
The reported effectiveness of immunosuppressive treatment in C3G has been variable. Immunosuppression did not seem to reduce progression to kidney failure as compared to untreated individuals. The response to immune suppression seen in this retrospective cohort provided the support for the current expert opinion on treatment approach for C3G. Eculizumab normalized soluble C5b-9 level in all patients with elevated levels of this biomarker of terminal pathway activity at baseline, suggesting it may represent a potentially useful marker of response. In a recent retrospective study, 26 patients with C3G were treated with eculizumab for a median duration of 14 months. Of these, six patients (23%) had a global clinical response, six (23%) had a partial clinical response, and 14 (54%) had no response. These results are consistent with the fact that eculizumab mainly targets glomerular inflammation and has no or limited effect on the complement dysregulation that governs C3G. Diagnosis Small-vessel vasculitis encompasses a group of diseases characterized by necrotizing inflammation of small vessels. Patients with systemic vasculitis may present with extrarenal manifestations affecting one or several organ systems, with or without kidney involvement. Commonly involved systems are the upper and lower respiratory tract, skin, eyes, and the nervous system. Although several diseases can manifest as a pulmonary-renal syndrome, simultaneous lung and kidney injury should raise concern for vasculitis. In this situation, serological testing and interpretation are of great diagnostic importance. All treatment modalities should be available, including rituximab and plasma-exchange. The center should have experience with these treatment modalities and their complications. Finally, a center should have access to an intensive care unit and an acute hemodialysis facility. Kidney prognosis and treatment response Kidney histology is predictive of long-term risk of kidney failure; prognostic histologic scores have been developed. Importantly, kidney recovery can be seen in the face of advanced kidney damage, and induction treatment should not be withheld on the basis of unfavorable histologic findings. Assessing response of kidney vasculitis can be difficult in the presence of persistent hematuria and proteinuria, which are seen in 50% of patients. A stable or falling creatinine is a guide; control of extrarenal disease and normalization of inflammatory markers. Persisting proteinuria can reflect disease activity or chronic parenchymal damage from preceding inflammation. The significance of persisting hematuria is unclear, but a return of hematuria after initial resolution may indicate kidney relapse. Regarding the route of cyclophosphamide administration oral and intravenous, cyclophosphamide resulted in similar outcomes. With intravenous cyclophosphamide, a reduction of the total cyclophosphamide dosage is achieved compared to oral cyclophosphamide. Nevertheless, more patients tended to experience relapses after intravenous cyclophosphamide during long-term follow-up. The rate of reduction of corticosteroids varies between studies with some aiming for withdrawal by month five, while others continue between 5-10 mg/day after six months. Complement-targeted therapy might be another strategy to reduce glucocorticoid exposition. The critical outcome, all-cause mortality, was included; however, there were no cases reported. Effects on complete remission at six months, relapse rate, and serious adverse events are graded as moderate. The studies comparing continuous oral versus intravenous pulse cyclophosphamide were not blinded (participants and study personnel) (Table S35518, 530-532). Overall, the quality of evidence on the important endpoints complete remission and leukopenia is graded as 258 moderate because of study limitations. Other outcomes exhibited low quality of evidence because of serious imprecision due to very few events (relapse, all-cause mortality). The quality of the evidence was low for all critical outcomes due to imprecision, as there was only one study.
Do not use code 3 for positive immunophenotyping or genetic testing identifying a more specific histology when the test result is preceded by "patchy weak staining. Positive laboratory test/marker study this code is rarely used for Hematopoietic and Lymphoid neoplasms. If there no provisional diagnosis or clinical suspicion of cancer, immunophenotyping or genetic testing would not be done. Assign code 7 when the diagnosis is confirmed by radiology or other imaging techniques only. While clinical diagnosis is seldom used for solid tumors, it is a valid diagnostic method for certain hematopoietic neoplasms. For these neoplasms, the biopsy, immunophenotyping, and genetic testing do not confirm the neoplasm. There are some circumstances under which the information originally coded in the abstract should be updated. At the time of diagnosis a patient is diagnosed with liver metastasis but primary site cannot be determined and the abstract is submitted as an unknown primary. Change the primary site from 147 Texas Cancer Registry 2018/2019 Cancer Reporting Handbook Version 1. An abstract is submitted with the histology of cancer (8000/3) and diagnostic confirmation code 7. At a later admit the H&P states that the patient has squamous cell carcinoma of the lung diagnosed by fine needle aspiration. The Histology should be changed from cancer to squamous cell carcinoma (8070/3), and the Diagnostic Confirmation should be changed to 2, cytology. Explanation Text documentation is an essential component of a complete electronic abstract and is heavily utilized for quality control and special studies. Text is needed to justify coded values and to document supplemental information not transmitted within coded values. High-quality text documentation facilitates consolidation of information from multiple reporting sources at the central registry. The text field must contain a description that has been entered by the abstractor independently from the code(s). If cancer abstraction software generates text automatically from codes, the text cannot be utilized to check coded values and should not be generated electronically from coded values. Information documenting the disease process should be entered manually from the medical record. Staging should include all information available through completion of surgery(ies) in the first course of treatment or within 4 months of diagnosis in the absence of disease progression, whichever is longer. For text documentation that is continued from one text field to another, use asterisks or other symbols to indicate the connection with preceding text. Suggestions for Text Date(s) of procedure(s), including clinical procedures, which provided information for assigning stage; organs involved by direct extension Size of tumor, status of margins 150 Texas Cancer Registry 2018/2019 Cancer Reporting Handbook Version 1. Suggestions for text Date(s) and type(s) of X-ray/Scan(s) Primary site Histology (if given) Tumor location 151 Texas Cancer Registry 2018/2019 Cancer Reporting Handbook Version 1. Suggestions for Text Type of lab test/tissue specimen(s) Record both positive and negative findings; rcord positive test results first Information can include tumor markers, serum and urine electrophoresis, special studies, etc. Record any additional comments from the pathologist, including differential diagnoses considered and any ruled out or favored. Tumor size that is independent of stage is also useful for quality assurance efforts. Size measured on the surgical resection specimen, when surgery is administered as the first definitive treatment, i. If only a text report is available, use: final diagnosis, microscopic, or gross examination, in that order. If neoadjuvant therapy followed by surgery, do not record the size of the pathologic specimen. Code the largest size of tumor prior to neoadjuvant treatment; if unknown code size 999. If no surgical resection, then the largest measurement of the tumor from physical exam, imaging, or other diagnostic procedures priotr to any other form of treatment (See coding rules below) 4. If 1, 2, and 3 do not apply, the largest size from all information available within four months of the date of diagnosis, in the absence of disease progression.

The incidence of Listeria monocytogenes in slaughtered animals, in meat and in meat products in Yugoslavia. Viability of Escherichia coli O157:H7 in fermented semidry low-temperature-cooked beef summer sausage. Unsaturated solutions of sodium chloride as reference sources of water activity at various temperatures. Draft Assessment of the relative risk to public health from foodborne Listeria monocytogenes among selected categories of ready-to-eat foods. Occurrence, numbers, and growth of Listeria monocytogenes on some vacuum-packaged processed meats. Occurrence of Listeria infection in meat industrial raw-materials and end products. Contamination des viandes et des produits de charcuterie par Listeria monocytogenes en Haute-Vienne. Listeria monocytogenes, occurrence and significance in meat and meat products and experience with recommendations for its detection and assessment. Zum Vorkommen von Listeria monocytogenes in Fleisch und Fleischerzeugnissen einschliesslich Geflugelfleisch des Handels. Staphylococcus aureus and Escherichia coli in nham (Thaistyle fermented pork sausage). Listerienfunde in rohen fleischerzeugnissen [Listeria findings in raw meat products]. The incidence of Listeria in the production of cured and air-dried beef, salami and mettwurst. Incidence of Salmonella, Campylobacter jejuni, Campylobacter coli and Listeria monocytogenes in poultry carcasses and different types of poultry products for sale on the Belgian retail market. Fate of Escherichia coli O157:H7 in Chinese-style sausage during the drying step of the manufacturing process as affected by the drying condition and curing agent. Due to a paucity of data, cold-smoked fish consumption estimates were based on data describing global production of cold-smoked salmon. Various other sources of consumption estimates are also shown, and it is noted that the estimates from different sources are not completely consistent, which leads to uncertainty in the estimates. In Germany and Denmark, hot-smoked product constitutes only a negligible or very small proportion of smoked salmon consumption (P. Similarly, in Australia, hot-smoked salmon products constitute ~10% of production and consumption (Walsh, 1999). Conversely, the contribution of other types of cold-smoked fish is not included in the estimates. Recognizing this limitation, the data are nonetheless used as proxy values for total cold-smoked fish consumption. From that data, there are various approaches available to calculate the annual per-person consumption of cold-smoked fish and its variability and uncertainty. If the total population of the nations is considered against the total production, the average consumption is 90. Per capita consumption in individual nations appears to vary between 8 and 1000 g/person/year, with a median value of 138 g/consumer/year. The average of the estimates of national per-person annual consumption is, however, 231 g. This estimate 3 Globefish have published an updated report on Salmon - A Study of Global Supply and Demand (Globefish, 2003). This provides more recent data on national production and imports/exports of cold-smoked salmon. However, due to limited time and resources it was not possible to incorporate the more recent data into this risk assessment. If each national consumption estimate is weighted according to the population size, the global average is calculated to be 146 g. The difference between this and the original global estimates arises because data for Canada, Chile, Germany and West Germany, and Norway could not be used because one element of the needed data was missing; see Table A5. Production (P) (tonne) Australia Austria Belgium Canada Chile Denmark Denmark Faeroe islands France Germany W. From the same data source, differences among population sub-groups were revealed but are not used explicitly in this assessment. Using data for consumption of all smoked seafoods, there was no significant difference in serving size by geographical region (north or south Germany) or age group (more or less than 60 years).
Sample cleanup is a time-consuming step and usually consists of extraction with solvent, liquid-liquid partition, and/or chromatographic separation and determination. Recently, non-invasive analyses, such as near-infrared spectrometry, have been used, with limited success, for detecting the occurrence of A. Loci index for genomes Aspergillus flavus Aspergillus parasiticus Available from the GenBank Taxonomy database, which contains the names of all organisms that are represented in the genetic databases with at least one nucleotide or protein sequence. Molecular Structural Data: Aflatoxins B1, B2, G1, G2, and M1 Bad Bug Book Foodborne Pathogenic Microorganisms and Natural Toxins Gempylotoxin For Consumers: A Snapshot 1. Toxin Gempylotoxin is an indigestible wax, composed of C32, C34, C36, and C38 fatty acid esters, with the main component C34H66O2 (Ukishima, et al. Some consumers continue to eat these fish, despite the fact that they may have a purgative effect. This may be due to personal preference, or consumers may unwittingly eat these fish if the product is not identified as escolar or oilfish and is instead marketed under different names. For additional information on vernacular or misleading names used for these species, see the Sources section, below. The wax was composed of C32, C34, C36 and C38 compounds, and the main component was C34H66O2. The alcohol components were mainly C16:0 and C18:1, as well as those of sperm whale (Physeter catodon) wax. The fatty acid components were mainly C18:1 and smaller amounts of highly unsaturated fatty acids. In some people, eating even small amounts of these fish can cause oily diarrhea (orange or brownishgreen), abdominal cramps, nausea, vomiting, and headache. Usually, not much fluid is lost from the body with the diarrhea caused by these fish, and the symptoms generally go away in a day or two. To help protect yourself, buy your fish from a reputable market, to help ensure that the fish in the package really is what the label says it is. Onset: Symptoms have been reported to start between 1 and 90 hours after the fish is consumed, with a median onset of 2. Symptoms: Diarrhea, often consisting of an oily orange or brownish-green discharge (keriorrhoea), without major fluid loss; abdominal cramps; nausea; headache; and vomiting. Sources Symptoms usually are associated with ingestion of escolar (Lepidocybium flavobrunneum) or oilfish (Ruvettus pretiosus). Other products have been implicated in illness (including butterfish, rudderfish, walu, white tuna, and Taiwanese seabass). In most cases, these products were actually escolar or oilfish, but were marketed under inappropriate local or vernacular names, such as those used where the species was harvested. Species substitution or misbranding occurs when a deceptive and misleading name is used. Additional deep-sea fish species, such as orange roughy (Hoplostethus atlanticus) and oreo dory (Allocyttus spp. Improperly handled escolar and oilfish also have been associated with scombrotoxin (histamine) poisoning, the topic of a separate chapter of the Bad Bug Book. Diagnosis Diagnosis is per symptoms, particularly of oily, orange or greenish-brown diarrhea, and history of having consumed this type of fish. Food Analysis the following articles provide information relevant to food analysis of the oils containing high levels of indigestible wax esters in these fish, as well as methods for identification of those species. Rapid detection of oilfish and escolar in fish steaks: A tool to prevent keriorrhea episodes. Unusually high levels of non-saponifiable lipids in the fishes escolar and rudderfish: Identification by gas and thin-layer chromatography. Keriorrhoea - the passage of oil per rectum - after ingestion of marine wax esters. Wax components of escolar (Lepidocybium flavobrunneum) and its application to base of medicine and cosmetics. Examples of Outbreaks An outbreak that occurred in New South Wales, in October 2001, provides an example.

While in the Stirling County study the prevalence of psychiatric disorder, especially psychoneurotic symptoms, was considerably greater among women than men (65 percent versus 47 percent), in the Yoruba sample this pattern was reversed, although the sex difference was small (42 percent among males and 39 percent among females). The Yoruba group also showed a higher prevalence of psychiatric symptoms based primarily on organic disorder than the Stirling County population, a finding that was compatible with the greater amount of severe endemic disease and malnutrition in the Nigerian population. Another seminal community survey was carried out by Orley in the early 1970s (Orley and Wing, 1979) in two Ugandan villages, and its results were compared with those obtained in a survey conducted with the same methodology in a working-class area in southeast London (Camberwell) among 237 women. The brief form of the ninth edition of the Present State Examination was used, translated into the Luganda language, and all the interviews in the Ugandan villages were conducted in that language. The three major psychiatric illnesses detected were depression, hypomania, and anxiety states, and higher rates were found for all three diagnoses in the Ugandan villages. The highest rates were for depression-the Ugandan rates were twice as high as those in Camberwell, both at threshold and for more definite cases. There was no significant difference in the overall rate of disorders between the two sexes in the Ugandan sample; combining all cases at threshold level and above, according to the Index of Definition, 27 percent of the women and 24 percent of the men had psychiatric disorders. For comparison, 11 percent of the women surveyed in the London sample were cases at threshold level and above. A number of other community surveys of various sample sizes and employing methodologies with different degrees of sophistication have been carried out in other African countries, including Sudan (Baasher, 1961; Rahim and Cederblad, 1989) and Senegal (Beiser et al. The Senegal studies did not break down psychiatric morbidity rates by gender, and thus will not be discussed further. In Sudan, Baasher (1961) surveyed the inhabitants of a village with 1,860 residents. A team including a psychiatrist visited all households and interviewed family members in order to pick up any cases of mental disorders. The author points out that this result was the opposite of that found in a Khartoum clinic studied, where the ratio of males to females was 3:1. In the later study in Sudan, Rahim and Cederblad (1989) randomly selected 204 subjects between the ages of 22 and 35 from a newly urbanized part of Khartoum. Subjects were assessed using the Self-Reporting Questionnaire, the Eysenck Personality Inventory, and a Sudanese rating scale of anxiety and depression. In the Orley and Wing (1979) study, also cited above, there were approximately twice as many cases of depression in their Ugandan series as in the female sample from a London inner-suburb. In a later review of this topic, Jegede (1979) also noted a considerable frequency of depression among Africans and stressed the common somatic presentation of this disorder. It has already been noted that most epidemiologic investigations carried out in community samples in various sites, predominantly in industrialized countries, have found a remarkable difference in rates of depressive disorders between males and females. While one analysis of the Ugandan data showed a significant excess of women with depressive disorders, however, this was largely accounted for by the exclusion from that analysis of subjects over 65 years of age: four of the eight men over age 65 in the group had a depressive disorder, but none of the seven women did. Adding the four men to the "depressed" sample served to narrow the gender gap, although the predominance of depressive symptoms among women persisted. Beyond the results obtained in these two studies, we lack population-based data, which might help clarify the issue, although there is an accumulation of data gathered through clinic-based investigations. Unfortunately, the clinic-based results cannot be generalized to total populations because of the potential biases inherent in presenting samples, which can be extreme between the two sexes in any clinical setting. For instance, a study was conducted in Ghana among all patients showing depressive symptoms who contacted a psychiatric inpatient or outpatient service over a period of several weeks. Yet in a similar study conducted at the outpatient psychiatric clinic of a hospital in Addis Ababa over a period of three years, a slight excess of males over females (27 versus 25) was encountered (Keegstra, 1986). An investigation carried out in Kenya using methodology comparable to that used in studies in Britain (Brown and Harris, 1978) found that the group identified as depressed had experienced more life events in the 12 months preceding the onset of depression than the controls in that same period (Ndetei and Vadher, 1984; Vadher and Ndetei, 1981). These results are similar to those obtained by researchers in Western settings and underscore the centrality of this issue to any future study that purports to unravel the determinants of depression in African settings. As for manic disorder, one relatively large study looked at all patients presenting over a two-year period at the two psychiatric units of a teaching hospital in Nigeria who met the Research Diagnostic Criteria for manic disorder (Makanjuola, 1985). Although there was an excess of females in the group diagnosed with bipolar disorder compared with the groups with recurrent unipolar manic disorder or with a single manic episode, the difference was not statistically significant. Conversion hysteria and anxiety and panic disorders have also been studied in African settings, providing institutional statistics about the differential sex prevalence among psychiatric patients treated for these disorders and the various aspects of their phenomenology, determinants, and course (Awaritefe, 1988; Benjamin et al.
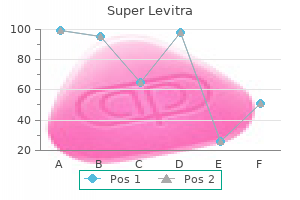
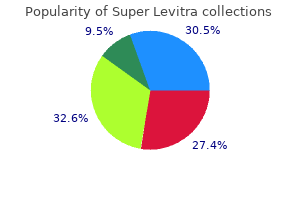
European Alder (Elderberry). Super Levitra.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96444
The chapter then briefly reviews what is known about injury patterns in the developing world. The life span perspective is employed, where possible, in the systematic evaluation of adverse health outcomes of injury across the female life span. Finally, public health research implications are drawn from a consideration of the information presented. It must be noted at the outset that substantial cross-national differences probably exist for most of what is covered in this chapter. The approach adopted will attempt to be as inclusive of such differences as possible in the hope that it will facilitate application of the variants discovered to future study of individual countries, or subpopulations within them. Although the "intent" of an injury is not always clear, classification by intent allows the identification of possible risk factors and the development of prevention strategies. Unintentional injuries are those caused by motor vehicles and other forms of transportation, drowning, poisoning, burns, or falls. Certain intentional injuries, such as rape, battering, sexual abuse, and domestic violence, affect females almost exclusively. Occupational injuries are the unintentional and intentional injuries that occur at work or traveling to and from a work setting. This belief has been changing, and significant progress is being made in both policy and prevention strategies. For instance, during the past decade, reductions in motor vehicle fatality rates, decreases in unintentional poisonings, and lowering rates of home fire fatalities have been realized in countries with injury prevention programs. In some countries the term "accident" is no longer used to describe an injury-producing event because of its connotation as something uncontrollable or random. There are a number of reasons why injury programs should be rapidly established in all countries. In developed countries, they account for more deaths in persons between the ages 1 and 44 than all infectious diseases combined. With the decreasing rates of childhood mortality and increased longevity observed in much of the Sub-Saharan region (see the Appendix), there is reason to expect that injuries will become an ever greater contributor to morbidity and mortality in the region. The second reason to establish injury prevention programs is that injuries impact significantly on health care and societal costs. In the United States, injuries imposed a $180 billion burden on the economy in 1988 (Rice et al. Epidemiologic Transition An epidemiologic transition occurs as countries move from a disease pattern dominated by infectious diseases to one characterized by noncommunicable diseases such as heart disease, cancer, and injury (Omram, 1971). Epidemiologic transition from infectious to noncommunicable diseases increases the relative importance of injuries compared with infectious disease. For instance, in Mexico the proportion of deaths from infectious diseases decreased from 43 percent to 17 percent during the 25-year period from 1955 to 1980. During this same time, the proportion of deaths resulting from unintentional injury increased from 4 percent to 11 percent. In Nigeria, the proportion of deaths from traffic accidents compared with the number of deaths from 16 common infectious diseases increased from 38. In addition to a shift in the relative importance of injuries, demographic changes, technological changes, and social changes affect the epidemiology of injuries and influence the absolute importance of injury as an epidemiologic category. Changing demographics, produced by improved child survival, elevate the proportion of older persons in a population, so that injuries such as occupational injuries and falls may become more important. Countries such as Thailand, Egypt, and Indonesia are experiencing increased numbers of deaths because of occupational injuries, especially those related to manufacturing. Technological changes, such as greater use of the automobile, local manufacturing, and rural electrification can also produce increases in the absolute numbers and rate of injuries. In Nigeria the number of road traffic fatalities more than doubled in seven years, and the rate of motor vehicle fatalities per 10,000 motor vehicles increased 127 percent in only 10 years (Asogawa, 1978). Similar increases have been seen in other developing countries and are obviously related to the rapid introduction of motor vehicles (see Figure 8-1).
Finally, while 66 percent of Sub-Saharan African women are recorded as having some kind of prenatal care, only 38 percent of all births are attended by health facility personnel, the lowest such figure in all the developing regions. Community studies show that most maternal deaths occur outside the medical system, either at home or on the way to the hospital (Thaddeus and Maine, 1990). In response, the provision of access to high-quality emergency obstetric care is gaining recognition as the most important strategy for preventing maternal deaths in the region, in Africa, and in other developing countries where maternal mortality rates are high (Prevention of Maternal Mortality Network, 1995). Access Bias A severe limitation on access is urban-rural bias, which is extreme in Sub-Saharan Africa. According to selected household surveys, of the individuals who report themselves as sick, those in urban areas obtain medical care more often than those in rural areas, and the wealthy contact a care provider more often than the poor. As for bias from other factors, there is no persuasive evidence that Sub-Saharan African females are at any significant disadvantage in being taken for clinical care in their early years. Surveys of the management of diarrheal disease, fever, and respiratory illness in infants and very young children, for example, reveal no significant differences in treatment by sex in the six African countries surveyed (Boerma et al. Nevertheless, gender bias in health services access and utilization accrues with age, as time, money, distance, and fear of stigma become matters of concern for girls and women. Data refer to a variety of years, generally no more than two years before the year specified. Nursing persons include auxiliary nurses, as well as paraprofessional personnel such as traditional birth attendants. Refers to births recorded where a recognized health service worker was in attendance. Sub-Saharan women resort to various home remedies, over-the-counter and prescription pharmaceuticals, and medicines purchased from traditional healers. These resources are used serially or concurrently in different combinations and sequences; selecting among them is a complex process based on habit, cost, perception of risk or urgency, familiarity, and ease of access. The general perspective is that traditional and modern health systems are not seen as in conflict, but rather as two different, but valid, roads to recovery. At the same time, traditional healers in Africa have only rarely "straddled" the two systems in the same way Ayurvedic practitioners do in parts of Asia, and their patients rarely receive whatever benefits modern medicine may confer (Caldwell and Caldwell, 1993). Although understanding this process and the behaviors associated with it would seem to be valuable to the design of preventive and curative interventions, there has been little systematic field research in the Sub-Saharan region into the ways females of different ages and educational histories manage their armamentarium of preventive and curative strategies across the spectrum of health problems and across the life span. One hypothesis suggested by this still uneven body of research is that women may be most likely to attempt to access the modern medical system in connection with illness in a very young child, and least likely to do so when there is a potential for some kind of stigma-for example, for family planning services, diagnosis and treatment of either sexually transmitted diseases or tropical infectious diseases that seem to be sexually transmitted (for example, urinary schistosomiasis), or conditions that might have social repercussions if disclosed (such as leprosy). The Dynamics of Female Education the World Development Report is unequivocal on the centrality of education in human health, stating flatly that "Households with more education enjoy better health, both for adults and for children, [a result that] is strikingly consistent in a great number of studies, despite differences in research methods, time periods, and population samples" (World Bank, 1993). The weight of the literature is toward a clear association between low levels of maternal education and increased child mortality (Cleland, 1990; Elo, 1992; Harrison, 1986). This seems to be particularly true for female children, especially when they are disvalued by the larger society. Data for 13 African countries between 1975 and 1985 show that an increase of just 10 percent in female literacy rates reduced child mortality by an equivalent 10 percent, whereas changes in male literacy had little influence (Hobcraft, 1993). To take a specific country case, a calculation has been made for Kenya that 2 maternal deaths and about 45 infant deaths would be averted for every 1,000 girls provided with one extra year of primary schooling (World Bank, 1993). There is broad general agreement on the major dimensions of the advantages of female education for household health. Female education increases knowledge about the importance of health and health care. It enhances access to income and the capacity and willingness to pay for health care, and is frequently correlated with access to such health-enhancing services as improved household water supplies. Better-educated women marry and start their families later, diminishing the risks associated with early pregnancies, and they tend to make greater use of prenatal care and delivery assistance and to produce fewer low-birthweight babies (Harrison, 1986; Hobcraft, 1993; Kennedy, 1992). Children of educated mothers enjoy such health-enhancing advantages as better food and domestic hygiene and more immunization, which in different ways reduce risk of infection. Mothers with more schooling also tend to be more effective in regimen compliance, use of health technologies, and overall case management (Vlassoff and Bonilla, 1994). Data from Ethiopia, for example, indicate that, regardless of whether or not abortion deaths were included in the calculation, illiterate women still suffered the most mortality (Kwast et al.
With the exception of systemic glucocorticoids, the above-described therapies have not been associated withanysignificantfetalcomplications. Alternative therapies include inhaled cromolyn sodium, leukotriene receptor antagonists, or sustained-release theophylline. Acute severe exacerbations must be treated aggressivelywithoxygentherapy,intravenous fluids, systemic glucocorticoids, administration of short-acting2-agonistsandipratropiumbynebulized aerosol,andantibioticsifthereisevidenceofbacterial infection. Toprevent fetal hypoxia, pulse oximetry should be used and oxygen saturation should be maintained at 95% or greater. Some patients may require endotracheal intubation and mechanicalventilationtomaintainanadequateoxygen supply. Serial fetal monitoring and ultrasonic assessment of fetal growth should be implemented. When pregnancy is progressing well, thereisnoneedforearlydelivery,anditisadvisableto await the spontaneous onset of labor. Early delivery can be considered for fetal growth restriction or maternal deterioration. Management of Labor and Delivery Labor and delivery are usually not triggers of acute asthma attacks. Glucocorticoid therapy, including inhaled or high-potency topical use for more than 3 weeks,maysuppressthehypothalamic-pituitary-adrenalaxis,andadministrationofstressdosesofmedicationduringlaborordeliveryshouldbeconsidered. An epidural block during labor reduces pain, anxiety, hyperventilation, and respiratory effort, all of which are known to aggravate the disease. Prostaglandins should not be used, because they are likely to trigger acute bronchoconstriction. Becauseofimprovementsindiagnosisandtreatment,the majority of females with cystic fibrosis now survive to adulthood. It is the most severe form of obstructive lung disease observed during pregnancy, but there is no evidence that pregnancy increases the maternal risk, unless there is severe disease with pulmonary hypertension. Women with pulmonary hypertension should be counseled about the greater risk that pregnancy poses for an adverse maternal, fetal, or neonatal outcome. Exocrinepancreaticinsufficiencyispresentinabout90%ofpatients,andscreening for diabetes (if not already diagnosed) should be undertaken early in pregnancy. Women with malabsorption symptoms might become more emaciated duringpregnancy,andtherearerisksofsuperimposed infections. Central Nervous System Disease In the majority of cases, seizure frequency does not change in pregnancy. Valproic acid should probably not be used in a woman planning a pregnancy,unlessotherdrugs have proven ineffective. The neural tube closes approximately 4 weeks postconception, before many women realize they are pregnant. Thosetakingvalproicacidorcarbamazepineshouldbe prescribed 4mg/day of folic acid for 1 to 3 months preconceptionandthroughthefirsttrimester. Antacids and antihistamines should be avoided in patients receiving phenytoin, because they lower plasma levels of phenytoin and mayprecipitateaseizureattack. After blood is drawn for plasma levels of anticonvulsants, intravenous lorazepam should be given slowly, followed by a loading dose of phenytoin with continuous cardiac monitoring. During labor and in the immediate postpartum period, anticonvulsant drugs must be continued. The dose of the anticonvulsant drug maybeloweredpostpartum,providedthatatherapeuticlevelismaintained. Although anticonvulsants are excreted in breast milk in small amounts, breastfeeding is not contraindicated. Complications Pregnant patients with epilepsy have a twofold increase in maternal complications such as preeclampsia, abruption, hyperemesis, and premature labor. Fetal hypoxia is a potential consequence of maternal seizures, and there is a high incidence of intrauterine fetal demise. Duringthisperiod,therisksofteratogenesis and miscarriage are much lower than in the first trimester,andtheriskofpretermlaborislowerthanin the third trimester. Precautions must be taken to avoid maternal hypotension and hypoxia that have adverse effects on uteroplacental blood flow.
References:




