Models can use genomic surveillance data to detect evolutionary changes during the outbreak that could indicate further adaptation to new host species (animal or human) or vectors, which could portend more extensive transmission. Few models attempt to predict the time and place of an outbreak beforehand, but retrospective studies of outbreak precursors have identified possible precipitating factors, and a broad class of models attempts to identify settings that could be conducive to disease emergence or spread (Box 2). Operationally useful models have been developed for some climatesensitive diseases, such as those transmitted by arthropod vectors whose abundance and behavior are tightly linked with temperature, precipitation, vegetation patterns, and other aspects of weather or the environment. For zoonotic diseases, studies in areas of disease emergence that identify wildlife or domestic animal species, the microbes they carry, and animal or human behaviors that could promote spillover have been especially revealing. These models are based on the biology of the specific pest and match the pest biology with climate and host characteristics to support plant pest detection activities. These pests can attack numerous host species, some (such as the old world bollworm) with hundreds of plant host species, including row crops (such as wheat, corn and cotton), vegetables (like peppers and tomatoes), and fruit crops (strawberries and stone fruits). Modelers drew on diverse data sources to generate insights into these uncertainties during the recent Ebola outbreak in West Africa, the current Zika outbreak in the Americas, and non human disease outbreaks in the United States, such as highly pathogenic avian influenza, white nose syndrome in bats, and sudden oak death. Ebola: When the West Africa Ebola outbreak gained international attention in March 2014, initial reports warned that it was already spiraling out of control, but data collection and reporting challenges hampered assessment of the situation. Key knowledge gaps included the importance of various transmission settings and the virulence of the outbreak virus strain. Preliminary models incorporated the limited available data to estimate the growth rate of the epidemic and predict its course in the absence of public health intervention. These early forecasts were cited widely in calls for a major international response. Analyses of viral genomic data and epidemiological data suggested that the outbreak had begun with the introduction of a new Ebola virus strain in late 2013, and showed that human travel was propagating the outbreak across urban centers and national borders. As the outbreak continued, detailed mechanistic models tested various possible interventions, and suggested that control could most quickly be achieved with a combination of hospital and communitybased measures, such as safe burial practices and prohibition of eating and serving bushmeat. Models also were used to support planning of anticipated field trials of candidate vaccines against Ebola. Zika: the Zika outbreak in the Americas also spurred a vigorous response by the modeling community, like the 20142016 Ebola outbreak did. As with Ebola, models were used to predict disease burden and 6 Toward Epidemic Prediction: Federal Efforts and Opportunities in Outbreak Modeling international spread and define the genetic lineage of the outbreak virus strain, and contended with knowledge limitations similar to those encountered in the Ebola response. Models also were used to address additional uncertainties around the Zika epidemic. For example, they assessed the risk of international spread associated with the 2016 Summer Olympics in Rio de Janeiro, Brazil; the risk of local transmission by competent mosquito vectors if infected travelers introduce the virus into new areas; the resources needed to screen donated blood for Zika virus; and the risk of birth defects in infants born to women infected during pregnancy. Highly Pathogenic Avian Influenza: In support of the response to the 20142015 outbreak of highly pathogenic avian influenza in the United States, models were developed to simulate disease introduction and spread within U. These models were used to evaluate alternative control strategies for their impact on outbreak severity, duration, and economic consequences, including trade losses. This enabled improvements in surveillance design, planning for business continuity, evaluation of vaccination strategies, resource planning for diagnostic testing, and stockpiling of personal protective equipment and antiviral drugs. Phylogenetic models were used to better understand disease spread and inform efforts to improve biosecurity on farms. FederalEffortsinOutbreakModeling the White House and Federal agencies have recognized the promise of modeling to improve epidemic preparedness and response. The policy foundation for Federal outbreak modeling includes the National Strategy for Pandemic Influenza Implementation Plan (2006), which identified models as "powerful tools that can be used to inform policy decisions by highlighting the impact of various interventions on the spread of disease"; National Strategy for Biosurveillance (2012), which included forecasting as a core function of biosurveillance; and National Biosurveillance Science and Technology Roadmap (2013), which noted that "New modeling and ecological forecasting approaches have the potential to enhance the effectiveness of current strategies for predicting the likelihood of disease outbreaks and determining the likely impacts when a threat is detected. Many of its participating agencies support programs in the area, ranging from foundational research into the ecological and biological factors driving disease emergence to operational modeling that supports decisions during outbreaks (Table 1). Department or agency Examples Department of Agriculture Animal and Plant Health Inspection Service: Foreign animal disease. Plant health modeling to identify potential pathogen niches and to assess spatiotemporal pest introduction risk. Agricultural Research Service: Research and modeling of arthropod vectors of human and animal disease and insect pests of crops. Department of Defense Defense Advanced Research Projects Agency: Modeling zoonotic spillover and predicting transmission of human diseases of military and national security importance.
Syndromes
It is quite likely that there will be constraintsenvironmental, interpersonal, financial, and administrativeon the ways that you can implement the approaches suggested in the Guide. Despite the challenges, your hard work makes a difference in the lives of all the children in the classroom. It is clear, though, that children with Asperger Syndrome may need more help and support than some of your typically developing students. The investment of time and energy in the strategies listed above can pay off tenfoldnot only for the child with Asperger Syndrome, but also for all the young learners in your school community. As you learn more about children with differences and how to support their inclusion in the classroom, you will become a mentor to other educators who may be facing this challenge for the first time. Many of the skills that make you a powerful educator will help you succeed in the tasks ahead of you. Your curiosity will fuel your education about Asperger Syndrome and other disorders on the "I learned a lot from my first experience teaching a child with autism, and it has autism spectrum; your communication benefited not only how I teach students with skills will help you create a meaningful autism, but also how I work with all my alliance with the parents of the child students. These support strategies must be available to the child at all times and in all environments. Presented below are examples of sensory support strategies and fidgets that can be used to address common sensory problem areas for young people with Asperger Syndrome. For a more comprehensive guide to the interpretations of and interventions for sensory-related behaviors, see Asperger Syndrome and Sensory Issues: Practical Solutions for Making Sense of the World. Sensory Support Process Sensory Problem Overly sensitive to touch, movements, sights, or sounds Signs or Behavior Distractible, withdraws when touched, and avoids certain textures, clothes, and foods; reacts negatively to ordinary movement activities, such as playground play or P. Craves intense sensory experiences, such as spinning, falling, or crashing into objects. Poor balance, great difficulty in learning a new task that requires motor coordination; appears awkward, stiff, or clumsy. Impulsive or distractible; shows lack of planning in approach to tasks; does not anticipate results of actions; difficulty adjusting to new situations or following directions; gets frustrated, aggressive, or withdrawn when encountering failure. Under-reactive to sensory stimulation Coordination problems Poor organization of behavior Unusually high/low activity level Poor self-concept Note: Taken from the book, Answers to Questions Teachers Ask About Sensory Integration, by Carol Stock Kranowitz, M. A child with Asperger Syndrome may encounter at least one or more of the following: Examples of Sensory Needs and Supports Sample Sensory Problem Area Caesar has difficulty pouring a glass of water without spilling it. He may have trouble with motor planning related to successfully completing a task. Greta cannot keep her hands and feet to herself during circle time in her preschool classroom. Greta may crave tactile input, in which case she may learn by handling objects, and/or she may fail to understand about personal boundaries. He may like his outfit because of the soft cotton texture and dislike jeans because of the texture or because certain characteristics may be irritating or uncomfortable, like a waistband or the width/length of the leg. She may find this calming or may be seeking oral, tactile, or proprioceptive input. Sample Support Strategy and Fidget Increase the weight of the container and decrease the amount of liquid in it, or fill cups or bowls only partially. Other interventions include rubbing lotion on the child, removing irritating clothing tags, or using a fragrance-free detergent. Provide her with something appropriate to chew on, such as candy, straws, gum, or a sports-type water bottle. A standard set of interventions should not be prescribed for individuals with Asperger Syndrome, as each student will have individual needs. Interventions that provide predictability, support, and empowerment, while also reducing anxiety and building on strengths, are generally effective. Some interventions that merit consideration for young people with Asperger Syndrome include: Priming Classroom assignment accommodations Visual supports Home base Choice making Handwriting modifications Incorporation of special interests Homework considerations these intervention activities are described in more detail on the following pages. Priming is not a time for teaching or reviewing the content of activity, or having the student actually complete the activity. Priming may occur the day before an activity, the morning of it, the class period before, or even at the beginning of the class period when the activity will be completed. Priming should occur in short, concise time periods in an environment that is relaxing for the student with Asperger Syndrome, and with a person who is patient and supportive.
Persistent vomiting or food refusal may require tube feeding (although this is rare). Management of congenital heart disease is as per the general population, however a dysplastic valve is more likely and therefore surgery may be more likely to be necessary. Routine paediatric investigations for failure to thrive and reduced growth velocity. Should be considered in the context of genetic management-which genes are tested for should be decided by a clinical geneticist. Management of congenital heart disease is as per the general population, however a dysplastic valve is more likely and surgery may be more likely to be necessary. Should be carried out at least once during mid/late childhood (5-11 years old), and before major surgery. Aspirin should be withheld before any surgical interventions, as per standard practice. Assess intellectual/cognitive abilities with special attention for learning difficulties as a result of motor delay, executive dysfunctions and inattention. Developmental delay caused by hypotonia will improve with occupational and physiotherapy. Ongoing review and support of learning and development with further assessment of special educational needs as required. Enrol patient in an individualised preventative oral healthcare programme from an early age. Routine follow up and regular dental examinations by a family dentist or local community dental services are essential. The likelihood of delayed puberty should be anticipated, and appropriate education and counselling provided around this issue. Access to social skills training, and programmes to teach basic self help and daily living skills, if required. No routine screening is recommended, however there should be a low threshold for investigation of neurological symptoms. Screen before any surgical intervention, and withhold aspirin prior to surgery, as per standard practice. Missing teeth/malocclusion/other dental anomalies: refer to a consultant in paediatric dentistry for multidisciplinary management. Refer for genetic counselling, mutation testing and discussion of risks to children and options in pregnancy, at an appropriate time. Prenatal features include; polyhydramnios, increased nuchal translucency, hydrops fetalis and cystic hygroma, with or without associated ascites, pleural effusion, renal abnormalities and congenital heart defects. Ultrasounds at 12-14 and 20 weeks and undertake mutation analysis if parental mutation known and clinical features are suggestive, if required. Potential difficulties, for example those arising from coagulation defects during childbirth, should be considered and planned for as appropriate. Repeat neuropsychological assessment if patient is symptomatic of mood/anxiety disorder(s), or if cognitive impairments are suspected. Management of specific complications, including epilepsy, will be as per the general population. Previously diagnosed adults: regular cardiac assessment of existing heart disease, or cardiac evaluation incase aortic disease missed previously. Avoid skin dryness, which can be worsened by long hot baths, perfumed soaps and dry atmospheres. Missing teeth/malocclusion/other dental anomalies: refer to a consultant in dentistry for multidisciplinary management. A case with a platelet cyclooxygenase-like deficiency and chronic idiopathic thrombocytopenic purpura. It contains information on over 5,000 conditions, including Williams Syndrome, and lists specialised clinics, diagnostic tests, patient organisations, research projects, clinical trials and patient registries relating specifically to Noonan Syndrome.
On average, Midwest Study participants who were looking for a job had been searching for 5. Length of Current Job Searcha (N = 157) Less than 1 month At least one but less than 6 months At least 6 but less than 12 months At least 12 but less than 24 months At least 24 months Mean length of current job search Median length of current job search a # 51 64 16 24 9 5. Chapin Hall at the University of Chicago 35 Income Seventy percent of the young adults in the Midwest Study reported having any income from employment during the past year compared with 94 percent of their Add Health counterparts (see Table 43). Moreover, when Midwest Study participants did have any income from employment, they had earned significantly less than their Add Health Study peers. In fact, the difference in median annual earnings between the groups was more than $18,000. Earnings during the Past Year: Midwest Study Compared with Add Health Study Midwest Study N # % 580 408 70. Many of these young adults reported income from sources other than their own employment. Limited to young adults who were with the custodial parent of at least one child whose other parent was not in the household. Asset accumulation is especially important for young people aging out of foster care who are less likely than other young adults to be able to depend on their parents or other family members for financial support in times of need. However, less than half of the Midwest Study participants reported having a checking or savings account (see Table 45). About the same percentage owned a motor vehicle and only 9 percent owned a home compared with 30 percent of their Add Health Study peers. Asset Accumulation: Midwest Study Compared with Add Health Study Midwest Study N # 593 277 595 288 564 53 % 46. Chapin Hall at the University of Chicago 37 Not only did many of the Midwest Study participants lack assets, but in addition, they often had incurred debt. Although only 12 percent reported borrowing at least $200 from family or friends, more than onethird reported having other debt, excluding student, home, or auto loans (see Table 46). Debts Borrowed at least $200 from relative or friend since most recent interview Any other outstanding debts a a N 594 593 # 70 211 % 11. Forty-five percent reported experiencing at least one of five material hardships during the past year compared with fewer than one-fifth of their Add Health Study peers (see Table 47). However, both samples were most likely to report "not having enough money to pay a utility bill. Economic Hardships during the Past Year: Midwest Study Compared with Add Health Study Midwest Studya N # 581 162 582 183 582 78 582 166 582 60 581 269 2. Add Health Study participants were asked if they had been without phone service for any reason. Approximately one-quarter of these young adults put off paying a bill in order to buy food and nearly as many received emergency food from a pantry (see Table 48). The other 8 items were only asked if the respondent was a parent living with at least one child. The first item is a screener and not used to compute the composite food security score. Twenty-five respondents with at least one resident child were not asked the food insecurity questions due to a problem with the programming of the survey instrument. The first 11 items were used to compute a food insecurity composite score for young adults who were not parents or young adults who were parents but not living with any of their children. These items plus eight additional items were used to compute a food insecurity composite score for young adults who were parents living with at least one child. Based on the number of affirmative responses that they gave, 28 percent of the young adults with no resident children and one-quarter of the young adults with at least one resident child would be categorized as having low or very low food security (see Table 50). Food Insecurity Scale Scores for Households With and Without Children # of affirmative responses Households with no resident child present (N = 317) High food security Marginal food security Low food security Very low food security Households with at least one resident child (N = 279) High food security Marginal food security Low food security Very low food security Zero One or two Three to five Six or more Zero One or two Three to seven Eight or more n 159 56 42 46 142 67 56 14 % 50. Two-thirds of the young women and 42 percent of the young men reported that they had been food stamp recipients. Where gender differences were found, young women were more likely than young men to report receiving benefits. During the past year, three-quarters of the young women compared with less than half of the young men had received benefits from at least one means-tested program. Among custodial parents, 86 percent of mothers compared with only 40 percent of fathers received benefits from one or more means-tested programs during the past year.
Sugimoto T, Kikkawa R, Haneda M, Shigeta Y: Effect of dietary protein restriction on proteinuria in non-insulin-dependent diabetic patients with nephropathy. Barsotti G, Ciardella F, Morelli E, Cupisti A, Mantovanelli A, Giovannetti S: Nutritional treatment of renal failure in type 1 diabetic nephropathy. Parillo M, Riccardi G, Pacioni D, Iovine C, Contaldo F, Isernia C, De Marco F, Perrotti N, Rivellese A: Metabolic consequences of feeding a high-carbohydrate, high-fiber diet to diabetic patients with chronic kidney failure. Coyne T, Olson M, Bradham K, Garcon M, Gregory P, Scherch L: Dietary satisfaction correlated with adherence in the Modification of Diet in Renal Disease Study. Coen G, Manni M, Addari O, Ballanti P, Pasquali M, Chicca S, Mazzaferro S, Mapoletano I, Napoletano I, Sardella D, Bonucci E: Metabolic acidosis and osteodystrophic bone disease in predialysis chronic renal failure: Effect of calcitriol treatment. Ferreira M: Diagnosis of renal osteodystrophy: When and how to use biochemical markers and noninvasive methods: When bone biopsy is needed. Hyperphosphatemia: Its consequences and treatment in patients with chronic renal disease. Llach F: Hyperphosphatemia in end-stage renal disease patients: Pathophysiological consequences. Atsumi K, Kushida K, Yamazaki K, Shimizu S, Ohmura A, Inoue T: Risk factors for vertebral fractures in renal osteodystrophy. Coco M, Rush H: Increased incidence of hip fractures in dialysis patients with low serum parathyroid hormone. Lau K: Phosphate excess and progressive renal failure: the precipitation-calcification hypothesis. Perit Dial Int 16:S190-S194, 1996 (suppl 1) Carlstedt F, Lind L, Wide L, Lindahl B, Hanni A, Rastad J, Ljunghall S: Serum levels of parathyroid hormone are related to the mortality and severity of illness in patients in the emergency department. J Lab Clin Med 104:1016-1026, 1984 Saha H: Calcium and vitamin D homeostasis in patients with heavy proteinuria. Ishimura E, Nishizawa Y, Inaba M, Matsumoto N, Emoto M, Kawagishi T, Shoji S, Okuno S, Kim M, Miki T, Morii H: Serum levels of 1,25-dihydroxyvitamin D, 24,25-dihydroxyvitamin D, and 25hydroxyvitamin D in nondialyzed patients with chronic renal failure. Coen G, Mazzaferro S, Ballanti P, Sardella D, Chicca S, Manni M, Bonucci E, Taggi F: Renal bone disease in 76 patients with varying degrees of predialysis chronic renal failure: A cross-sectional study. Madsen S, Olgaard K, Ladefoged J: Degree and course of skeletal demineralization in patients with chronic renal insufficiency. The relationship betweeen sensory and motor nerve conduction and kidney function, azotemia, age, sex, and clinical neuropathy. Morena F, Aracil F, Perez R, Valderrabano F: Controlled study on the improvement of quality of life in elderly hemodialysis patients after correcting end-stage renal disease-related anemia. Kidney Int 38:167-184, 1990 Walser M: Progression of chronic renal failure in man. Ruggenenti P, Perna A, Zoccali C, Gherardi G, Benini R, Testa A, Remuzzi G: Chronic proteinuric nephropathies. Hannedouche T, Chauveau P, Kalou F, Albouze G, Lacour B, Jungers P: Factors affecting progression in advanced chronic renal failure.
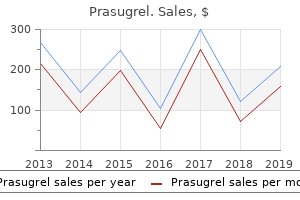
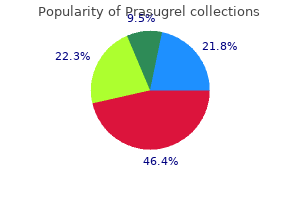
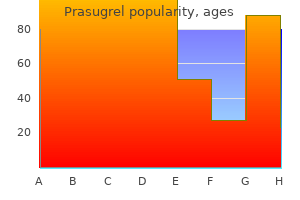
Seaweed Gelatin (Agar). Prasugrel.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96124
However, estrogen treatment down-regulates the density of this receptor, which might be a mechanism whereby estrogen protects adipose tissue from androgen effects. Estrogen by itself seems to protect postmenopausal women receiving replacement therapy from visceral fat accumulation (121). Estrogen receptors are expressed in human adipose tissue (122) and show a regional variation of density, but whether the quantity of these receptors is of physiological importance has not been clearly established (34). Thyroid hormones have multiple catabolic effects on fat cells as a result of interactions with the adrenergic receptor signal transduction system, and most of these interactions are also present in human fat cells (125). There are data regarding the characterization of the nuclear T3 receptor in human fat cells (126). Although receptor regulation has not yet been demonstrated, there is little doubt that the thyroid hormone receptors are important for the function of human adipose tissue (125). Further, no data are available on the correlation between visceral fat mass and thyroid hormone levels. Adenosine behaves as a potent antilipolytic and vasodilator agent and can be considered as an autocrine regulator of both lipolysis and insulin sensitivity in human adipose tissue. Site differences in ambient adenosine concentration, perhaps controlled by blood flow, may also modulate adipose tissue metabolism (7). Adenosine content is higher in omental than in abdominal subcutaneous adipose tissue, but the receptor-dependent inhibition of lipolysis is, as indicated before (102), less pronounced in the former than in the latter depot (127). However, despite strong antilipolytic effect of adenosine analogs, human adipocytes contain few adenosine type Al receptors, regardless of the fat depot considered (128). The residual variance corresponded to environmental factors, but some factors (cultural, nongenetic) could be transmitted from parents to descendents and sometimes were confounded by genetic effects (131). However, after adjustment of the visceral adipose tissue for the fat mass, the effect of the gene with the major effect was not more compatible with a mendelian transmission. These results suggested the presence of a pleiotropism: the gene with the major effect, identified by the fat mass (135), could similarly influence the amount of visceral fat (133). This phenotypic covariation is characterized by familial resemblances and the existence of common genetic factors for the two phenotypes (G3) explaining their 30% covariation. These results have confirmed the presence of a genetic pleiomorphism and suggested the presence of genes affecting simultaneously the amounts of fat mass and visceral abdominal fat. The interactions of the effects of genotype and environment evaluated in monozygotic twins, when the energy balance is manipulated, indicated that even though there were large interindividual differences in the response to excess or negative energy balance, there was a significant within-pair resemblance in response (96, 137). In effect, in response to overfeeding, there was at least 3 times more variance in response between pairs than within pairs for the gains in body weight, fat mass, and fat-free mass (96). In relation to the response to the negative energetic balance, at least 7 times Downloaded from academic. Schematic representation of the genetic effects on total fat mass and visceral fat (adjusted for the fat mass) and on the co-variation between the two phenotypes (Quebec Family Study, 1996). G1 and G2 represent the genetic effects specific for the total fat mass and visceral fat, respectively. E1 and E2 represent the specific effects of the environment on total fat mass and visceral fat, respectively. This intrapair similarity in the response to either excess or deficient energy balance is also observed in relation to the abdominal visceral fat (131). Thus, the interaction between genotype and environment is important to consider in the study of the genetics of obesity since the propensity to fat accumulation is influenced by the genetic characteristics of the subject. Several candidate genes as well as random genetic markers were found to be associated with obesity as well as body fat and fat distribution in humans. The current human obesity gene map, based on results from animal and human studies, indicates that all chromosomes, with the exception of the Y chromosome, include genes or loci potentially involved in the etiology of obesity (138). This mutation was also shown to be associated with abdominal visceral obesity in Japanese subjects, with lower triglycerides in the Trp64Arg homozygotes but not heterozygotes (143). It has been suggested that those with the mutation may describe a subset of subjects characterized by decreased lipolysis in visceral adipose tissue. Previously, it was reported by the same group that apo-B-100 gene EcoR-1 polymorphism appeared to modulate the magnitude of the dyslipidemia generally found in the insulinresistant state linked with visceral obesity (145). These studies are a demonstration of a significant interaction between visceral obesity and a polymorphism for a gene playing an important role in lipoprotein metabolism. However, the association with abdominal visceral fat area was seen only in subjects of the lower tertile of the percent body fat level.
Despite better microvascular, macrovascular, and allcause mortality outcomes, intensive therapy was associated with a higher rate of severe hypoglycemia (61 episodes per 100 patient-years of therapy). Longeracting basal analogs (U-300 glargine or degludec) may convey a lower hypoglycemia risk compared with U-100 glargine in patients with type 1 diabetes (18,19). Rapid-acting inhaled insulin to be used before meals is now available and may reduce rates of hypoglycemia in patients with type 1 diabetes (20). Postprandial glucose excursions may be better controlled by adjusting the timing of prandial insulin dose administration. The optimal time to administer prandial insulin varies, based on the type of insulin used (regular, rapid-acting analog, inhaled, etc. Recommendations for prandial insulin dose administration should therefore be individualized. Insulin Injection Technique Ensuring that patients and/or caregivers understand correct insulin injection technique is important to optimize glucose control and insulin use safety. Thus, it is important that insulin be delivered into the proper tissue in the right way. Recommendations have been published elsewhere outlining best practices for insulin injection (21). Exogenous-delivered insulin should be injected into subcutaneous tissue, not intramuscularly. Recommended sites for insulin injection include the abdomen, thigh, buttock, and upper arm (21). Injection site rotation is additionally necessary to avoid lipohypertrophy and lipoatrophy (21). Lipohypertrophy can contribute to erratic insulin absorption, increased glycemic variability, and unexplained hypoglycemic episodes (28). Patients and/or caregivers should receive education about proper injection site rotation and to recognize and avoid areas of lipohypertrophy (21). As referenced above, there are now numerous evidence-based insulin delivery recommendations that have been published. Proper insulin injection technique may lead to more effective use of this therapy and, as such, holds the potential for improved clinical outcomes. Noninsulin Treatments for Type 1 Diabetes Injectable and oral glucose-lowering drugs have been studied for their efficacy as adjuncts to insulin treatment of type 1 diabetes. Pramlintide is based on the naturally occurring b-cell peptide amylin and is approved for use in adults with type 1 diabetes. Similarly, results have been reported for several agents currently approved only for the treatment of type 2 diabetes. The addition of metformin to adults with type 1 diabetes caused small reductions in body weight and lipid levels but did not improve A1C (31,32). The risks and benefits of adjunctive agents beyond pramlintide in type 1 diabetes continue to be evaluated through the regulatory process; however, at this time, these adjunctive agents are not approved in the context of type 1 diabetes (37). Given the potential adverse effects of immunosuppressive therapy, pancreas transplantation should be reserved for patients with type 1 diabetes undergoing simultaneous renal transplantation, following renal transplantation, or for those with recurrent ketoacidosis or severe hypoglycemia despite intensive glycemic management (38). Considerations include comorbidities (atherosclerotic cardiovascular disease, heart failure, chronic kidney disease), hypoglycemia risk, impact on weight, cost, risk for side effects, and patient preferences. E the American Diabetes Association/ European Association for the Study of Diabetes consensus report "Management of Hyperglycemia in Type 2 Diabetes, 2018" (39) recommends a patient-centered approach to choosing appropriate pharmacologic treatment of blood glucose. Lifestyle modifications that improve health (see Section 5 "Lifestyle Management") should be emphasized along with any pharmacologic therapy. See Sections 12 and 13 for recommendations specific for older adults and for children and adolescents with type 2 diabetes, respectively. Initial Therapy Metformin should be started at the time type 2 diabetes is diagnosed unless there are contraindications; for most patients this will be monotherapy in combination with lifestyle modifications. Metformin is effective and safe, is inexpensive, and may reduce risk of cardiovascular events and death (40). Metformin is available in an immediate-release form for twicedaily dosing or as an extended-release Pharmacologic Approaches to Glycemic Treatment S93 Table 9. S94 Pharmacologic Approaches to Glycemic Treatment Diabetes Care Volume 42, Supplement 1, January 2019 Figure 9. S96 Pharmacologic Approaches to Glycemic Treatment Diabetes Care Volume 42, Supplement 1, January 2019 Table 9.

The plate should be removed and rotated as above, and then returned for a second 4minute incubation. False-negative reactions may occur, usually due to prozoning, which may be overcome by diluting the serum or retesting after a given time. This is prepared from tablets available commercially; otherwise it may be prepared from a stock solution of sodium chloride (42. However, this buffer contains barbituric derivatives that are no longer available in several countries. Satisfactory results may be also obtained with a barbituric-free solution of sodium chloride 0. Numerous variations of the test exist but, whichever procedure is selected, the test must use an antigen that has been prepared from an approved smooth strain of B. A control serum that gives a minimum positive reaction should be tested in each set of tests to verify the sensitivity of test conditions. The absence of anti-complementary activity is checked for each serum in the first row. Nevertheless, the technique used and the interpretation of results must have been validated in accordance with the principles laid down in Chapter 1. Infection with Brucella in pigs: i) In the absence of international standard serum for porcine brucellosis the test should be duly validated and the cut-off established in the test population with appropriate validation techniques (see chapter 1. Nevertheless, the technique used and the interpretation of results must have been validated in accordance with the principles laid down in chapter 1. Infection with Brucella in pigs: i) In the absence of an international standard serum for porcine brucellosis, the test should be duly validated and the cut-off established in the test population with appropriate validation techniques (see chapter 1. Some protocols are less sensitive or less specific than others; therefore results obtained from different assays are not always comparable. An additional positive serum (internal control) must be included in each plate to validate the repeatability of the test from plate to plate and from day to day. It is a homogeneous assay in which analytes are not separated and it is therefore very rapid. The supernatant solution is then treated with 20 g of trichloroacetic acid to precipitate any proteins and nucleic acids. Accordingly, like all other serological tests, positive reactions should be investigated using suitable confirmatory and/or complementary strategies. Sheep and goat as well as porcine sera are diluted 1/10 for the plate test or 1/25 (goat and porcine) and 1/40 (sheep) for the tube test. A reading (in millipolarisation units, mP) over the established threshold level is indicative of a positive reaction.
The following are some examples: Allergy: Patients who have had a prior allergic-like reaction or unknown-type reaction. A prior allergic-like or unknown type reaction to the same class of contrast medium is considered the greatest risk factor for predicting future adverse events. In general, patients with unrelated allergies are at a 2- to 3-fold increased risk of an allergic-like contrast reaction, but due to the modest increased risk, restricting contrast medium use or premedicating solely on the basis of unrelated allergies is not recommended. For example, a prior reaction to gadolinium-based contrast medium does not predict a future reaction to iodinated contrast medium, or vice versa, more than any other unrelated allergy. Asthma: A history of asthma increases the likelihood of an allergic-like contrast reaction [3,7]. Due to the modest increased risk, restricting contrast medium use or premedicating solely on the basis of a history of asthma is not recommended. Cardiac Status: Patients with severe cardiac disease may be at increased risk of a non-allergic cardiac event if an allergic-like or non-allergic contrast reaction occurs. Anxiety: There is some evidence that contrast reactions are more common in anxious patients [8]. Reassuring an anxious patient before contrast medium injection may mitigate the likelihood of a mild contrast reaction. Other Historical and Pre-Procedure Considerations Age and Gender: Infants, neonates, children, and the elderly have lower reaction rates than middle-aged patients [1,9] Male patients have lower reaction rates than female patients. Due to the modest increased risk, restricting contrast medium use or premedicating solely on the basis of patient age or gender is not recommended. Beta-Blockers: Some have suggested that use of beta-blockers lowers the threshold for contrast reactions, increases the severity of contrast reactions, and reduces the responsiveness of treatment with epinephrine [10]. Due to the modest increased risk, restricting contrast medium use or premedicating solely on the basis of betablocker use is not recommended. Patients on beta-blocker therapy do not need to discontinue their medication(s) prior to contrast medium administration. Sickle-Cell Trait/Disease: Some have suggested that contrast medium exposure to patients with sickle cell trait or sickle cell disease might increase the risk of an acute sickle crisis; however, there is no evidence this occurs with modern iodinated or gadolinium-based contrast medium [11]. Therefore, restricting contrast medium use or premedicating solely on the basis of sickle cell trait or sickle cell disease is not recommended. Therefore, restricting contrast medium use or premedicating solely on the basis of a history of pheochromocytoma is not recommended. Direct injection of any type of contrast medium into the adrenal or renal arteries in a patient with pheochromocytoma has not been adequately studied and is of unknown risk. Premedication is not recommended solely on the basis of a history of myasthenia gravis. It is controversial whether iodinated contrast medium should be considered a relative contraindication in patients with myasthenia gravis. Therefore, restricting contrast medium use or premedicating solely on the basis of a history of hyperthyroidism is not recommended. In patients with acute thyroid storm, iodinated contrast medium exposure can potentiate thyrotoxicosis; in such patients, iodinated contrast medium should be avoided. In patients considering radioactive iodine therapy or in patients undergoing radioactive iodine imaging of the thyroid gland, administration of iodinated contrast medium can interfere with uptake of the treatment and diagnostic dose. If iodinated contrast medium was administered, a washout period is suggested to minimize this interaction. The washout period is ideally 3-4 weeks for patients with hyperthyroidism, and 6 weeks for patients with hypothyroidism [16,17]. Normal Thyroid Function: Iodinated contrast medium does not affect thyroid function test results in patients with a normally functioning thyroid gland [15]. Multiple studies have shown that a single dose of iodinated contrast medium administered to a pregnant mother has no effect on neonatal thyroid function. Concomitant use of iodinated contrast medium with certain intra-arterial medications. Decisions about the use and timing of such medication are outside the scope of this document.
They may think twice before approaching a suspicious person or making a traffic stop. The Illinois Attorney General Lisa Madigan intervened by filing a separate lawsuit and negotiating a separate consent decree. Kevin Graham, president of the Fraternal Order of Police there, said in a statement that the proposed consent decree "`is politically motivated and threatens both public safety and the well-being of our members. This is not evidence that the Department of Justice is not interfering with local control. We on the Commission cannot speak to the question of the performance of any of particular police department. As a result, we cannot we opine on whether adding layers of bureaucracy will be a good thing or a bad thing in a particular case. Mercifully, we have not yet reached the point where bureaucracy is considered a good unto itself. However, I must point out that one of her statements seems to have inadvertently misstated something. The Court ultimately found that that the Los Angeles Police Protection League should have been granted leave to intervene as of right. In the interim, however, the District Court had entered the consent decree without the participation of either the Los Angeles Police Protection League or the Community Interveners. On this matter, the Court held that "it was proper for the district court to continue to act in the case notwithstanding the intervention appeal because no stay was entered" and stated that its holding "does not require the district court to turn back the clock or rescind the consent decree. The Commission decided on this topic in the wake of protests in Ferguson, Missouri after the death of Michael Brown. The Criminal Section wrote in its report: As Wilson drove toward Brown and Witness 101, he told the two men to walk on the sidewalk. Wilson then called for backup, stating, "Put me on Canfield with two and send me another car. According to three autopsies, Brown sustained a close range gunshot wound to the fleshy portion of his right hand at the base of his right thumb. However, as discussed later in this report, those witness accounts could not be relied upon in a prosecution because credible witness accounts and physical and forensic evidence, i. The autopsy results alone do not indicate the direction Brown was facing when he received two wounds to his right arm, given the mobility of the arm. However, as detailed later in this report, there are no witness accounts that could be relied upon in a prosecution to prove that Wilson shot at Brown as he was running away. Witnesses who say so cannot be relied upon in a prosecution because they have given accounts that are inconsistent with the physical and forensic evidence or are significantly inconsistent with their own prior statements made throughout the investigation. Brown then turned around and came back toward Wilson, falling to his death approximately 21. As detailed throughout this report, several witnesses stated that Brown appeared to pose a physical threat to Wilson as he moved toward Wilson. According to these witnesses, who are corroborated by blood evidence in the roadway, as Brown continued to move toward Wilson, Wilson fired at Brown in what appeared to be self-defense and stopped firing once Brown fell to the ground. Witness accounts and an audio recording indicate that when Wilson and Brown were on the roadway, Wilson fired three gunshot volleys, pausing in between each one. As documented by crime scene photographs, Brown fell to the ground with his left, uninjured hand balled up by his waistband, and his right, injured hand palm up by his side. Although there are several individuals who have stated that Brown held his hands up in an unambiguous sign of surrender prior to Wilson shooting him dead, their accounts do not support a prosecution of Wilson. Certain other witnesses who originally stated Brown had his hands up in surrender recanted their original accounts, admitting that they did not witness the shooting or parts of it, despite what they initially reported either to federal or local law enforcement or to the media. While credible witnesses gave varying accounts of exactly what Brown was doing with his hands as he moved toward Wilson-i. Although some witnesses state that Brown held his hands up at shoulder level with his palms facing outward for a brief moment, these same witnesses describe Brown then dropping his hands and then "charging" at Wilson. Instead, the report uncritically repeats the statement of Montague Simmons from the Organization for Black Struggle, who stated at the hearing: the U. Commission on Civil Rights has now cast its eyes upon our community because the execution of Mike Brown, the corrupt and inept ways of the investigation as follows: the investigation that ended in a fiasco of a grand jury that would have amounted to business as usual, except for the anger, tenacity and determination of the people who have been in the streets over 250 days.
References:




