works by other authors, because they seemed to us to be optimal solutions to the problem of visually depicting a difficult subject. In particular, we would like to pay tribute here to the graphic originality of the late Dr. Our colleagues at the Sanderbusch Neurological Clinic were always ready to help us face the difficult task of getting the book written while meeting the constant demands of patient care.

Other Syndromes the methods of diagnosing fetal alcohol syndrome arise from the larger fields of teratology and dysmorphology (clinical genetics). It is essential to remember that many birth defect syndromes share isolated features, but each is differentiated by a unique constellation of features. Comprehensive assessments lead to accurate diagnoses and informed intervention plans. Although space has been provided to record a full complement of data, we are not implying that all of these assessments must be conducted to derive a diagnosis. It is the responsibility of the clinical team to select the most appropriate assessment battery for each patient. The form also serves as a centralized data repository for efficient generation of the final medical report and is designed to facilitate data entry into a database. The New Patient Information Form completed by the caregivers prior to the diagnostic evaluation (Appendix 2). Medical/psychological/educational assessments conducted prior to the diagnostic evaluation. Assessments administered by the clinical team at the time of the diagnostic evaluation. The caregiver/patient interview conducted at the time of the diagnostic evaluation 2. Diagnosis of fetal alcohol spectrum disorders by a multidisciplinary team of professionals (physician, psychologist, speech-language pathologist, occupation therapist, etc. All team members participate in the derivation of the 4-Digit Code and intervention plan. Type of Score Other Test/Subtest Names Score Age (yr/mos) or Date Other Test/Subtest Names Score 0 1 2 3 Academic Achievement. Depression, etc) Disorder Age (yr/mos) or Date Diagnosed Disorder Age (yr/mos) or Date Diagnosed Disorder Age (yr/mos) or Date Diagnosed Medication. If yes, source of confirmation: Reported use of alcohol during this pregnancy is: Other information about alcohol use during this pregnancy unknown unknown unknown Reliable Somewhat reliable Unk. Birth order if child is the result of a multiple birth pregnancy: of Prenatal care: Yes, (If yes, when did it start Other conditions of heritability or malformation that may be relevant to this case. Abuse: Physical Sexual Number of home placements Other. Medical Issues B. Each 4-Digit Diagnostic Code falls into one of 22 unique Clinical Diagnostic Categories (labeled A through V). A list of the 4-Digit Diagnostic Codes, which fall within each Clinical Diagnostic Category, is presented in Section V. The following terms are used in varying combinations to name the 22 diagnostic categories. These include a unique cluster of minor facial anomalies (short palpebral fissures, thin upper lip, and a smooth philtrum) and growth deficiency. Other physical findings (major or minor anomalies) may be detected instead of or in addition to these sentinel findings that may suggest alternate or additional conditions. There are places on the Diagnostic Form to record and interpret other physical findings. Static Encephalopathy: the term "encephalopathy" refers to "any significant abnormal condition of the structure or function of brain tissues" (Anderson, 2002). The term "static" means that the abnormality in the brain is unchanging; neither progressing nor regressing. The term does not define or suggest any specific pattern of structural, neurological, or functional abnormality. Neurobehavioral Disorder: the term "Neurobehavioral Disorder" is used in this diagnostic system when the patient presents with cognitive/behavioral dysfunction at the Rank 2 level and no evidence of structural, neurological or functional abnormalities at the Rank 3 or Rank 4 levels. Alcohol (Exposed, Not Exposed, Exposure Unknown): these terms are used to reflect prenatal alcohol exposure and its potential risk to the unborn child. Alcohol exposure is reported independently of outcome(s) and does not imply that a causal association exists between the exposure and the outcome(s). Given the fact that variable presentation is the rule rather than the exception after teratogenic exposures, we felt it was appropriate to establish this diagnostic category.
The dose should be reduced if these symptoms occur, and it should be discontinued if symptoms are severe or worsening. Valproic acid and divalproex sodium: Hepatotoxicity, including fatalities, have been reported, usually during the first 6 months of treatment. There is an increased risk of valproateinduced acute liver failure and resultant deaths in patients with mitochondrial disease. Valproate should not be given to a woman of childbearing potential unless the drug is essential to the management of her medical condition, and women should use effective contraception while using valproate. Patients and guardians should be warned that abdominal pain, nausea, vomiting, and/or anorexia can be symptoms of pancreatitis that require prompt medical evaluation. In some cases, vigabatrin may also damage the central retina and may decrease visual acuity. However, this assessment cannot always prevent vision damage, and once detected, vision loss due to vigabatrin is not reversible. Vigabatrin should be withdrawn from patients who fail to show substantial clinical benefit. Healthcare providers who prescribe vigabatrin and pharmacies that dispense the product must be specially certified. Additionally, some medications are recommended to be titrated during initial treatment. Please refer to the prescribing information of the individual products for more detailed information. For the nasal spray, a second dose may be given 4 hours after the initial dose when required. The product should be used to treat no more than 1 episode every 5 days and no more than 5 episodes per month. Should be used to treat no more than 1 episode every 3 days and no more than 5 episodes per month. Capsules are extendedrelease and may be suitable for once-daily dosing in some adults. Immediate-release tablets are given 2 to 3 times per day and the suspension is given 4 times per day. Delayed-release tablet and capsule doses > 250 mg per day should be given in divided doses. Suspension should be prepared using water only and administered immediately after preparation. Tablets for oral suspension (Spritam) can be dissolved in liquid and swallowed or allowed to disintegrate in the mouth. Perampanel (Fycompa) Pregabalin (Lyrica) Rufinamide (Banzel) Stiripentol (Diacomit) tablets, oral suspension capsules, oral solution tablets, oral suspension oral oral oral once daily at bedtime 2 to 3 times per day 2 times per day Tablets can be administered whole, as half tablets, or crushed. Powder should be mixed with water and taken immediately after mixing during a meal. Capsules should be swallowed whole without chewing to avoid local irritation of the mouth and throat. These products vary in terms of their indications for specific seizure types and indications other than epilepsy. Evidence-based guideline: treatment of painful diabetic neuropathy: report of the American Academy of Neurology, the American Association of Neuromuscular and Electrodiagnostic Medicine, and the American Academy of Physical Medicine and Rehabilitation. Comparative efficacy of antiepileptic drugs for patients with generalized epileptic seizures: systematic review and network meta-analyses. Safety and efficacy of midazolam nasal spray in the outpatient treatment of patients with seizure clusters-a randomized, double-blind, placebo-controlled trial. Practice Parameter: treatment of postherpetic neuralgia: an evidence-based report of the Quality Standards Subcommittee of the American Academy of Neurology. Efficacy and tolerability of the new antiepileptic drugs I: treatment of new-onset epilepsy. Report of the Therapeutics and Technology Assessment Subcommittee and Quality Standards Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Evidence-based guideline: treatment of convulsive status epilepticus in children and adults: report of the Guideline Committee of the American Epilepsy Society.
Syndromes
The inner skull base forms the floor of the cranial cavity, which is divided into anterior, middle, and posterior cranial fossae. The anterior fossa lodges the olfactory tracts and the basal surface of the frontal lobes; the middle fossa, the basal surface of the temporal lobes, hypothalamus, and pituitary gland; the posterior fossa, the cerebellum, pons, and medulla. The anterior and middle fossae are demarcated from each other laterally by the posterior edge of the (lesser) wing of the sphenoid bone, and medially by the jugum sphenoidale. The middle and posterior fossae are demarcated from each other laterally by the upper rim of the petrous pyramid, and medially by the dorsum sellae. Skull Viscerocranium the viscerocranium comprises the bones of the orbit, nose, and paranasal sinuses. The superior margin of the orbit is formed by the frontal bone, its inferior margin by the maxilla and zygomatic bone. The frontal sinus lies superior to the roof of the orbit, the maxillary sinus inferior to its floor. The nasal cavity extends from the anterior openings of the nose (nostrils) to its posterior openings (choanae) and communicates with the paranasal sinuses-maxillary, frontal, sphenoid, and ethmoid. The infraorbital canal, which transmits the infraorbital vessels and nerve, is located in the superior (orbital) wall of the maxillary sinus. The portion of the sphenoid bone covering the sphenoid sinus forms, on its outer surface, the bony margins of the optic canals, prechiasmatic sulci, and pituitary fossa. Skull 5 Temporomandibular joint Argo light Argo Meninges the meninges lie immediately deep to the inner surface of the skull and constitute the membranous covering of the brain. The pericranium of the inner surface of the skull and the dura mater are collectively termed the pachymeninges, while the pia mater and arachnoid membrane are the leptomeninges. Pain can thus be felt in response to noxious stimulation of the dura mater, while the cerebral parenchyma is insensitive. Some of the cranial nerves, and some of the blood vessels that supply the brain, traverse the dura at a distance from their entry into the skull, and thereby possess an intracranial extradural segment, of a characteristic length for each structure. Thus the rootlets of the trigeminal nerve, for instance, can be approached surgically without incising the dura mater. Pachymeninges the pericranium contains the meningeal arteries, which supply both the dura mater and the bone marrow of the cranial vault. The pericranium is fused to the dura mater, except where they separate to form the dural venous sinuses. The virtual space between the pericranium and the dura mater-the epidural space-may be forced apart by a pathological process, such as an epidural hematoma. Immediately beneath the dura mater, but not fused to it, is the arachnoid membrane; the intervening virtual space-the subdural space-contains capillaries and transmits bridging veins, which, if injured, can give rise to a subdural hematoma. The falx cerebri separates the two cerebral hemispheres and is bordered above and below by the superior and inferior sagittal sinuses. It attaches anteriorly to the crista galli, and bifurcates posteriorly to form the tentorium cerebelli, with the straight sinus occupying the space between the falx and the two halves of the tentorium. The much smaller falx cerebelli separates the two cerebellar hemispheres; it encloses the occipital sinus and is attached posteriorly to the occipital bone. The tentorium cerebelli separates the superior aspect of the cerebellum from the inferior aspect of the occipital lobe. The opening between the two halves of the tentorium, known as the tentorial notch or incisura, is traversed by the midbrain; the medial edge of the tentorium is adjacent to the midbrain on either side. The tentorium attaches posteriorly to the sulcus of the transverse sinus, laterally to the superior rim of the pyramid of the temporal bone, and anteriorly to the anterior and posterior clinoid processes. The tentorium divides the cranial cavity into the supratentorial and infratentorial spaces. The pituitary stalk, or infundibulum, accompanied by its enveloping arachnoid membrane, Meninges Pia Mater the cranial pia mater is closely apposed to the brain surface and follows all of its gyri and sulci. The cerebral blood vessels enter the brain from its surface by perforating the pia mater. Except for the capillaries, all such vessels are accompanied for a short distance by a pial sheath, and thereafter by a glial membrane that separates them from the neuropil.
It is important to note that because only one search term was used, this search was not as thorough as the search performed for somnology and somnopathy R01 grants. Therefore, it may represent a significant under representation of the asthma field. In 2004, Harvard University, the University of Pennsylvania, and the University of Pittsburgh received 46 percent of sleep-related career development awards. Further, although many sleep disorders disproportionately affect minorities (Rosen et al. In 2004, only 15 percent of all investigators with an R01 identified themselves as belonging to a minority ethnicity (Asian, African American, Hispanic, Pacific Islander, or other) (personal communication, M. As minority clinicians and investigators are more likely to work in underserved areas (Urbina et al. Barriers to Sleep Research Career Development Barriers to attracting, training, and sustaining a critical mass of sleep investigators include the poor awareness among the general public and health care professionals and the availability of appropriate mentors to provide scientific and career guidance to new investigators. Exciting basic science research and the dissemination of this excitement to a broad group of potential trainees are necessary and potentially ratelimiting steps in attracting new investigators from a limited pool of individuals committed to academic careers. Therefore, although there have been some remarkable successes in scientific investigation aimed at elucidating fundamental sleep physiology and biology. Fundamental scientific discoveries play critical roles in galvanizing interest in any scientific discipline. Recruiting and retaining trainees in somnology and sleep medicine competes with other more established fields, many of which have made highly publicized advances, enjoy widespread respect across medical centers, and are more established as an academic discipline. Investigators, particularly new ones who commit to interdisciplinary sleep-related research, are challenged to prove their value in academic medical centers that are accustomed to recognizing and rewarding individuals with "departmentally" defined research foci. Resource allocation needed to support new investigators may require complex negotiations among academic departments, which may deter new investigators or otherwise limit their access to needed support. In addition, identification of optimal mentoring relationships, critical for career development, will likely require sustained relationships among individuals with competing institutional commitments. Increasing fiscal pressures and, for physicians, demands to spend more time on clinical services, are threats to protected time critical for career development. New investigators are also often burdened with substantial debt from school loans, providing disincentives to participate in prolonged postdoctorate training. Programs have been developed with the aims of attracting new trainees and developing the research and academic skills, and supporting their transition to independent and externally funded investigators (K01, K02, K08, K23, and K25). National Research Service Award Institutional Training Grants (T32) provide institutions with funds to support the training of individual postdoctoral candidates. To limit the number of grants that were not relevant to somnology or sleep disorders, the committee included only grants in which the key words appeared in both the thesaurus terms and the abstract and not the abstract alone. Analysis of the number of sleep-related T and F awards shows an increase between 2000 and 2004 (Figure 7-2). However, the number of K awards decreased over the same time period and a larger proportion went to a smaller group of academic institutions. Three institutions, Harvard University, University of Pennsylvania, and University of Pittsburgh, accounted for 27 percent of all sleep-related T, K, and F grants received in 2000, 35 percent in 2004. The same three institutions received 29 percent of all K awards in 2000, and 46 percent in 2004. This may reflect the extensive development of these programs and concentration of senior investigators. In general, for any given award category, with few exceptions no more than one new career development award was granted in any given year between 2000 and 2004. Since 2000, investment in career development awards for clinical scientists, K08 and K23, has varied. Although there has been greater investment in the K23 series, it is still minimal with five new awards in 2003 by four different institutes. There has also been very limited investment in the K07 academic career awards, designed to improve curricula and emphasize development of scientist leadership skills. Apart from the Sleep Academic Award program, there has been very little investment through the K07 mechanism, no new awards were granted in 2003, and only three in 2004.
Rather, there have been diagnostic guidelines that physicians have been encouraged to follow, but the guidelines have not been sufficiently specific to assure diagnostic accuracy or precision. How many facial features must be present, how severe must the features be, and what scale of measurement should be used to judge the severity There has been a lack of objective, quantitative scales to measure and report the magnitude of expression of key diagnostic features For example, although a thin upper lip and smooth philtrum are key diagnostic features (Astley & Clarren, 1996; Clarren & Smith, 1978; Jones & Smith, 1973; Smith, 1979; Stratton et al. Objective quantitative scales not only improve accuracy and precision, but also establish a common numeric language for communicating outcomes in medical records and in the medical literature. So would an individual whose mother drank a fifth of vodka daily throughout pregnancy and presented with microcephaly, severe mental retardation, growth deficiency and no facial anomalies. New diagnostic terms that more finely differentiate the variable exposures and outcomes of individual patients, without implying alcohol as the sole causal agent, are needed. Features such as microcephaly, neurological abnormalities, attention deficit, mental retardation, and growth deficiency frequently occur in individuals with prenatal alcohol exposure, and frequently occur in individuals with no prenatal alcohol exposure. The 4-Digit Code also requires that all other adverse prenatal and postnatal exposures and events be documented for they too serve as important risk factors that must be taken into consideration when deriving a diagnosis and intervention plan. Accurate surveillance is vital for setting public health policy and assessing the effectiveness of primary prevention efforts. The 4-Digit Code requires that data be collected not just to support the diagnosis, but to derive the diagnosis. Meeting the Diagnostic Challenge Each of the above limitations has been largely overcome with the development of the "4-Digit Diagnostic Code". Greatly increases diagnostic precision and accuracy through the use of objective, quantitative measurement scales, image analysis software, and specific case definitions. Offers an intuitively logical numeric approach to reporting outcomes and exposure that reflects the true diversity and continuum of disability associated with prenatal alcohol exposure. Documents the presence of prenatal alcohol exposure without judging its causal role. Documents all other prenatal and postnatal adverse exposures and events that can also impact outcome. Provides a quantitative measurement and reporting system that can be used independent of diagnostic nomenclature. Can be taught to a wide array of health care and social service providers, thus greatly expanding the availability of diagnostic services. While this document might at first appear overly complex and perhaps daunting, one will find that this diagnostic approach is logical and easy to use, and will greatly facilitate the proper description and classification of patients presenting with all possible combinations of outcomes and exposures. These are subsequently named to reflect the Likert ranking of each digit in the 4Digit Diagnostic Code. For example, a code of 3243 is the Diagnostic Category called "Sentinel physical finding(s) / static encephalopathy (alcohol exposed)". Ultimately, establishing terms that are both clinically accurate, broadly applicable, and facilitate access to services remains a challenge. It is important to remember that the 4-Digit Code provides a numeric measurement and reporting system for exposures and outcomes that can be used independently of the proposed diagnostic nomenclature. When either feature receives a rank of 3 or 4, Sentinel physical finding(s) is placed at the beginning of the name. When alcohol exposure receives a Rank 3 or 4, (alcohol exposed) is placed at the end of the name. When alcohol exposure receives a Rank 2, (alcohol exposure unknown) is placed at the end of the name. A code of 1222 would receive the clinical name Neurobehavioral disorder (alcohol exposure unknown). Subsequent pages in the Medical Summary Note should document the findings and recommendations specific to the patient. We are looking for growth deficiency characteristic of a teratogenic insult, not characteristic of postnatal environmental factors such as nutritional deprivation or chronic or acute illness. In contrast, growth deficiency due to postnatal environmental influences is likely to present as periodic fluctuations in the curve. Postnatal growth (all measures collected after birth) Select the part of the growth record with the greatest deficiency in the height percentile.
To ensure its provider network can provide physical access, reasonable accommodation, and accessible equipment for Enrollees with physical or mental disabilities. To acknowledge and agree that the following sanctions take effect immediately and are not subject to stay during the pendency of an appeal: a. To comply with the pharmacy choice requirements established by House Bill 759 (2019). To specify that, at the time of this Agreement, the prevalent nonEnglish languages spoken by Enrollees and potential Enrollees in the State are as follows: a. Disqualification from future participation in the Maryland Medicaid Managed Care Program; and f. That the term of this Agreement shall begin on January 1, 2020 and terminate on December 31, 2020. Completion or termination of the Section 1115 Research and Demonstration Waiver and Federal funding thereunder; b. Notification by the Maryland Department of Budget and Management that State funds are not available for the continuation of the HealthChoice Program; c. That any change in Federal or State law or regulation that affects any provision or term of this Agreement shall automatically become a provision or term of this Agreement. That a notice required to be given to the other party under this Agreement, unless specified otherwise, is effective only if the notice is provided in writing and sent by first-class mail, courier or delivery service, or electronic transmittal of original documents with signatures, to the representative and address for that party listed below: a. Notices to the Department shall be sent to: Jill Spector Director, Medical Benefits Management Administration Maryland Department of Health 201 W. Covered Entity and Business Associate shall collectively be known herein as the "Parties. Business Associate may, if directed to do so in writing by Covered Entity, create a limited data set as defined at 45 C. Any such limited data sets shall omit any of the identifying information listed in 45 C. Business Associate will report any material breach or violation of the data use agreement to Covered Entity immediately after it becomes aware of any such material breach or violation. Business Associate agrees to use appropriate safeguards, and comply with Subpart C of 45 C. Is made to Covered Entity without unreasonable delay and in no case later than fifteen (15) calendar days after the incident constituting the Breach is first known, except where a law enforcement official determines that a notification would impede a criminal investigation or cause damage to national security. A brief description of what happened, including the date of the Breach and the date of the discovery of the Breach, if known; 2. Any steps the affected Individuals should take to protect themselves from potential harm resulting from the Breach; 4. A brief description of what the Business Associate is doing to investigate the Breach, to mitigate losses, and to protect against any further Breaches; and Rev. Contact procedures for the affected Individuals to ask questions or learn additional information, which shall include a toll-free telephone number, an e-mail address, website, or postal address. In the event the event the Breach occurs through the fault of Business Associate, Business Associate shall be responsible for notifying Individuals by sending via First Class U. In the event the Breach occurs through the fault of Covered Entity, Covered Entity shall be responsible for notifying Individuals no later than 60 calendar days after Covered Entity receives notice of the Breach from the Business Associate. To the extent permitted by the Underlying Agreement, Business Associate may use agents and subcontractors. Part 164, comply with the requirements of Subpart E that apply to the Covered Entity in the performance of such obligation(s); M. Provide an opportunity for Business Associate to cure the breach or end the violation and, if Business Associate does not cure the breach or end the violation within the time specified by Covered Entity, terminate this Agreement; or Immediately terminate this Agreement if Business Associate has breached a material term of this Agreement and Covered Entity determines or reasonably believes that cure is not possible. The obligations of Business Associate under this Section shall survive the termination of this agreement. Any ambiguity in this Agreement shall be resolved to permit Covered Entity to comply with the Privacy and Security Rules. The Business Associate or Subcontractor is acting as an independent contractor and not as the agent of the Covered Entity or Business Associate. This Agreement does not give the Covered Entity or Business Associate such control over operational activities so as to make the Rev.
References:




