Good management encompasses educating the patient about the disease and treatment, ensuring medication adherence, titrating dosage to assure clinical well-being, and monitoring treatment response. Pharmacists can make a dramatic difference in treatment success by educating the patient and monitoring adherence. Pharmacists are well positioned to correct therapeutic inadequacies by identifying and managing common factors that affect drug availability, such as drug interactions, effects of common comorbid conditions, timing of administration, and consistency of drug formulation. In addition, all faculty are expected to openly disclose any offlabel, experimental, or investigational use of drugs or devices discussed in this activity. The faculty and planning committee have been advised that this activity must be free from commercial bias, and based upon all the available scientifically rigorous data from research that conforms to accepted standards of experimental design, data collection, and analysis. The Planning Committee for this activity included Ruth Cohen and Margaret Inman of Continuing Education Alliance. The members of the Planning Committee have no significant relationships to disclose. Acknowledgment: the author wishes to acknowledge Katherine Salay, PharmD Candidate, for providing technical assistance. How to Receive Credit: Accreditation Continuing Education Alliance is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. A certificate of credit will be automatically generated upon successful completion of the activity. No part of this publication may be reproduced or transmitted by any means, electronic or mechanical, or stored in any storage and retrieval system, without permission in writing from the publisher. False the fundamental effective pharmacologic treatment- replacement of thyroid hormones-has not changed in decades. VaryingPhysiologicLevothyroxine RequirementsAccordingtoPatientAgeand PregnancyStatus Patient Status Neonate Children 8-12 months Children 2-10 years Adolescents Adults Elderly persons Pregnant women Source: Reference 21. Desiccated thyroid contains T4 and T3; but the balance of T4 and T3 in nonhuman animals is not the same as that in humans. In addition, the amounts of T4 and T3 can vary in every batch of desiccated thyroid, making it more difficult to moderate blood levels. Finally, because desiccated thyroid pills have binders, they are not completely "natural. Levothyroxine is metabolized to the more biologically active T3 in target tissues. False Of patients treated with levothyroxine, 30% to 60% do not reach biochemical euthyroidism, that is, they are either undertreated or overtreated. In 43% of patients aged >65 years were overmedicated may women who are hypothyroid at the be at risk for adverse biochemically euthyroid while receivonset of pregnancy or who become ing levothyroxine. Patients who are under- or overmedicated may be at risk for adverse Levothyroxine is considered safe hyperthyroidism. Given that potential adherence, although most clinicians believe nonadherbenefits outweigh potential risks, the Endocrine ence is common. The requirement for high doses of levothyroxine should prompt suspicion that they may be a factor. Thyroiditis affects approximately 10% of patients with type 1 diabetes6 and can present a complex clinical picture. Amiodarone, an antiarrhythmic agent, contains 37% iodine by weight and may impair conversion of T4 to the highly active compound T3. Thyroid abnormalities have been noted in 14% to 18% of patients receiving long-term amiodarone therapy, although with lower doses (150-330 mg), the incidence of thyroid dysfunction is 3. The abnormalities range from abnormal thyroid function test findings to overt thyroid dysfunction, which manifest as thyrotoxicosis or hypothyroidism. Both conditions can develop in apparently normal thyroid glands or in glands with preexisting abnormalities. Additional data on this issue can be expected with publication of the results of an ongoing clinical study evaluating whether differences between levothyroxine formulations affect thyroid functioning. A recent survey of physicians who treat patients with hypothyroidism revealed abundant clinical evidence of product differences. Physician lack of awareness of the switch meant followup testing may not have been implemented. Most cases involved generic substitution for brand name levothyrox- Pharmacists are in an excellent position to educate the patient with thyroid dysfunction about the basics of thyroid physiology and pathophysiology. In particular, that means reinforcing the need to normalize thyroid hormone levels to maintain basic metabolic functioning.
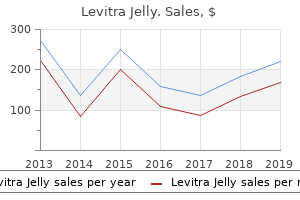
Purified Turpentine Oil (Turpentine Oil). Levitra Jelly.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96513
Furthermore, in other retrospective series, investigators failed to note a benefit from tonsillectomy. The macroscopic hematuria usually resolves spontaneously in a few days, but in some cases it can persist for several weeks. Kidney function usually, but not always, recovers completely after the disappearance of macroscopic hematuria. Kidney biopsies performed during an episode of macroscopic hematuria typically show mesangial proliferation and occasional segmental crescents. While some use crescents involving over 50% of glomeruli as the definition,551 others use the presence of incipient to fulminant cellular crescents, with or without segmental endocapillary proliferation in 410% of glomeruli. One anecdotal report indicated benefit in five patients using plasma exchange in a combination of immunosuppressive therapies. The three largest observational studies495,551,552 all concluded that immunosuppression is potentially useful. In another study, although an improved outcome was seen in those receiving immunosuppression, the conclusions were cautious, as the treated and untreated groups were not comparable. Recommended therapeutic regimens in these reports are varied, but initial therapy has usually included high-dose oral or i. Supplementary Table 48: Meta-analyses and systematic reviews on immunosuppression for IgA nephropathy. Supplementary Table 51: Meta-analyses and systematic reviews on immunosuppression for IgA nephropathy. Supplementary Table 61: Evidence profile of studies examining omega-3 fatty acid treatment in IgA nephropathy. Supplementary Table 62: Meta-analyses and systematic reviews on fish oil treatment in IgA nephropathy. Supplementary Table 65: Meta-analyses and systematic reviews on antiplatelet therapy for IgA nephropathy. It affects all ages, but 90% of cases are found in those less than 10 years of age, with the median age at presentation being 6 years. Ninety percent of children had developed kidney involvement by 8 weeks after acute presentation, while 97% developed kidney involvement by 6 months. Seven of 36 children (19%) in the prednisone group still had kidney involvement at 6 months compared to 15 of 35 (43%) in the placebo group. A prospective but uncontrolled study of 38 consecutive children with mean follow-up period of 5 years and 7 months showed resolution of severe nephritis (nephrotic syndrome and/or 450% crescents on biopsy) in 27 of 38 children treated with three pulses of methylprednisolone followed by oral prednisone for 4 months. Most children in their series of 20 patients were biopsied within 3 months, with a median of 30 days. Treatment with prednisone and azathioprine resulted in improvement in acuity score but not chronicity score. Therefore, treatment strategies at the time of presentation have been developed with the goal of preventing nephritis, or reducing the risk of severe persistent nephritis. Three of the five trials (568 patients) were well designed, placebocontrolled trials; exclusion of poor-quality studies from the 219 chapter 11 meta-analysis removed heterogeneity without altering the findings. The investigators commented that the small population size did not permit definitive conclusions. The kidney may also sustain damage by other mechanisms, such as thrombotic microangiopathy. The reported incidence of clinically important kidney disease in systemic lupus is about 38%. An active sediment includes hematuria, especially acanthocytes suggestive of glomerular bleeding, leukocyturia in the absence of infection, and red and white blood cell casts. Immunofluorescence and electron microscopy show significant subendothelial and mesangial immune deposits.
Molecular findings that provide these types of prognostic information or guide optimal initial/ongoing treatment decisions have the potential to significantly alter clinical management. Using an evidence-based approach to knowledge synthesis (systematic reviews, meta-analyses, and clinical practice guidelines) of data can also enable evidence-informed clinical practice. Barriers to dissemination and implementation of clinical practice guideline recommendations need to be overcome. Evidence-based guidelines may need to be formally adapted to various practice settings to enable their implementation. Important gaps in patientdirected knowledge translation have been recently identified by thyroid cancer patients and survivors (1060,1061). The development of plain language educational materials, including decision aids or other decision support tools would be helpful for use as adjuncts in physician counseling of patients about diagnostic and treatment options. In the case of relatively uncommon adverse effects of treatments, prospective surveillance research is also needed. Current methodologies for both Tg and anti-Tg antibodies remain problematic in many ways that hopefully will be overcome in the future. For Tg assays, these include interference with Tg measurement by the presence of anti-Tg and heterophile antibodies and the use of a host of different methods with varying results in terms of sensitivity or detection limits. While more ``ultrasensitive' Tg assays have been developed, we need to determine the true clinical significance or utility of measurable levels below 0. Competitive immunoassays have not provided an alternative in view of their unpredictability (771). In regard to anti-Tg antibodies, we need to better characterize the various epitopes of interfering antibodies to better understand their effect in different sera in order to interpret the associated spectrum of results obtained for measurable Tg. Authoritative bodies such as the National Academy of Clinical Biochemistry should consider mandating specific methodology rather than recommending general guidance. Yet, in the absence of these dissections, this is not the observed clinical locoregional recurrence rate for these patients. On the other hand, grossly involved metastatic lymph nodes were at one time minimally invaded by metastatic thyroid cancer. The challenge is to differentiate between low-volume metastatic disease that progresses with potential clinical consequences, and that which remains stable. To date, only one study has addressed this question, and no sonographic, pathologic, demographic, or molecular feature predicted outcome (849). Subsequently, randomized controlled interventional trials could be designed to address change in outcome, such as development of additional loco-regional disease, appearance of distant metastases, or disease-specific survival. Generally predicated upon identification of synergistic interactions in preclinical models, several studies are examining the question of whether therapy combining several agents may improve outcomes in thyroid cancer. Still other trials are focusing on novel nontraditional therapies, including engineered candidate virotherapeutics. Despite these large numbers of patients living with thyroid cancer, there is only a modest amount of peer-reviewed literature studying thyroid cancer survivors. There is very little information regarding the impact of the diagnosis itself or the effect of living with persistent disease such as Tg-positive, scan-negative thyroid cancer. A thoughtful and comprehensive analysis of thyroid cancer survivors will likely require both qualitative studies with in-depth interviews of survivors that will represent as many demographics of thyroid cancer patients as possible. Additionally, or as a next step, the development and/or utilization of a validated survey type instrument needs to be developed. This instrument would be designed to assess the quality of life of thyroid cancer survivors in a more quantitative manner, allowing for rigorous statistical analyses, and will help identifying areas to target that may improve the lives of thyroid cancer survivors (1072). Further research also needs to be performed in addressing patient and survivor care needs throughout the active treatment and survivorship trajectory, including issues such as identification and management of treatment-related side effects (1060,1061), psychosocial distress (1060,1061), persistent fatigue (1073,1074), financial impact (12), and cancer-related worry (1075). Sharleene Cano, Assistant to the Taskforce, for their constant help and support, as well as Ms. Vicki Wright (Division of Endocrinology, University of Colorado School of Medicine) for her assistance in manuscript preparation. He is a consultant for Veracyte, Exelixis, Bayer, AstraZeneca, Eisai, Genzyme, Novo Nordisk, and Eli Lilly.

These toxicities are much less common that those associated with percutaneous treatment modalities. Concerning bone lesions, radiotherapy plays an important role because it can complement surgery in case of incomplete resection or be used alone for pain relief or palliation. However, the major limitation of radiotherapy in spine lesions is the cumulative dose to the spinal cord. Spinal myelopathy or vertebral fractures are the most important side effects, especially in case of large-volume lesions. A multicenter prospective trial on 183 lung metastases from cancer other than colorectal showed a complete response rate of 88% at 1 year and an overall survival of 92% and 64% at 1 year and at 2 years, respectively (1022). Cases of delayed recurrence have also been reported, and long-term follow-up is needed. Furthermore, repeated treatments can be performed on the same lesion and multiple lesions can be treated in the same patient. Local disease control was achieved in the few reported cases of lung and bone metastases from thyroid cancer treated by thermal ablation (883,1016,1025). The association of cryoablation and cementoplasty seems promising in purely lytic bone metastases from thyroid cancer. Published experience using thermal ablation and stereotactic radiation in thyroid cancer patients is limited, and recommendations are currently based on more robust evidence in other solid tumors. Randomized prospective studies comparing the efficacy and tolerability of these different techniques are lacking, and their choice in clinical practice is based on local experience, lesion location as well as patient status and preference. Stereotactic radiation therapy is preferred to whole-brain radiation because life expectancy in patients with brain metastases may be prolonged, and stereotactic radiation induces less short- and long-term toxicity compared with whole-brain radiation (fatigue, headache, cognitive decline, and behavioral changes), and it may be effective even in patients with multiple brain lesions. The reasons for this association are unclear, but there is no evidence to suggest that trial participation is deleterious to patient outcomes, and it may be beneficial. Participation in a clinical trial should be considered in any situation wherein there exists no effective or proven standard of care, or when a standard of care is being compared with a promising new or investigational therapy. Adjuvant therapy trials may be appropriate for patients at high risk for disease recurrence following primary treatment who wish to pursue aggressive therapy. However, given the indolent nature of metastatic disease in most patients, therapeutic clinical trial participation should not be considered for patients with stable, asymptomatic metastatic disease unless agents with significant likelihood of complete remission, prolongation of survival, or biologic impact such as redifferentiation that could sensitize to definitive therapy are available (see section [C37]). Clinicians considering referral of patients for trials should review available treatment options and eligibility criteria, preferably through discussions with trial center personnel and review of trial materials at the website A broad variety of such trials may exist at any given time, which can generally be identified through online databases such as Benefit has been demonstrated in the form of improved progression-free survival (delay in time to disease progression or death) in three randomized, doubleblinded, placebo-controlled clinical trials: vandetanib (1033), sorafenib (1013), and lenvatinib (1034). However, randomized clinical trial data are not yet available to address many additional critical questions, including effects of systemic therapies of various types on survival and quality of life, or to address critical issues of optimal patient selection/inclusion/exclusion criteria for therapy and duration of treatment. Consequently, therapeutic decisions are presently based upon the convergence of expert opinion and patient preference/philosophy, thus emphasizing the critical need to address the above questions definitively through clinical trials. As a guide, evidence-based recommendations with expert consensus have been recently published (953). Although more ``novel' approaches have attracted attention recently, it is important to optimally apply fundamental approaches. Also important is the consideration of alternatives to the use of systemic therapy, such as the application of surgery or other localized approaches (including radiation therapy or thermal ablation approaches). It is also critically important to ensure that the disease prompting therapy represents metastatic thyroid cancer. In particular, because pulmonary nodules attributable to benign causes are common, the presence of pulmonary nodules does not in and of itself justify the application of systemic therapy. Thus, in cases of diagnostic uncertainty in which the result would have definitive therapeutic implications, biopsy is required, especially when Tg levels are low/unhelpful (such as in the presence of anti-Tg antibodies).

Poverty, poor transport infrastructure and geographic isolation all contribute to inadequate long term management of patients with thyroid cancer in many developing countries. Continuing education of physicians is required in order to instigate appropriate management algorithms. In turn, the physicians need to promote education of the general public and dispel misinformation, so that patients will seek appropriate medical help as early as possible. In many countries cultural factors may also inhibit appropriate management of thyroid cancer. Patients may seek traditional family therapies as alternatives to modern medicine, and due to lack of information, may fear modern medical equipment and techniques. In addition to patient and physician education, there exists a need for the establishment of data registries in many countries. Even with the introduction of new equipment and staff, unless data is collected that accurately reflects the impact, or otherwise, of any change, the true benefit of change cannot be assessed. Such data is also a powerful tool for use at administrative and government levels in order to argue the benefit for ongoing financial support, or the need for additional support. This review of the experience related from various countries around the world offers insight as to the effectiveness of information networks related to the availability of information technology, and groups and societies whose goals are for the optimal management of as many patients as possible. However, this review indicates that there is much potential for improvement, and also that an inertia of knowledge growth has developed that should provide us with optimism for the future. The long term follow-up studies of external radiation-exposed victims of Hiroshima and Nagasaki have indicated the elevated risk of thyroid cancer during the lifespan of exposed individuals. Furthermore, the dramatic increase of childhood thyroid cancer around Chernobyl has changed conventional concept and understandings of the mechanism of radiation-induced thyroid carcinogenesis. The genes subject to mutations in thyroid carcinogenesis can be classified as oncogenes or anti-oncogenes (tumour suppressor genes) based on their mode of action. Some genetic changes leading to thyroid cancer are inherited through the germline, but most are acquired or somatic in nature. Here the molecular genetics of human thyroid cancer is summarized from the standpoint of genetic factors and environmental status. Especially discussed is the molecular mechanism of radiation-induced thyroid carcinogenesis. Most oncogenes appear to be closely related to normal growth factors, genes that control cell division or to hormone receptors [18. In general, these genes, when turned on, promote cell growth, division and depress differentiation. Typically, activation of one such gene may not be enough to produce malignancy, but if accompanied by the expression of another oncogene, or if gene mutation or reduplication occurs, the cell may progress towards the transformation. The escape mechanism from cell apoptosis is also critical for abnormal cell proliferation. The genetic and chromosomal instability subsequently also occurs during the development of thyroid cancer. Recently mutations of thyroid hormone receptors have been reported in human thyroid cancer tissues, suggesting the up-regulation mechanism of c-myc at the transcriptional level [18. Activating mutations of H-ras at codons 12, 13, and 61 and overexpression of H-ras, are found in adenomas and carcinomas, but H-ras mutations are also found in nodular goitre tissue, suggesting that H-ras mutations could be an early event in oncogenesis [18. Enhanced sensitivity to apoptosis in ras-transformed thyroid cells may suggest the complexity of intracellular signal transduction during the early stage of thyroid oncogenesis [18. Another important oncogene is frequently and specifically expressed in papillary thyroid cancers. These mutations affect extracellular loops of the transmembrane domain and the transmembrane segments, and are proven to induce hyperfunction by transfection studies. Anti-oncogenes Compared to oncogene activation, second mechanism of thyroid carcinogenesis arises from inactivating mutations in genes that normally serve to limit cell proliferation. In general, single functional copy of antioncogene is sufficient to provide normal physiologic effects. The occurrence of tumour-specific suppressor genes is often detected by the lack of heterozygosity of chromosomal markers associated with deletions of segments of genetic material. Thus, evidence for characteristic chromosomal abnormalities within tumour cells may lead to recognition of a tumour suppressor gene. Mutation or deletion of the p53 tumour suppressor gene is found in only few differentiated thyroid cancers, but in many undifferentiated cancers, suggesting that this genetic deletion may be one of the final steps leading to anaplastic thyroid cancer growth [18. The involvement of cell cycle regulators remains to be further clarified at the standpoint of tumour suppressor gene during thyroid oncogenesis.

This also has the effect of reducing the remnant activity in the straw and container. Capsules have far fewer problems, but the patient must be told to swallow the capsule, and not to chew it. All steps in the administration process should be checked independently by a knowledgeable person to minimize the risk of errors. Finally, the treatment room, and all items used in the administration, must be checked for contamination, and any necessary warning signs put in place (see later). Contaminated items must be either disposed of correctly and safely, or stored until sufficient radioactive decay has taken place. On a routine check the following day, extremely high activity is noted in the waste bin. It is subsequently determined that the patient did not swallow the capsule, but hid it in the back of her mouth, chewing it when the staff had left, during her meal. This transferred much of the activity to the disposable cutlery and crockery, and napkin. Possible acute side-effects There is a range of possible side-effects which may become apparent within a few hours or days of administration. The medical and nursing staff involved must be aware of these, and how to deal with them if necessary. Gastric As patients already have very low levels of circulating thyroxine, they may feel generally unwell. When this is combined with anxiety related to the disease and treatment, and a low level of radiation sickness, it can lead to vomiting in the first 24 hours or so. This can be a serious radiation contamination problem, and should be avoided if at all possible. Many centres prescribe a prophylactic anti-emetic such as metoclopromide, administered shortly before the radioiodine is taken. It is not however completely effective in all cases and local procedures must be prepared to deal with contaminated vomit. If vomiting occurs within the first few hours, the vomit can contain a high proportion of the administered activity, especially if a capsule was used. Salivary glands Again, the radiation can induce sialitis (or sialadenitis) - a relatively frequent acute effect - in the first day or two. It is best relieved by encouraging the patient to stimulate saliva production by chewing or sucking sweets. More rarely, there may be long term effects such as pain, dryness of mouth or even more rarely, development of nodules. These may only be related to high cumulative absorbed doses from multiple treatments. Thyroid/Trachea If there is a significant amount of thyroid tissue remaining, thyroiditis and associated oedema can occur, with possible tracheal compression. If it occurs, this can be a serious complication which must be dealt with quickly. Excretory pathways Radioiodine will be excreted from the patient primarily by the kidneys, and consequently, the patient should be encouraged to drink freely to minimize dose to kidneys, bladder and gonads. Because of the lack of thyroid tissue, a great majority of the administered activity will appear in the urine. In most cases, 50-60% of the administered activity is excreted in the first 24 hours, and around 85% over a stay of 4-5 days [12. This will manifest in contamination of eating and drinking utensils, and pillow coverings (due to saliva excretion during sleep). The proportion of each (apart from urine) will vary widely, so it is best to assume that all forms of contamination are present, until proved otherwise. Radiation monitoring and radiation safety precautions the patient the patient should be identified as receiving radioiodine treatment by means of a wristband, a clearly visible notice in their medical record, a sign on their bed, a sign on the bedroom door (see 6. The wristband and medical record entry must include at least the radionuclide, activity administered, and date of administration. From the time of administration to discharge, the radiation levels emitted by the patient must be regularly checked. Many countries have prescribed or derived limits of retained activity before discharge of the patient can occur. However, the ultimate purpose of such recommendations is that prescribed dose limits for members of the public and dose constraints for caregivers are not exceeded.
Syndromes
Systemic signs such as fever and lack of appetite and sub acute (minor alterations in the milk and the affected quarter such as clots, flakes or discoloured secretion. The quarter may also be slightly swollen and tender (Philpot and Nickerson, 2000). Batu is located in the East Shoa Zone of the Oromia National state about 163 kilometres away from Addis Ababa. The rainfall is bimodal unevenly distributed with an average annual rainfall of 761mm. Monthly temperature variation is highly depend on rainfall, due to its location close to the equator and the seasons are only distinguished by the intensity of rain, which is the most in August and the least in December. The soil is fine sandy, loam with sand, silt clay in proportion of 34:48:18% respectively. Dairy cows were kept as source of milk and yoghurt for the town and kept by larger dairy farms and smallholder farms. All the cows in this study are hand milked and most of them milked two times a day during lactation period. The sample size was determined based on the formula given by Thrusfield (2007) considering 5% absolute precision, 95% level of significance and expected prevalence of 20%. Study Design: A cross- sectional study was carried out to determine the prevalence of Streptococcus uberis in bovine mastitis from December 2014 to April 2015 at cow and quarter level. Based on clinical manifestations for clinical mastitis and indirect test (California mastitis test and Culture) for sub clinical mastitis; Questionnaires and direct observations of the farms were used to collect information regarding the risk factors used in the analyses. Microbial isolation and in-vitro antibiotic susceptibility test using seven antimicrobial discs. Data Collection: A questionnaire was developed and pretested, and all information relating to the study objectives was recorded. Relevant information was collected on cow history, housing system, milking practice, drug usage and other management practices. Risk factors considered were breed, age, parity, stage of lactation and floor type. The universal bottle were labelled, then put in ice containing icebox and transported immediately to the Addis Ababa University College of veterinary medicine and agriculture. For primary identification, colony size, shape, colour, haemolytic characteristics and Grams reaction. Since Streptococcus uberis is fastidious bacteria it does not grow on nutrient agar as other bacteria grown. The gram stained smears from typical colonies that showed gram positive cocci occurring in long chain were taken as presumptive Streptococcus uberis (Quinn et al. Catalase test: Pure culture of the isolates were picked using a sterile loop from the agar and mixed with a drop of 3% H2O2 on a clean glass slide. If the organism was catalase positive, bubbles of oxygen were liberated within a few seconds and catalase negative isolates did not produce bubbles. The catalase negative cocci were considered as Streptococci (Quinn, 2004) (Table 6). Oxidation and fermentation test: Uninoculated media is green in colour and semisolid, when the bacteria was inoculated it change to yellow due production of acid by fermentation of glucose in the media. Streptococcus are fermentative bacteria, both sealed and open test tube were changed to yellow (Quinn, 2004).
Fever: Acetaminophen or ibuprofen may be given if your child has a fever over 101. How You Get Strep Throat Strep throat is an infection in the throat and tonsils caused by group A Streptococcus bacteria (called "group A strep"). A strep test (throat swab) is needed to tell if your child has strep throat; just looking at their throat is not enough to make a diagnosis. If the strep culture is positive, a prescription for antibiotics will be necessary. Once treatment begins, your child should start feeling better within a day or two. Children with strep throat should stay home from school or daycare until they have taken antibiotics for at least 24 hours. Antibiotics will be effective against strep if given even 1 week after the start of symptoms. Group A Streptococcus (strep) is a contagious bacterial infection that causes fever, sudden onset of a sore throat, swollen tonsils and painful swallowing. Strep throat accounts for 15 - 30% of all sore throats in children ages 5 to 15 Diagnosis and treatment If a throat swab tests positive for group A strep bacteria, your child will likely receive a 10-day course of oral antibiotics. To reduce the risk of complications, it is important to complete the entire course of antibiotics as prescribed. Limit close contact with people who are sick and wash your hands frequently with soap and water or alcohol-based sanitizer. Strep carriers are less likely to be contagious and most will not require treatment. The treatment of strep throat can prevent some rare but serious complications such as rheumatic fever (a disease that affects the heart) or spread of the strep infection to other areas of the body. In addition, with treatment the fever and much of the sore throat are usually gone within 24 hours. If the medicine is a liquid, store the antibiotic at the recommended temperature and use a medication measurer to be sure that you give the right amount. Even though your child will feel better in a few days, give all the antibiotic doses to keep the strep throat from flaring up again. A long-acting penicillin (Bicillin) injection is another option if your child refuses oral medicines or if it will be impossible for you to give the oral medicine regularly. If taken correctly, the oral penicillin works just as rapidly and effectively as a shot. Give your child acetaminophen (Tylenol) or ibuprofen (Motrin, Advil) if he has a fever over 102 degrees F (39 degrees C) or a great deal of throat discomfort. Any child or adult who lives in your home and has fever, sore throat, headache, or vomiting in the next week should be evaluated. In fact, one theory supposes that certain individuals are genetically more susceptible to strep and catch it more easily. Another theory proposes that some of the bacteria normally present in the throat help the strep to survive by inactivating the antibiotic drug. This presents a problem for the carrier, because every sore throat will have a positive culture- even when it is not a strep throat and is caused by a virus. Thus, when a child has many positive throat cultures, we will often check to see if he or she is a carrier. If this is the case, special medication may be used to try to rid the child of the strep. While family members should not share toothbrushes, a person with strep does not need to discard his own. Removing the tonsils greatly reduces (but does not eliminate) the chances of getting strep throat. Tonsillectomy is performed by an ear nose and throat specialist under general anesthesia.
Rates of short-term adverse effects may be higher after administration of 100 mCi 131I compared to 30 mCi, in a small number of trials examining these outcomes. The absolute disease-specific survival remained high even in the patients receiving lower administered activities of 131I, and there were no differences in overall survival in these older patients. However, there were some statistically significant differences between the treatment groups that may have influenced these results, including higher numbers of men and individuals with lateral neck nodal disease and a longer follow-up period (which may increase the rate of detection) in the higher administered activity group of this study (723). In this study, no recurrences were noted in either group after a median follow-up of 7. Although the mean primary tumor size was higher in the group treated with higher activities compared with the lower activity group in this study ( p < 0. In this study, the respective rates of disease recurrence, mortality, and stimulated Tg >2 ng/mL were not significantly different in the lower administered activity group (i. In another study comparing rates of disease structural recurrence/persistence in 181 patients with positive N1b lymph nodes, Sabra et al. Such findings may suggest, however, that the routine measurement of urinary iodine excretion, outside of possibly a research setting or suspected iodine contamination, may not be necessary. In a comparison of the results of pretherapy 131 I scans to posttherapy scans, the rate of newly discovered lesions on posttherapy scans was reported to be between 6% and 13%. In older literature, it had been reported that posttherapy scanning demonstrated new findings in 31% of 39 cases studied, but the detection of thyroid foci was included in that outcome, whereas almost a third of the patients (12 of 39) had a sizeable portion of their thyroid remaining following primary surgery (736). The authors of this study reported that the concordance of lesions detected on both scans was 80. A limitation in interpreting the posttherapy scan literature is that all of the lesions identified on posttherapy scans were not always confirmed to represent structural disease (i. Similar recommendations hold for low-risk patients who have not undergone remnant ablation, although serum Tg levels may be measurably higher and continued surveillance for recurrence applies. The 10-year cause-specific and disease-specific survivals were not different between the patients who underwent thyroidectomy versus a lesser operation, although it was common for the patients undergoing lobectomy to also receive an ipsilateral central neck dissection. The approach to patients with gross incomplete surgical resection of disease is addressed in another section (Recommendation 72). Doxorubicin may act as a radiation sensitizer in some tumors of thyroid origin (760) and could be considered for patients with locally advanced disease undergoing external beam radiation therapy. In particular, the use of radiation therapy within the context of initial/primary surgery/thyroidectomy has no meaningful literature support. There are reports of responses among patients with locally advanced disease (756,757) and improved relapsefree and cause-specific survival in patients over age 60 with extrathyroidal extension but no gross residual disease (758), and selective use can be considered in these patients. In such contexts, the risks of anticipated additional serial re-operations Accurate surveillance for possible recurrence in patients thought to be free of disease is a major goal of long-term follow-up. Tests with high specificity allow identification of patients unlikely to experience disease recurrence, so that less aggressive management strategies can be used that may be more cost effective and safe. Similarly, patients with a higher risk of recurrence are monitored more aggressively because it is believed that early detection of recurrent disease offers the best opportunity for effective treatment. A large study (761) found that the residual life span in disease-free patients treated with total or near-total thyroidectomy, 131I for remnant ablation, and in some cases high-dose 131I for residual disease was similar to that in the general Dutch population. In contrast, the life expectancy for patients with persistent disease was reduced to 60% of that in the general population but varied widely depending upon tumor features. Age was not a factor in disease-specific mortality in a comparison of patients with age-matched individuals in the Dutch population. Patients with persistent or recurrent disease are offered treatment to cure or to delay future morbidity or mortality. In the absence of such options, therapies to palliate by substantially reducing tumor burden or preventing tumor growth are utilized, with special attention paid to tumors threatening critical structures. A second goal of long-term follow-up is to monitor thyroxine suppression or replacement therapy to avoid underreplacement or overly aggressive therapy (767).
Shatavari + Oestrogens or Oestrogen antagonists the interaction between shatavari and oestrogens or oestrogen antagonists is based on a prediction only. Shatavari + Miscellaneous Limited evidence suggests that shatavari increases the gastric emptying rate similarly to metoclopramide, which is known to decrease the absorption of atovaquone, digoxin and ketoprofen, and increase the absorption of ciclosporin, dantrolene, morphine Evidence, mechanism, importance and management Shatavari contains phytoestrogens and has been investigated in a variety of pharmacological and clinical studies for its effect on lactation, dysfunctional uterine bleeding, premenstrual syndrome and menopausal symptoms; this has been the subject of a review. Previous reports about its possible toxicity have been found to be because of contamination with Teucrium species; skullcap itself is now considered to be safe to use. Constituents the major active components of skullcap are the flavonoids scutellarin, scutellarein, baicalein, baicalin (the glucuronide of baicalein), dihydrobaicalin, apigenin, luteolin and other methoxyflavones. Pharmacokinetics No relevant pharmacokinetic data found for skullcap, but see flavonoids, page 186, for information on individual flavonoids present in the herb. Interactions overview No interactions with skullcap found, but for information on the interactions of individual flavonoids present in skullcap, see under flavonoids, page 186. Use and indications Skullcap has been used traditionally as a sedative and to treat S 355 Soya Glycine max (L. This highlights the problems of extrapolating the findings of in vitro studies to clinical situations. The pharmacokinetics of the isoflavone constituents of soya are further discussed under isoflavones, page 258. Constituents the isoflavones in soya beans consist mainly of genistein and daidzein, with smaller amounts of isoformononetin, ononin, glycetein, desmethyltexasin and others. They are present mainly as glycosides, and the amount varies between the different soya products. S Interactions overview Soya products may increase the metabolism of caffeine and reduce the absorption of levothyroxine. Potential interactions of isoflavone constituents of soya are covered under isoflavones; see antibacterials, page 260, nicotine, page 261, paclitaxel, page 261, tamoxifen, page 262, and theophylline, page 263. Clinical review: a critical evaluation of the role of soy protein and isoflavone supplementation in the control of plasma cholesterol concentrations. Nonhormonal therapies for menopausal hot flashes: systematic review and meta-analysis. Cassidy A, Albertazzi P, Lise Nielsen I, Hall W, Williamson G, Tetens I, Atkins S, Cross H, Manios Y, Wolk A, Steiner C, Branca F. Critical review of health effects of soyabean phyto-oestrogens in post-menopausal women. Use and indications Soya is a widely used food, particularly in Japanese and Chinese cuisine. Fermented products include soy sauce, natto and miso, and these can contain high concentrations of the isoflavones. There are numerous purported benefits of soya protein, the most well studied being possible reductions in hyperlipidaemia, menopausal symptoms and osteoporosis, and prevention of some cancers. Epidemiological studies suggest that a diet with a high intake of soya might protect against breast cancer. One paper notes that many of the demonstrable actions of isoflavones in soya are attributed to the aglycones genistein and daidzein; however, these occur in negligible amounts unless the product has been fermented. Despite numerous studies and meta-analyses, the health benefits of soya have not been conclusively proven and remain controversial. For the theoretical possibility that broadspectrum antibacterials might reduce the metabolism of the isoflavone constituents of soya, such as daidzein, by colonic bacteria, and so alter their efficacy, see Isoflavones + Antibacterials, page 260. Soya + Levothyroxine and related drugs Soya + Caffeine Soya products may increase the metabolism of caffeine. Clinical evidence Caffeine elimination is low in neonates, but increases faster in those receiving formula feeds (type not specified), than in breast-fed infants. Mechanism Neonates are less able to metabolise caffeine than adults: hepatic metabolism matures in the first year of life. Importance and management Clinical evidence in support of an interaction between soya and caffeine is limited, because the two studies do not state the formula feeds used, although it seems likely that soya feeds are implicated; this suggestion is supported by experimental evidence. In infants, caffeine is dosed individually, but be aware that required doses are likely to increase in those receiving formula feeds, including soyabased formula.
References:




