If this happens repeatedly, it suggests abnormal joint laxity, capsular or ligamentous deficiency, or some type of internal derangement such as a torn meniscus or a loose body in the joint. Patients often forget to mention previous illnesses or accidents, or they may simply not appreciate their relevance to the present complaint. They should be asked specifically about childhood disorders, periods of incapacity and old injuries. Similarly, certain rheumatic disorders may be suggested by a history of conjunctivitis, iritis, psoriasis or urogenital disease. Metastatic bone disease may erupt many years after a mastectomy for breast cancer. Patients should also be asked about previous medication: many drugs, and especially corticosteroids, have long-term effects on bone. Alcohol and drug abuse are important, and we must not be afraid to ask about them. When dealing with a suspected case of bone or joint infection, ask about communicable diseases, such as tuberculosis or sexually transmitted disease, in other members of the family. It is important to establish its exact distribution; from this we can tell whether the fault lies in a peripheral nerve or in a nerve root. We should also ask what makes it worse or better; a change in posture might be the trigger, thus focussing attention on a particular site. There are the obvious things such as the level of care and nutrition in children; dietary constraints which may cause specific deficiencies; and, in certain cases, questions about smoking habits, alcohol consumption and drug abuse, all of which call for a special degree of tact and non-judgemental enquiry. Loss of function Functional disability is more than the sum of individual symptoms and its expression depends upon the needs of that particular patient. This will help to answer the question: `What has the patient lost and what is he or she hoping to regain With time his teaching has been extended and we now add test, to include the special manoeuvres we employ in assessing neurological integrity and complex functional attributes. It is important to look for deformity in three planes, and always compare the affected part with the normal side. In many joint disorders and in most nerve lesions the limb assumes a characteristic posture. Watson: You appeared to read a good deal upon [your client] which was quite invisible to me. The clues are endless and the game is played by everyone (qualified or lay) at each new encounter throughout life. When we proceed to the structured examination, the patient must be suitably undressed; no mere rolling up of a trouser leg is sufficient. Only by proceeding in a purposeful, orderly way can we avoid missing important signs. Alan Apley, who developed and taught the system used here, shied away from using long words where short ones would do as well. Abnormal creases, unless due to fibrosis, suggest underlying deformity which is not always obvious; tight, shiny skin with no creases is typical of oedema or trophic change. The other scars are due to postoperative infection; one of the sinuses is still draining. General survey Attention is initially focussed on the symptomatic or most obviously abnormal area, but we must also look further afield.
This can demonstrate conduction block or slowing or normal continuity of the nerve. Cord-to-cord stimulation and cord-to-cortical potential measurement are usually resolved as averaged recordings to reveal intraoperative evidence of spinal pathway disruption. If surgical treatment is being considered, it should never be based on a single assessment when, due to stress, the child appears to have abnormally high tone and muscle contractures. This usually appears as a spastic palsy on one side of the body with the upper limb more severely affected than the lower. Some disorder of upper limb function is invariably present but signs may be subtle. Side to side involvement may be asymmetrical and the terms asymmetric diplegia and occasionally bilateral hemiplegia are used. The less severely affected children can have reasonable mobility but the non-walking diplegic patient may be similar to the total body involvement group discussed below. Diagnosis in infancy the full-blown clinical picture may take months or even years to develop. A history of prenatal toxaemia, haemorrhage, premature birth, difficult labour, foetal distress or kernicterus should arouse suspicion. A neonatal ultrasound scan of the head may identify intracerebral bleeding that would increase the likelihood of later problems. Early symptoms include difficulty in sucking and swallowing, with dribbling at the mouth. The normal child holds up its head at 3 months, sits up at 6 months and begins walking at about 1 year. Diagnosis in later childhood Most children presenting to the orthopaedic surgeon have already had the diagnosis made. Occasionally, for example with a mild hemiplegia or a symmetrical mild diplegia, the diagnosis has not been made and the child is simply referred for advice about their gait or their tendency to trip and fall. A familiarity and knowledge of the normal developmental milestones and gait patterns helps the clinician identify the child who is outside the normal range. Bleck (1987) has described seven tests for children 10 Neuromuscular disorders (a) (b) (c) (d) 10. The primitive neck-righting reflex, asymmetrical and symmetrical tonic neck reflexes, the Moro reflex and the extensor thrust response should all have disappeared at 1 year of age. Children who retain more than two primitive reflexes after that age, cannot sit unsupported by 4 years and cannot walk unaided by 8 years are unlikely ever to walk independently. Ideally the child should be reviewed by a multidisciplinary team so that speech, hearing, visual acuity, intelligence and motivation can also be assessed. Since cerebral palsy is essentially a disorder of posture and movement, the child should be carefully observed sitting, standing, walking and lying. The system is reliable and valid; it aids in communication between members of the multidisciplinary team and is a useful guide to management. With tight hamstrings, the normal lumbar lordosis may be obliterated and the child may have difficulty standing unsupported. Often attempts to correct one deformity may aggravate another and it is important to establish which deformity is the primary one and which are compensatory. Balance reactions are often poor and a gentle push that would force a normal child to take a step in the appropriate direction to maintain his or her balance may simply knock over a child with cerebral palsy. Dystonic, athetoid and ataxic movements may become more noticeable during walking. In hemiplegics, best behaviour walking may demonstrate a flat foot pattern with the heel coming down most of the time while the more normal or representative pattern will highlight the asymmetric flexed knee and toe-walking pattern. Each limb must be observed in both the stance and swing phases of gait and in the coronal, sagittal and transverse planes. In the spastic diplegic patient, the standing posture mentioned above is influential in defining their walking pattern too.
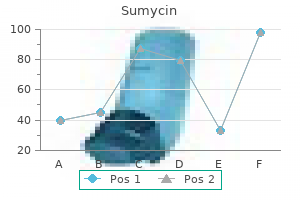
| Comparative prices of Sumycin | ||
| # | Retailer | Average price |
| 1 | Dollar General | 494 |
| 2 | Rite Aid | 293 |
| 3 | Giant Eagle | 415 |
| 4 | Albertsons | 796 |
| 5 | Barnes & Noble | 264 |
| 6 | A&P | 192 |
| 7 | Subway | 752 |
| 8 | Target | 847 |
| 9 | Gap | 786 |
| 10 | Best Buy | 740 |
The condition may include whether a surface is smooth or textured and whether the item is dusty, rusty, or contains any residue. Prior to using any development techniques, the item should be carefully examined for the presence of any patent impressions. If there are no impressions of value noted during the initial observations, the notes should reflect that no patent prints or no patent prints of value were observed. If patent impressions of value are present, their location and orientation on the item should be documented (through notes, sketches, or photographs) and an examination-quality photograph should be taken. No patent prints of value visible on the blade; no patent prints visible on handle. If the item is too small or writing directly on the item will alter or destroy any evidentiary value, the item may be placed inside a container. For example, if a bullet casing was taken from the scene, the casing could be placed in an envelope that is marked with a unique identifier. The casing, inside the marked envelope, can then undergo final packaging and sealing. The elements to be considered in the analysis of friction ridge impressions should be detailed in the technical or operational manual for the laboratory. The quality of level-one, level-two, and level-three detail is influenced by the following factors: pressure distortion, deposition pressure, development medium, matrix, and substrate (Ashbaugh, 1999, p 109). Documentation of analysis may be minimal, using symbols to mark directly on the lift cards and photographs. This is particularly effective when the original lifts or photographs are part of the case record. If symbols are used to document the analysis, the proper use and meaning of the symbols should be detailed in the technical or operational manual. If L1 and L2 are part of the case record, they should contain all of the basic elements of the analysis. L1 and L2 are black powder lifts (that is, black powder is the developmental medium) and indicate the location from which the latent prints were recovered (substrate). The notes must contain enough detail to discern which photograph or lift was examined and the results of the analysis of the latent prints. Without the original or legible reproductions of the original latent lifts and photographs in the case record, this connection would not be possible. Expanded documentation of the analysis of a complex impression may include photographic enlargements of the impression and detailed notes regarding all of the elements of analysis and factors of quality. Anatomical aspect: Based on adjacent impressions, L2A is consistent with an impression of a left index finger. Deposition pressure: Average deposition pressure across the entire impression, possibly a bit lighter toward the tip of the finger. Indicators of pressure distortion are marked in the photographic enlargement as a, b, c, d, and. The original touch of the finger is indicated as "a" As the finger slid across the surface, the detail in. The direction of travel is noted in the striations present in the impression; one such striation is marked "b" Another indication of pressure distortion.
At this point, the embryonic epidermis is three to four cell layers thick, but it is still smooth on its outer and inner surfaces. Keratinocytes are tightly bound to each other by desmosomes, and the cells of the basal layer are attached to the basement membrane by hemidesmosomes (Holbrook, 1991a, p 5). In fact, axons can be traced to the superficial levels of the dermis, and in some cases they almost abut the basal lamina of the epidermis. The dermis becomes distinguishable from deeper subcutaneous tissue due largely to a horizontal network of developing blood vessels. Unlike other epidermal structures, blood vessels continue to alter with aging, as some capillary loops are lost and new ones arise from the interpapillary network. Unlike the developing primary ridges, the vascular network is not a permanent structure. As volar epidermal cells divide, shallow "ledges" (Hale, 1952) can be seen on the bottom of the epidermis. These ledges delineate the overall patterns that will become permanently established on the volar surfaces several weeks later (Babler, 1991, p 101; Evatt, 1906). Another plausible theory is that developing nerves may interact with epidermal cells to stimulate clustered interactions that blend together in the early stages of ridge development. At the time of embryonic friction ridge formation, the central nervous and cardiovascular systems are undergoing a critical period of development (Hirsch, 1964). Researchers have reported innervation at the sites of ridge formation immediately preceding the appearance of friction ridges and suggest that innervation could be the trigger mechanism for the onset of proliferation (Bonnevie, 1924; Dell and Munger, 1986; Moore and Munger, 1989). Early research on pattern distribution established "developmental fields" or groupings of fingers on which patterns, had a greater tendency to be similar (Meier, 1981; Roberts, 1982; Siervogel et al. Other interesting hypotheses have been published regarding the connection between innervation and friction ridge patterning, but the main consideration for the purposes of friction ridge formation is that specific parts of the nervous system are undergoing development at the same time that ridges begin to appear on the surface of the hands. The presence of nerves and capillaries in the dermis before friction ridge formation may be necessary for friction ridge proliferation. It would seem that complex simultaneous productions such as friction ridge formation would benefit from being in communication with the central nervous system or the endocrine and exocrine (hormone) systems (Smith and Holbrook, 1986). However, it is doubtful that nerves or capillaries independently establish a map that directly determines the flow of the developing friction ridges. It seems more likely that the alignment of the nerves and capillaries is directed by the same stresses and strains on the developing hand that establish ridge alignment (Babler, 1999; Smith and Holbrook, 1986). It is well recognized in cell biology that physical pressure on a cellular system can trigger electrochemical changes within that system. Merkel cells occupy the epidermis just prior to innervation along those pathways (Holbrook, 1991a), suggesting that even before ridge formation, the stresses created by the different growth rates of the dermis and epidermis are causing differential cell growth along invisible lines that already delineate pattern characteristics (Loesch, 1973). Regardless of the trigger mechanism controlling the onset of the first primary ridge proliferations, the propagation of primary ridges rapidly continues. The cell growth during this phase of development is along the primary ridge, in what has been labeled the "proliferative compartment"The proliferative compartment. During this time, primary ridges (as marked by the arrow) increase in depth and breadth.
Effectiveness of syphilis treatment using azithromycin and/or benzathine penicillin in Rakai, Uganda. Single-dose azithromycin versus penicillin G benzathine for the treatment of early syphilis. Azithromycin treatment failures in syphilis infections-San Francisco, California, 2002-2003. Evaluation of macrolide resistance and enhanced molecular typing of Treponema pallidum in patients with syphilis in Taiwan: a prospective multicenter study. Response of latent syphilis or neurosyphilis to ceftriaxone therapy in persons infected with human immunodeficiency virus. Normalization of serum rapid plasma reagin titer predicts normalization of cerebrospinal fluid and clinical abnormalities after treatment of neurosyphilis. Jarisch-Herxheimer reaction after penicillin therapy among patients with syphilis in the era of the hiv infection epidemic: incidence and risk factors. Discordant Syphilis Immunoassays in Pregnancy: Perinatal Outcomes and Implications for Clinical Management. Maternal syphilis and vertical perinatal transmission of human immunodeficiency virus type-1 infection. Apparent failure of one injection of benzathine penicillin G for syphilis during pregnancy in human immunodeficiency virus-seronegative African women. A study evaluating ceftriaxone as a treatment agent for primary and secondary syphilis in pregnancy. In 2011, the subgenus Biverticillium was found to form a monophyletic group with Talaromyces that is distinct from Penicillium, and was taxonomically unified with the Talaromyces genus. The wild bamboo rat in highland areas in the endemic regions is the known animal reservoir of T. Reactivation of latent infections has been demonstrated in non-autochthonous cases with a history of remote travel to the endemic countries and can occur many years after exposure. Donor-acquired transmission has been reported in a lung-transplant recipient from Belgium. The infection frequently begins as a subacute illness characterized by fever, weight loss, hepatosplenomegaly, lymphadenopathy, and respiratory and gastrointestinal abnormalities. Gastrointestinal involvement presenting as diarrhea or abdominal pain occurs in 30% of patients. Significant hepatosplenomegaly is present in 70% of patients and together with intra-abdominal lymphadenopathy cause abdominal distention and pain. Skin lesions in talaromycosis have typical central-necrotic appearance and can be a diagnostic sign. However, skin lesions are a late manifestation of talaromycosis and are absent in up to 60% of patients. Culture results usually return within 4 days to 5 days but can take up to 14 days. Diagnostic delay, particularly in patients presenting without fever or skin lesions, is associated with increased mortality. Identification of a clear midline septum in a dividing yeast cell is what distinguishes T. The suppurative reaction develops with the joining of multiple abscesses seen in the lung and subcutaneous tissues of immunocompetent patients. The anergic and necrotizing reaction is characterized by focal necrosis surrounded by distended histiocytes containing proliferating fungi seen in the lung, liver, and spleen of immunocompromised patients. Microscopically, filamentous hyphae with characteristic spore-bearing structures called conidiophores and conidia can be seen.
Syndromes
Processing techniques should be reviewed periodically to ensure that the techniques are current and still effective. This review will allow for updates and revisions to be made to the processing procedure. The quality manager may have casework responsibilities along with managing the quality assurance program. It is important that an agency document the specific requirements and duties expected of this position. These may include, but are not limited to , qualifications of the quality manager; time limits, if any, that a person shall be designated as quality manager; reviewing and updating the quality manual; disseminating quality assurance program policies and updates to all examiners and management; completing all case file reviews or overseeing the work produced by quality reviewers; maintaining all quality records; tracking all quality issues; and producing a written report annually detailing the quality record of the agency. These educational opportunities may include such coursework as undergraduate or postgraduate classes or degrees, academic or service-related seminars, and educational conferences provided by professional organizations. An agency may wish to include in this policy the tracking of individual requests or attendance at any of the abovementioned continuing education opportunities. By tracking these requests and attendance records, an agency may better identify which individuals strive to further their knowledge about their profession, which may be acknowledged during a performance review. These minimums should be clear and precise to allow for easy understanding and should include all requirements for evidence handling, evidence examination, evidence preservation, examination documentation, evidence disposition, and report wording. If an agency establishes minimum standards and controls, it must establish a policy for reevaluating them. This reevaluation should include a timetable to ensure that all standards and controls are accurate and current with generally accepted scientific practices. Organization and management requirements may include the delineation of organizational structure, administrative practices, and delegation of authority. These requirements may include minimum educational requirements, specific undergraduate or postbaccalaureate class-specific requirements, and employee development by attending professional organization meetings and seminars. This policy should address safety showers, eye wash stations, fire extinguishers, fume hood air flow requirements, and time frames for verifying the working condition of these safety features. In addition, a facility requirement policy should contain specific time frames and conditions, such as the minimum number of staff required onsite to ensure the safety of staff when engaging in certain activities, such as chemical processing or laser examination. These programs have been promoted to provide the criminal justice system with generally accepted methods for quality assurance. As examiners, we owe it to the community we serve to produce a quality work product each time we work a case, no matter what the offense. A reproduction of the friction ridge arrangements on a fingerprint, palmprint, or footprint may be left on an object when it is touched. This permits the impression to be used for the personal identification of individuals in criminal investigations. Thus, the forensic science of fingerprints, palmprints, and footprints is utilized by law enforcement agencies in support of their investigations to positively identify the perpetrator of a crime. This chapter will address the laws and rules of evidence as they apply to friction ridge impression evidence. Historical court decisions and recent appellate and United States Supreme Court rulings will be addressed. This chapter will primarily address federal court decisions and the Federal Rules of Evidence, which may not be applicable to all states. The term "friction ridge impression" will be used to refer to any impression made from human friction ridge skin. There are two different types of friction ridge impressions: those of known individuals intentionally recorded, and impressions from one or more unknown persons on a piece of evidence from a crime scene or related location; the latter are generally referred to as latent prints. The scope of this chapter will include legal aspects associated with experts and evidence, and legal challenges to the admissibility of friction ridge impression evidence. The text makes occasional references to laws or court decisions of specific states or foreign countries when notable. The reader is strongly encouraged to consult those legal sources that more particularly govern the jurisdiction in which the expert will be testifying. How these rules affect examiners of friction ridge impressions will be discussed later. At this point, the discussion is limited to defining the terms the law of evidence uses in connection with legal proceedings. A witness who will be offering opinion testimony must first be shown to be qualified as an expert.
The margin of resection most likely to be positive is the superior mesenteric artery margin along the right lateral border of the superior mesenteric artery. Incomplete resection resulting in a grossly positive retroperitoneal margin provides no survival advantage from surgical resection (compared with those who receive chemoradiation and no surgery). The natural history of these tumors is poorly understood due to their relative rarity, but demonstrated prognostic factors include patient age, distant metastases, tumor functional status, and degree of differentiation. Including these tumors in the pancreatic cancer staging system will allow for improved data collection and subsequent identification of potential prognostic factors. Job Name: - /381449t being classified as benign or malignant should be staged by this system and reported to cancer registries. Recommendations for the reporting of pancreatic specimens containing malignant tumors. Application of the pancreatic adenocarcinoma staging system to pancreatic neuroendocrine tumors. Prognostic score predicting survival after resection of pancreatic neuroendocrine tumors: analysis of 3851 patients. Relationship between hospital volume and late survival after pancreaticoduodenectomy. Major vascular resection as part of pancreaticoduodenectomy for cancer: radiologic, intraoperative, and pathologic analysis. Long-term survival after curative resection for pancreatic ductal adenocarcinoma: clinicopathologic analysis of 5-year survivors. Thinsection contrast-enhanced computed tomography accurately predicts resectability of malignant pancreatic neoplasms. Prognostic factors associated with resectable adenocarcinoma of the head of the pancreas. Long-term survival after resection for ductal adenocarcinoma of the pancreas: is it really improving Endoscopic ultrasound and fine needle aspiration for the valuation of pancreatic masses. Historical, current and future perspectives on gastrointestinal and pancreatic endocrine tumors. Other less common factors, such as asbestos exposure, may contribute to the development of lung cancer. In recent years, the level of tobacco exposure, generally expressed as the number of cigarette pack-years of smoking, has been correlated with the biology and clinical behavior of this malignancy. Lung cancer is usually diagnosed at an advanced stage and consequently the overall 5-year survival for patients is approximately 15%. However, patients diagnosed when the primary tumor is resectable experience 5-year survivals ranging from 20 to 80%. Clinical and pathologic staging is critical to selecting patients appropriately for surgery and multimodality therapy. The great vessels include: Aorta Superior vena cava Inferior vena cava Main pulmonary artery Intrapericardial segments of the trunk of the right and left pulmonary artery Intrapericardial segments of the superior and inferior right and left pulmonary veins Regional Lymph Nodes. During the past three decades, two different lymph node maps have been used to describe the regional lymph nodes potentially involved by lung cancers. The nomenclature for the anatomical locations of lymph nodes differs between these two maps especially with respect to nodes located in the paratracheal, tracheobronchial angle, and subcarinal areas. Carcinomas of the lung arise either from the alveolar lining cells of the pulmonary parenchyma or from the mucosa of the tracheobronchial tree. The trachea, which lies in the middle mediastinum, divides into the right and left main bronchi, which extend into the right and left lungs, respectively. The bronchi then subdivide into the lobar bronchi in the upper, middle, and lower lobes on the right and the upper and lower lobes on the left. The inside of the chest cavity is lined by a similar membrane called the parietal pleura.

Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Medullary carcinoma of the thyroid: a study of the clinical features and prognostic factors in 161 patients. Implications of prognostic factors and risk groups in the management of differentiated thyroid cancer. Prognostic factors and risk group analysis in follicular carcinoma of the thyroid. Risk group stratification and prognostic factors in papillary carcinoma of the thyroid. Prognostic indicators of outcomes in patients with distant metastases from differentiated thyroid carcinoma. Tumor of any size extending beyond the thyroid capsule to invade subcutaneous soft tissues, larynx, trachea, esophagus, or recurrent laryngeal nerve Very advanced disease. Approximately two-thirds of these lesions arise in the nasal cavity and paranasal sinuses; one quarter are found in the oral cavity and the remainder occur only sporadically in other mucosal sites of the head and neck. To reflect this aggressive behavior, primary cancers limited to the mucosa are considered T3 lesions. Mucosal Melanoma of the Head and Neck 97 In order to view this proof accurately, the Overprint Preview Option must be set to Always in Acrobat Professional or Adobe Reader. The anatomic extent criteria to define moderately advanced (T4a) and very advanced (T4b) disease are given below. For a description of anatomy, refer to the appropriate anatomic site chapter based on the location of the mucosal melanoma. For the rules for classification, refer to the appropriate anatomic site chapter based on the location of the mucosal melanoma. Esophagus and Esophagogastric Junction 103 In order to view this proof accurately, the Overprint Preview Option must be set to Always in Acrobat Professional or Adobe Reader. In contrast, this revision is data driven, based on a risk-adjusted randomsurvival-forest analysis of worldwide data. The previous system was neither consistent with these data nor biologically plausible. Some explanations for the discrepancy relate to the interplay among T, N, and M, histopathologic type, biologic activity of the tumor (histologic grade), and location. The unique lymphatic anatomy of the esophagus links N to T, permitting lymph node metastases from superficial cancers (pT1); this renders prognosis similar to that of more advanced (higher pT) N0 cancers. Similarly, advanced cancers (higher pT) with a few positive nodes may have a similar prognosis to those of less advanced cancers (lower pT) with more positive nodes. Previous staging recommendations ignored histopathologic type, but availability of data on a large mixture of adenocarcinoma and squamous cell carcinomas from around the world has permitted assessing the association of histopathologic type with survival. Although at first glance these multiple trade-offs seem to create a less orderly arrangement of cancer classifications within and among stage groupings compared with previous stage groupings, when viewed from the perspective of the interplay of these important prognostic factors, the new staging system becomes biologically compelling and consistent with a number of other cancers. In addition, patients undergoing surgery alone with pT4 and pM1 cancers represent a select population; placing them into stage groups, therefore, required either combining some classifications or using literature as a supplement. Patients with cervical esophageal cancer, sometimes treated as a head-andneck tumor, were also poorly represented. The location of the primary tumor is defined by the position of the upper end of the cancer in the esophagus. This is best expressed as the distance from the incisors to the proximal edge of the tumor and conventionally by its location within broad regions of the esophagus. It also arbitrarily divides the esophagus into equal thirds: upper, middle, and lower (Table 10. However, clinical importance of primary site of esophageal cancer is less related to its position in the esophagus than to its relation to adjacent structures (Figure 10.

Vascularized fibular grafts in the treatment of congenital pseudarthrosis of the tiba. Congenital tibial bowing Congenital tibial bowing comprises a spectrum of disorders with significant differences in both aetiology and prognosis for the different types (Crawford and Schorry, 1999). Posteromedial tibial bowing is a relatively benign condition which usually resolves spontaneously as the child grows. However, the leg may end up shorter than normal, requiring epiphysiodesis on the opposite side or limb lengthening to counteract the limb length inequality. Anteromedial bowing is almost always associated with fibular deficiency and congenital defects of the foot, or some type of femoral dysplasia. Knowing the cell line from which the tumour has sprung may help with both diagnosis and planning of treatment. There are, however, pitfalls in this approach: Tumours, tumour-like lesions and cysts are considered together, partly because their clinical presentation and management are similar and partly because the definitive classification of bone tumours is still evolving and some disorders may yet move from one category to another. Benign lesions are quite common, primary malignant ones rare; yet so often do they mimic each other, and so critical are the decisions on treatment, that a working knowledge of all the important conditions is necessary. Chondromyxoid fibroma Malignant Osteosarcoma: central peripheral parosteal Chondrosarcoma: central peripheral juxtacortical clear-cell mesenchymal Fibrosarcoma Cartilage forming Fibrous tissue Mixed Giant-cell tumours Marrow tumours Vascular tissue Fibroma Fibromatosis Suspicion is aroused if the injury was slight; in elderly people, whose bones usually fracture at the cortico-cancellous junctions, any break in the mid-shaft should be regarded as pathological until proved otherwise. Swelling is sometimes diffuse, and the overlying skin warm and inflamed; it can be difficult to distinguish a tumour from infection or a haematoma. If the tumour is near a joint there may be an effusion and/or limitation of movement. Spinal lesions, whether benign or malignant, often cause muscle spasm and back stiffness, or a painful scoliosis. The examination will focus on the symptomatic part, but it should include the area of lymphatic drainage and, often, the pelvis, abdomen, chest and spine. Patients may be completely asymptomatic until the abnormality is discovered on x-ray. Malignant tumours, too, may remain silent if they are slow-growing and situated where there is room for inconspicuous expansion. Chondrosarcoma and fibrosarcoma typically occur in older people (fourth or sixth decades); and myeloma, the commonest of all primary malignant bone tumours, is seldom seen before the sixth decade. In patients over 70 years of age, metastatic bone lesions are more common than all primary tumours together. Pain is a common complaint and gives little indication of the nature of the lesion; however, progressive and unremitting pain is a sinister symptom. It may be caused by rapid expansion with stretching of surrounding tissues, central haemorrhage or degeneration in the tumour, or an incipient pathological fracture. However, even a tiny lesion may be very painful if it is encapsulated in dense bone. Often, though, patients seek advice only when a mass becomes painful or continues to grow. A history of trauma is offered so frequently that it cannot be dismissed as having no significance. Yet, whether the injury initiates a pathological change or merely draws attention to what is already there remains unanswered. Neurological symptoms (paraesthesiae or numbness) may be caused by pressure upon or stretching of a peripheral nerve. Progressive dysfunction is more ominous and suggests invasion by an aggressive tumour. Stippled calcification inside a cystic area is characteristic of cartilage tumours. Look carefully at the bone surfaces: periosteal newbone formation and extension of the tumour into the soft tissues are suggestive of malignant change. For all its informative detail, the x-ray alone can seldom be relied on for a definitive diagnosis. With some notable exceptions, in which the appearances are pathognomonic (osteochondroma, non-ossifying fibroma, osteoid osteoma), further investigations will be needed. It may also reveal suspected lesions in inaccessible sites, like the spine or pelvis; and it is a reliable method of detecting pulmonary metastases.
Surveillance for Stage I non-seminomatous germ cell tumours of the testis: the optimal protocol has not yet been defined. Treatment of disseminated germ-cell tumors with cisplatin, bleomycin and either vinblastine or etposide. Nearly all malignant tumors are carcinomas arising from the renal tubular epithelium or, less frequently, from the renal pelvis (see Chap. The majority of kidney tumors are now being detected incidentally in asymptomatic individuals. Common sites of metastasis include the lungs, lymph nodes, liver, bone, and brain. Staging depends on the size of the primary tumor, invasion of adjacent structures, and vascular extension. The rationale for division of T2 into T2a (>7 cm but not more than 10 cm) and T2b (>10 cm) is based on large retrospective cohort studies with extended follow-up that demonstrate substantially different outcomes for these subgroups. Multiple studies have documented a poor prognosis for patients with ipsilateral adrenal involvement similar to patients with T4 or M1 disease, and these tumors are now reclassified to reflect current concepts about likely mechanisms of spread. In contrast, tumors with isolated renal vein thrombus are known to have a relatively favorable prognosis and are now Kidney 479 In order to view this proof accurately, the Overprint Preview Option must be set to Always in Acrobat Professional or Adobe Reader. Job Name: - /381449t of sarcomatoid features, the presence/absence of lymphovascular invasion, and the presence/absence of necrosis. Each papilla opens in the minor calices; these in turn unite in the major calices and drain into the renal pelvis. Lymph nodes outside of these templates should be considered distal (metastatic) rather than regional. Finally, nodal involvement is now consolidated as N1 since most studies suggest a relatively poor prognosis with any extent of nodal involvement. Recent data also demonstrate that multiple adverse features can act in a collaborative manner to further worsen the prognosis and emerging algorithms are incorporating all of these parameters. These adverse features include perirenal fat invasion, tumor size as a continuous variable, size of the largest involved lymph node, and extranodal extension. In addition, there are a number of potential molecular prognostic factors including genetic variables, proliferative markers, angiogenic parameters, growth factors and receptor, and adhesion molecules. Ideally future staging protocols would capture this information to facilitate individualized counseling and foster further progress in this field. Specific factors to be examined include degree of invasion, the presence/level of venous involvement, the presence and type of adrenal gland involvement, the type of grading system employed and grade determined, the presence/absence Metastatic Sites. Common metastatic sites include the bone, liver, lung, brain, and distant lymph nodes. The National Cancer Data Base findings regard- ing impact of size on T2 category on all-cause mortality and observed survival Size (cm) 4. The pathologic specimen should be processed in such a fashion as to allow for full pathologic assessment. Perinephric and perisinus fat should be left intact and sectioned in such a manner that allows for careful evaluation of these regions and they should be defined independently. Recent studies suggest a worse prognosis with perisinus fat invasion that may be related to increased access to lymphatic and vascular structures. For specimens for partial nephrectomy, the margins should be evaluated from at least two sections and should include the renal sinus for central tumors. Integrated algorithms that incorporate these factors have been validated and have been shown to improve prognostication over anatomic tumor stage alone. The use of these instruments for estimating prognosis and patient counseling can aid in decision-making. Clinical examination, abdominal computed tomography scanning, and other appropriate imaging techniques are required for assessment of the primary tumor and its extensions, both local and distant. Evaluation for distant metastasis should be done by laboratory biochemical studies, chest radiographs, and if clinically indicated, additional studies. Careful assessment of the adrenal gland and regional lymph nodes is recommended with resection on a selective basis.
References:




